Live Hospice Discharge of Individuals with Cognitive Disabilities: A Systematic Review
Victoria M. Winogora, Christine E. DeForge, Kimberlee Grier, Patricia W. Stone

TL;DR
This review finds that people with cognitive disabilities are more likely to be discharged from hospice while still alive, suggesting potential disparities in hospice care quality.
Contribution
This is the first systematic review focusing on live hospice discharge for individuals with cognitive disabilities.
Findings
Cognitive disability was associated with live hospice discharge in all included studies.
Individuals with cognitive disabilities had longer hospice lengths of stay.
Risk factors included female sex, minoritized race, for-profit hospice ownership, and home-based hospice services.
Abstract
To systematically review the evidence on live hospice discharge for individuals with cognitive disabilities. Systematic Review Adults with cognitive disabilities enrolled in hospice in the United States Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we searched for United States-based (US), English-language, and peer-reviewed literature focused on live discharges from hospice for individuals with cognitive disabilities. We searched PubMed, CINHAL, and Web of Science for articles published between January 1, 2014, through August 1, 2024. We used the Joanna Briggs Institute Analytical Cross-Sectional Studies Appraisal Tool to assess study quality. After screening 1,543 titles and abstracts, we completed a full text review of 30 articles, of which 8 met inclusion criteria. All included studies were cross-sectional analyses. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
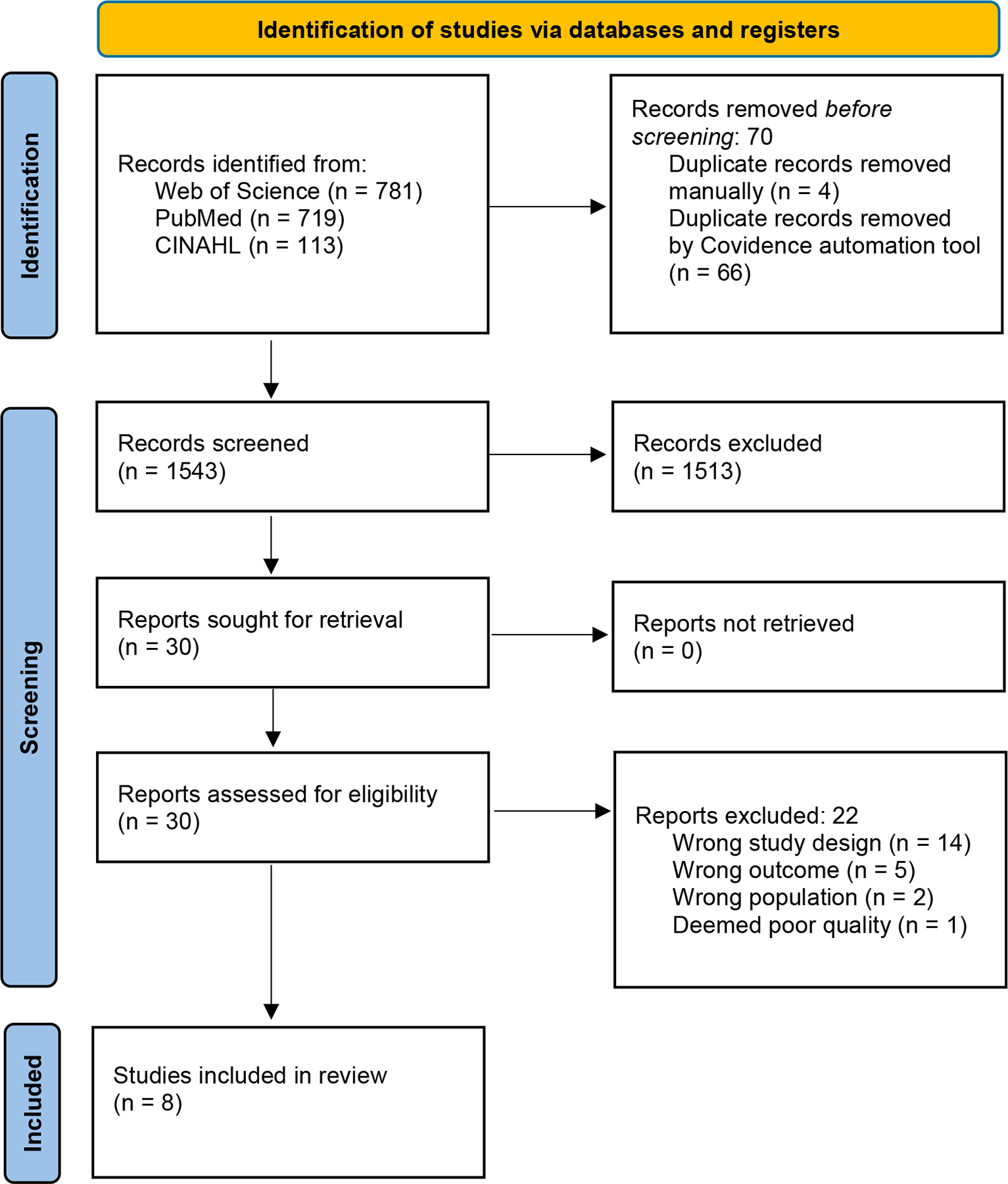 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Geriatric Care and Nursing Homes · Frailty in Older Adults
Introduction
Cognitive disabilities are defined as serious difficulty concentrating, learning new things, remembering, or making decisions.^1,2^ These disabilities are commonly associated with several diagnoses (i.e., Alzheimer’s disease and related dementias [ADRDs], stroke, traumatic brain injuries, intellectual and developmental disabilities).^1^ Except in the context of ADRDs, individuals with cognitive disabilities are commonly underrepresented in end-of-life research for a variety of reasons.^2–4^ Even among individuals with ADRDs, under-detection and/or late diagnosis can contribute to their underrepresentation.^5^ For example, it has been estimated that 41% of Medicare decedents have dementia, yet using data from 2022, the Centers for Medicare and Medicaid Services reported only 11.1% having an official diagnosis of ADRDs.^3,6,7^ This difference may be because nearly half of patients with ADRDs are not diagnosed until the later stages, suggesting that use of ADRDs diagnostic codes in research may result in unintentionally excluding a large segment of the population with cognitive disabilities.^5,8^ Other contributing factors, including ethical considerations and medical mistrust, influence research participation for other individuals with cognitive disabilities, including those resulting from intellectual and developmental disabilities.^9^ Using the term cognitive disability in research better captures this population, who are vulnerable to poor/sub-optimal end-of-life outcomes.^10–12^
One and a half million Medicare beneficiaries annually use hospice care, a specialized service available to individuals near end-of-life (i.e., with a terminal condition and < 6-month prognosis.,^13–15^ Data describing hospice use among individuals with cognitive disabilities broadly speaking is lacking; much more is known about hospice use among those with ADRDs. Roughly 20% of individuals who enroll in hospice are diagnosed with ADRDs.^14,15^ Researchers have found that individuals with ADRDs are less likely to enroll in hospice in the last month of life compared to individuals without ADRDs.^16^ Little is known about end-of-life care for individuals with intellectual and developmental disabilities; however data from small qualitative studies demonstrate that these populations are accessing palliative and end-of-life care.^10–12,17^ Given that hospice is considered best practice for end-of-life care, because it minimizes unwanted treatments and improves quality of life near end-of-life, it is essential to understand barriers to high-quality hospice care for this vulnerable population.^18–20^
Disparities in hospice access and care quality (e.g., length of stay) for individuals with cognitive disabilities have been identified in recent literature.^11,12,21,22^ Concurrently, a troubling trend of increased live discharge from hospice for individuals with ADRDs has emerged.^13,14,23,24^ Live hospice discharge is defined as termination of hospice benefits and discharge of a patient from hospice services prior to the patient’s death, that is, while the patient is alive.^13,14,23,24^ Data from the National Home and Hospice Care Survey found that between 6% and 15% of hospice patients experience live discharge.^25^ Live discharge from hospice can happen for a variety of reasons (e.g., patient/family preferences to pursue life-prolonging treatment and/or hospital admissions); however, the concern is that, for individuals with cognitive disabilities, live discharge often happens when a patient has outlived their hospice prognosis (i.e., > 6 months) and therefore the benefit is terminated. Roughly 20% of all hospice patients are discharged alive, and comorbid dementia diagnosis places an individual at increased odds of live discharge.^7,14,23,26^ Qualitative researchers have described the detrimental impacts of live discharge on patients and families, resulting in poor end-of-life care quality and suboptimal bereavement outcomes.^13,14,27,28^
Because individuals with cognitive disability are at risk for sub-optimal end-of-life care,^12,29,30^ an understanding of current hospice care practices among this group, specifically live discharge and factors influencing live discharge, is essential. Thus, the purpose of this systematic review is to synthesize the evidence on live hospice discharge for individuals with cognitive disabilities, including factors influencing differences in live hospice discharge (e.g., patient characteristics and hospice agency characteristics).
Methods
We developed and registered an a priori protocol (PROSPERO CRD42024571021) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for the conduct and reporting of this review. A comprehensive search strategy was developed (Supplemental Methods) in consultation with a research librarian and used to search the following databases from January 1, 2014, through August 1, 2024: PubMed, CINAHL, and Web of Science. We excluded studies published prior to 2014 due to the Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014, which systematized audits of hospices with high proportion of long stays, directly impacting the federal regulations surrounding hospice care.^31^ Studies meeting inclusion criteria: 1) included both observational and interventional studies; 2) were conducted in the US to limit differences across geographic and health care system contexts (e.g., health care and cultural variations to end-of-life care); 3) were published in peer-reviewed journals in English; 4) included adult (>18 years of age) patients enrolled in hospice care; 5) included patients with a cognitive disability (i.e., diagnosis of dementia, stroke, brain injuries, intellectual or developmental disability or evaluated to have cognitive impairment at the time of hospice care delivery); and 6) examined live discharge from hospice care. We excluded studies that 1) were qualitative, due to the nature of the review question; 2) included in-hospital (general inpatient) hospice due to Medicare requirement that these encounters are short-term; 3) were written in a language other than English; 4) were conducted outside the US; 5) did not include individuals with cognitive disabilities; 6) did not assess hospice care; and 7) did not assess live discharge from hospice care.
Article Screening
All identified records were uploaded into Covidence^32^, which was used for duplicate removal and to manage review workflow. All team members reviewed a subset (n =15) of titles/abstracts together to establish consistency between reviewers. Two reviewers (VMW, PWS) then independently screened the remaining titles/abstracts for eligibility and full texts of potentially eligible records. Discrepancies were resolved through team discussion.
Critical Appraisal of Study Quality
As only cross-sectional studies were included in this review the Joanna Briggs Institute Analytical Cross-Sectional Studies Tool (see Supplemental Materials) was used to assess study quality; each quality criterion was categorized as Yes, No, Unclear or Not Applicable.^33^ Each item response coded as “yes” was scored as one point and “no,” “unclear,” and “not applicable” was scored as zero, yielding a total score, with higher scores indicating higher quality. To standardize assessments across studies, overall quality was calculated as the proportion of “yes” responses to the total number of items in the study designs checklist. We deemed studies earning < 50% of Joanna Briggs Institute elements to be at high risk of bias (i.e., low quality). Two reviewers independently assessed study quality. Discrepancies in quality assessments were discussed by reviewers and, additional team members were enlisted if needed to reach consensus. If low quality studies were found, we excluded them from data synthesis.
Data Extraction
Two independent reviewers extracted data from each included study, using a standardized data extraction form, which was pilot tested prior to use. We extracted the following data: article citation, study aims, study outcomes, inclusion criteria including how cognitive disability was identified, exclusion criteria, data source, sample size, dates of data collection, study location, statistical analysis method utilized, covariates, patient demographics (e.g., race, sex, age, socioeconomic status, primary hospice diagnosis, and comorbidities), hospice level data (e.g., geographic location, urbanicity, and ownership), and hospice quality data (e.g., nurse visits and hospice quality rating). Discrepancies in extracted data were resolved through team discussion.
Data Synthesis
Study data were synthesized using tables to facilitate comparisons. We grouped studies by participant diagnoses, sex, setting, and location. Tables were created to facilitate comparisons across studies. This method was selected to allow for comprehensiveness. As consistencies began to appear across studies, major findings were put onto tables for ease of perception.
Results
The initial search yielded 1,543 records after removing duplicates; 30 full article texts were assessed for eligibility and 8 studies ultimately met criteria for inclusion (Figure 1). A complete list of excluded studies with justification is provided in the Supplement/Appendix.
Quality Appraisal
Table 1 in the Supplemental Materials shows the results from the quality appraisal conducted for this review. Six of the eight studies included in this review scored 100% on Joanna Briggs Institute appraisal.^13,14,22,24,34,35^ Two of the studies^7,23^ were assessed as unclear in two elements: 1) was the exposure measured in a valid and reliable were way? and 2) were objective, standard criteria used for measurement of the condition? Both studies^7,23^ were scored at an 80%, and upon discussion were determined to be suitable for inclusion.
Study Characteristics
Table 1 presents the characteristics of the included studies. All the studies involved secondary data analyses. The studies were published in 2017,^34^ 2018,^22^ 2020,^23^ 2021,^24^ 2022,^7,14^ and 2023.^13,35^ There were variations in location and types of hospices included in the analyses. In relation to geographical variation, authors of 3 studies looked at single hospice providers in New York City (NYC),^23,24,34^ whereas 5 looked at national hospice data.^7,13,14,22,35^ Samples ranged in size from 2,629^23^ to 2,195,076.^13^ The drastic difference in range is explained by three of studies with smaller sample sizes that used data from single hospice agencies in NYC,^23,24,34^ and one group that used data from the Health and Retirement Study.^7^ In the studies with larger sample sizes, researchers used data from national data sources.^13,14,22,35^ In three studies, investigators calculated mean age,^7,23,24^ which ranged from 82.8^7^ to 89.8 years of age.^23^ For all the studies included in this review, investigators included sex and race; and in every study, females outnumbered males, with the range being 58%^34^ to 72.2%^24^ female. Race was broken down into categories. Black non-Hispanic subjects ranged from 6.7%^14^ to 16.1%^32^ of total participants. Hispanic subjects ranged from 1.7%^13^ to 21%^24^ of total participants. In 6 studies, researchers focused on patients with dementia,^7,14,22–24,35^ whereas 2 looked at live discharges more generally, and conducted subset analyses on individuals with dementia.^13,34^
Measurement of Cognitive Disability
In five studies, investigators used ICD-9/ICD-10 codes to determine cognitive disabilities (i.e. ADRDs).^13,14,22,34,35^ In another study, the investigators also used ICD-9/ICD-10 codes for patients with primary diagnoses of ADRDs, and a probability score of > 0.5 for patients they determined had comorbid dementia.^7^ In two studies investigators used electronic medical record data (i.e., cognitive assessments) to determine if a patient had dementia.^23,24^
Six studies looked at individuals with primary hospice diagnoses of dementia versus individuals with other primary hospice diagnoses.^7,22–24,34^ Russell and peers (2017) compared individuals with a primary hospice diagnosis of dementia versus those with cancer, heart failure, stroke, and pulmonary disease.^34^ Lastly, Gianattasio and peers (2023) compared individuals with a primary hospice diagnosis of dementia to those with lung cancer.^13^
Other Factors Assessed for Association with Live Discharge
In four studies researchers assessed the relationship between race and ethnic minority status and live hospice discharge.^7,14,34,35^ Sex was assessed in four of the included studies.^7,14,22,34^ Location of hospice delivery was assessed in two of the included studies.^23,24^ In four studies, investigators examined the for-profit status of the involved hospice agencies.^13,14,22,35^ Lastly, in two studies researchers described the impact of registered nurse visits on live hospice discharge.^23,24^
Study Findings
Following death, live discharge is the second most common outcome for individuals with cognitive disabilities receiving hospice care.^14,22,24,24,34^ In two studies, researchers found that live hospice discharge occurred in the context of condition stabilization, acute hospitalization, transfer or service move, and elective revocation.^23,34^ In six studies, researchers found that individuals with ADRDs experienced live discharge at increased rates compared to individuals with alternative primary hospice diagnoses, such as cancers, heart failure, stoke, and pulmonary disease.^7,13,22–24,34^ In these six studies, the authors found that the percentage of live discharge for individuals with cognitive disabilities ranged from 21%^24^ to 45%.^7^ In all (n=8) studies, researchers found that individuals with indicators of cognitive disabilities had longer lengths of stay in hospice. Authors of all studies included in this review (n = 8) reported that prolonged length of stay is associated with live discharge in individuals with an indicator of cognitive disabilities. Two additional elements were of particular interest:
Patient-Level Factors Other than Cognitive Disability Were Associated with Live Discharge. Table 2 presents factors associated with live discharge across studies. Demographic factors other than cognitive disability that were associated with live discharge included minoritized race or ethnicity^7,14,34,35^ and female sex.^7,14,22,34^ Further, minoritized race was found to be a risk factor for live discharge (both in national^14,35^ and NYC samples)^23,24^ in addition to female sex (also both in a NYC sample^34^ and national samples).^7,14,22^Hospice-Level Factors Were Associated with Live Discharge. Hospices in the lower quartile of quality ratings (as measured by the Consumer Assessment of Healthcare Providers and Systems survey for hospice), and those that were for-profit hospices were identified as risk factors for live hospice discharge for patients.^13,14,22,35^ Hunt and colleagues (2022) found no significant regional variation in relation to live hospice discharge for patients with dementia.^14^ Other hospice level factors identified with live discharge included hospice care delivery in the home setting,^23,24^ and greater time between registered nurse visits.^23,24^ Specifically, in two single-agency (NYC; non-profit) studies, researchers found that live discharge risk increased as the number of days between nurse visits increased.^23,24^
Discussion
To our knowledge, this is the first systematic review assessing live hospice discharge among individuals with cognitive disabilities. The authors of the research synthesized did not use the term “cognitive disability.” Nevertheless, in all the research synthesized we found that the indicator of cognitive disability was associated with increased likelihood of live discharge compared to those with other diagnoses (i.e., cancer, pulmonary diseases, heart failure), which warrants further exploration.^7,13,34^ We identified patient-level risk factors for live discharge (i.e., female sex, racial and ethnic minority, and prolonged length of stay).^14,22,23,34,35^ Furthermore, we found that live discharge was associated with hospice ownership, location of hospice care delivery, and geographic location.^13,22–24,35^
Other researchers have conducted systematic reviews of live discharges from hospice specifically in ADRDs patients.^15^ We expanded upon this work by synthesizing findings relating to both patient-level (e.g., diagnosis, location of care, race/ethnicity, sex) and organizational factors (e.g. ownership, geographic location, quality) associated with live discharge from hospice and including diagnoses other than ADRDs.
In a qualitative study, researchers found that live discharge is distressing to patients and families and results in suboptimal hospice outcomes (i.e. poor symptom control, acute care hospitalizations).^28^ Identifying the patient level factors associated with live discharge provides direction for future research, both to explore reasons behind these differences and also to develop interventions to avoid live discharge for these specific groups.
In the included studies, researchers found that 21%^24^ to 45%^7^ of individuals with cognitive disabilities experienced live discharge compared to 6% to 15% for the general hospice population. These data demonstrate the significant increased risk of live discharge that this population experiences and the importance of future research aimed at reducing this risk.
Researchers have found that geographic location (i.e., distance to and concentration of healthcare facilities) in the US is associated with access to care (i.e. hospice facilities, nurse visitations, and hospitals) as well as variation in population races/ethnicities, and socioeconomic status.^36^ This finding is vital for researchers to understand, as for-profit hospice ownership rose from one-third in 2000 to over two-thirds by 2020.^37^ Many hospice acquisitions have been funded through private equity.^37^ In 2021, 14% of Medicare hospice patients received care from private equity-owned hospices.^38^ Growth in for-profit hospice ownership has been substantial; however, these agencies offer narrower range of services,^39,40^ provide fewer community benefits (i.e. charity care),^39,40^ care for more lower acuity patients,^41^ have higher rates of hospital and emergency department use,^42^ and receive more deficiency citations.^22,39–45^ This systematic review adds to the body of evidence demonstrating significant differences in clinical outcomes by hospice ownership (i.e., increased risk of live hospice discharge for patients with cognitive disabilities serviced by for-profit hospice agencies), identifying three studies that showed these associations.^13,22,35^ More research is also warranted to explore differences in organizational factors, especially private equity ownership and live discharge from hospice.
None of the included studies address if individuals with cognitive disabilities enter hospice with lower mortality risk, so it is not possible to conclude if this contributes to the increased rate of live discharge among this population. However, a study that looked at hospice re-enrollment after live discharge found no significant association between diagnosis, functional score at admission or change between admission and discharge, and mortality within six months after live hospice discharge, suggesting that differences in live discharge may not be related to functional status or mortality risk.^46^ Further exploration on the factors that place individuals with cognitive disabilities at increased risk of live hospice discharge is therefore warranted.
Literature on hospice re-enrollment following live discharge is limited, however a single retrospective study conducted by LeSage and peers (2014) found that only 31% of general population patients who were discharged alive from hospice re-enrolled.^47^ These authors did not include ADRDs (or other cognitive disabilities) as a primary hospice diagnosis in their analyses, therefore conclusions related to the cognitive disability population cannot be drawn. However, it is worth noting that the authors found that 40% of patients died within 6 months of live discharge, suggesting that these patients actually had ongoing hospice eligibility at the time of their deaths.^47^ Further research is warranted to examine if disparities exist in hospice reenrollment following live discharge for patients with cognitive disabilities.
This review identified additional gaps and future possible research opportunities. There were no interventional studies found in our literature search, and all the studies of patients with cognitive disability focused on patients with ADRDs. Given their vulnerability to poor end-oflife outcomes, patients with cognitive disability (e.g., more broadly speaking, specifically in the context of intellectual and developmental disabilities) should be included in future work. As investigators learn more about disparate hospice care among this group, research should move towards intervention development to minimize suboptimal hospice care/end-of-life outcomes for those with cognitive disabilities. Of note, none of the studies in this review followed patients for prolonged periods of time after live discharge. It is vital that researchers explore what happens to patients with cognitive disabilities after live discharge to determine what meaningful interventions this population wants and needs regarding hospice care.
To summarize, the population of individuals with cognitive disabilities is increasing the US, and as they age, there will be subsequent growth in the number of those accessing hospice care. Individuals with cognitive disability experience disparate access and care quality in many aspects of their medical care,^21,48–51^ however data on their hospice use is limited. This review summarized the evidence to date and demonstrated a need for enhanced understanding of outcomes and potential hospice care disparities among this population.^10,12,21^ While we sought to find research that included patients with a variety of cognitive disabilities, this aim proved to be more difficult than anticipated. The vast majority of the data focused on individuals with ADRDs. In the future, it would be beneficial to have data on individuals with other forms of cognitive disabilities, such as intellectual and developmental disabilities and acquired brain injuries as these populations are at increased risk of adverse end-of-life outcomes. Investigators conducting hospice research should also consider assessing in-hospital death, where many acquired brain injuries (i.e., traumatic brain injury and stroke) deaths occur. Additionally, future research should include work targeting individuals with intellectual and developmental disabilities as this group was not readily identified in studies included in our review. Our hope is in the future to involve individuals directly impacted by this work as stakeholders and collaborators, because as the saying goes, “nothing about us, without us.”^52^
Limitations
While we conducted a systematic search, we may have missed some published articles. We had justification for excluding studies prior to 2014 but may have excluded data relevant to our research question. We restricted our search to deaths outside of the hospital, which may have failed to capture studies of individuals with cognitive disability who died in the hospital following hospice care. Our definition of cognitive disabilities was intended to be comprehensive but was developed by our research team and could have resulted in exclusion of other studies of relevant populations. Further, our inclusion of only adult patients limits our evidence synthesis given that a large subset of patients with intellectual and developmental disabilities are pediatric patients who potentially qualify for/access hospice care. All the studies we identified focused on individuals with ADRDs, thus generalizability to the larger cognitive disability community is limited. Furthermore, our search was limited to the US, which limits generalizability to other countries.
Conclusions and Implications
Hospice disparities, including live discharge from hospice, are a fact for individuals with cognitive disabilities, one such example is live discharge from hospice. As the population of individuals with cognitive disabilities in the US continues to grow, it is vital that researchers explore the underlying etiology of live discharges, to best understand the problem, and to find solutions to address it. In reducing live discharges from hospice for individuals with cognitive disabilities we can ensure equitable end-of-life care for vulnerable populations, reduce healthcare spending, and prevent patient and caregiver duress.
Supplementary Material
1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Consumer and Governmental Affairs Bureau. Individuals with Cognitive Disabilities: Barriers to and Solutions for Accessible Information and Communication Technologies. Federal Communications Commission; 2016:1–37. Accessed December 14, 2023. https://docs.fcc.gov/public/attachments/DOC-341628 A 1.pdf
- 2DHDS. Centers for Disease Control and Prevention, National Center of Birth Defects and Developmental Disabilities, Division of Human Development and Disability. Disability and Health Data System (DHDS) Data. Published online December 18, 2024. Accessed March 15, 2024. https://www.cdc.gov/dhds/datasets/index.html
- 3HHS. Cognitive Impairment: A Call for Action, Now! U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2011:1–4. https://www.cdc.gov/aging/pdf/cognitive_impairment/cogimp_poilicy_final.pdf
- 4Schalock RL, Luckasson R, TasséMJ. An Overview of Intellectual Disability: Definition, Diagnosis, Classification, and Systems of Supports (12th ed.). American Journal on Intellectual and Developmental Disabilities. 2021;126(6):439–442. doi:10.1352/1944-7558-126.6.43934700345 · doi ↗ · pubmed ↗
- 5Chen Y, Power MC, Grodstein F, Correlates of missed or late versus timely diagnosis of dementia in healthcare settings. Alzheimer’s & Dementia. Published online June 27, 2024:alz.14067. doi:10.1002/alz.14067 PMC 1135002838934297 · doi ↗ · pubmed ↗
- 6CMS. Centers for Medicare & Medicaid Services. Chronic Conditions Data Warehouse: Alzheimer’s Disease Disparities in Medicare Fee-For-Service Beneficiaries. Published online January 2022. https://www 2.ccwdata.org/web/guest/medicare-tables-reports
- 7Aldridge MD, Hunt L, Husain M, Li L, Kelley A. Impact of Comorbid Dementia on Patterns of Hospice Use. Journal of Palliative Medicine. 2022;25(3):396–404. doi:10.1089/jpm.2021.005534665050 PMC 8968839 · doi ↗ · pubmed ↗
- 8Bradford A, Kunik ME, Schulz P, Williams SP, Singh H. Missed and Delayed Diagnosis of Dementia in Primary Care: Prevalence and Contributing Factors. Alzheimer Disease & Associated Disorders. 2009;23(4):306–314. doi:10.1097/WAD.0b 013e 3181 a 6bebc 19568149 PMC 2787842 · doi ↗ · pubmed ↗