Feasibility of Utilizing Spot-Scanning Proton Arc (SPArc) for Whole-Lung Irradiation: A Case Report
Peilin Liu, Lewei Zhao, Gang Liu, Xi Cao, An Qin, Di Yan, Xiaoqiang Li, Craig Stevens, Rohan Deraniyagala, Xuanfeng Ding

TL;DR
This case report explores a new proton therapy technique for lung cancer treatment that better protects the heart and reduces overall body dose.
Contribution
The study introduces and evaluates the feasibility of Spot-scanning Proton Arc (SPArc) therapy for whole-lung irradiation in a pediatric patient.
Findings
SPArc reduced mean heart dose to 5.41 Gy compared to 8.48 Gy with IMPT and 9.56 Gy with VMAT.
SPArc had a lower integral body dose (98 Gy·L) compared to VMAT (137 Gy·L) and IMPT (189 Gy·L).
SPArc demonstrated improved delivery efficiency compared to IMPT and VMAT.
Abstract
Photon radiotherapy is the conventional method in the treatment of bilateral whole-lung metastasis. However, uncertainties, longer delivery times, large lateral penumbra, and motion interplay limit intensity-modulated proton therapy (IMPT)’s use in bilateral lung metastases. To overcome such limitations in IMPT, this study explores the feasibility of using a novel proton therapy technique, Spot-scanning Proton Arc (SPArc) therapy, to improve the dose sparing to the heart and other healthy tissue for this pediatric patient compared to the volumetric modulated arc therapy (VMAT) and IMPT. A 13-year-old patient with a malignant neoplasm of bone and articular cartilage, presenting with bilateral whole-lung metastasis, received whole-lung irradiation of 15 Gy in 10 fractions using VMAT. For comparative analysis, plans were generated using IMPT and SPArc. The study showed that SPArc was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
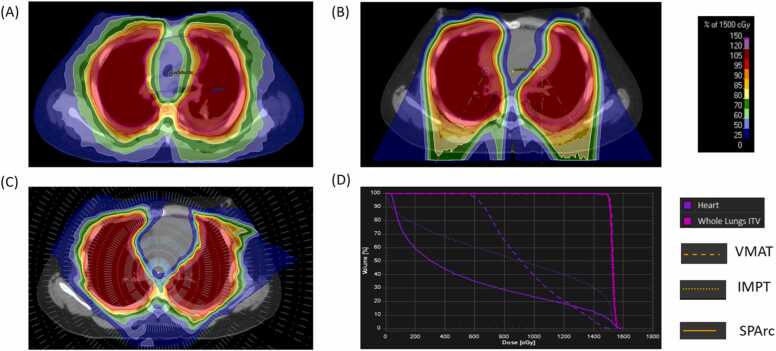 Figure 1
Figure 1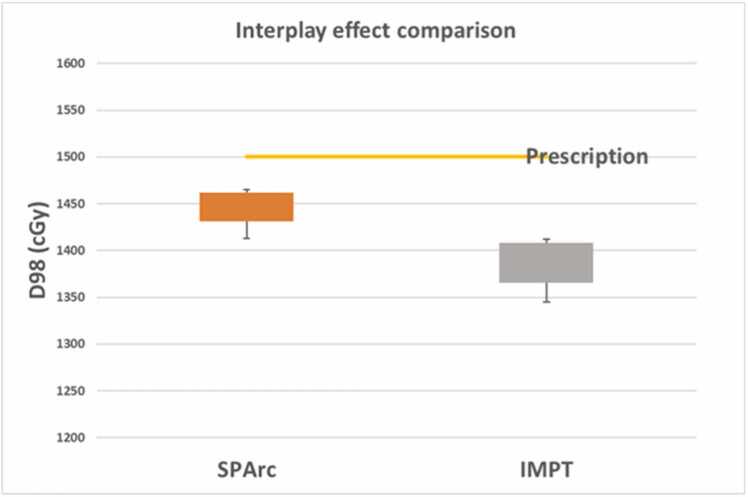 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiation Therapy and Dosimetry · Advanced Radiotherapy Techniques · Renal and related cancers
Introduction
Whole lung irradiation (WLI) is pivotal in treating pulmonary metastasis in pediatric patients.1, 2 The 5-year overall survival with and without WLI was 61% and 49%, respectively.3, 4 WLI significantly improves local control of lung disease and leads to a trend toward better progression-free survival.5 The overall survival rate and relapse-free survival are 78% and 72% in children with favorable histology tumors in the National Wilms Tumor study-3.6 However, radiation therapy, particularly to the heart, can lead to a range of complications impacting the pericardium, myocardium, endocardium, cardiac valves, conduction system, and coronary arteries.4, 7, 8 These cardiovascular disorders are a leading cause of premature mortality among long-term cancer survivors.1 The 20-year congestive heart failure rate in the National Wilms Tumor was 4.4% after initial treatment and 17.4% after the first or subsequent relapse.4 Further, a study of 4122 French-British cancer survivors, monitored for a median of 26 years, revealed that the adjusted relative risk of cardiac mortality was significantly elevated (RR 7.4) after receiving heart radiation doses exceeding 5 Gy. This study was among the first to establish a link between low to intermediate cardiac doses (5-15 Gy) and increased cardiovascular mortality in childhood cancer survivors.8 Thus, potential cardiac toxicity from WLI must be acknowledged, and improved radiation techniques are highly desirable.9
Proton therapy’s physical properties enable significant dose reduction to surrounding normal tissues, a benefit particularly relevant for children.10 Recently, spot-scanning proton arc (SPArc) therapy was introduced into radiation oncology as a concept in 2016, allowing gantry rotation while delivering proton spots and switching energies.11, 12 The previous investigation reported significant improvement in the dosimetric outcome in various clinical indications such as lung,13 breast,14 prostate,15 head and neck cancers.16 This is the first study to investigate the feasibility of utilizing such a novel treatment technique in WLI for a pediatric patient with bilateral pulmonary metastasis through the dosimetric comparison, treatment delivery, and interplay effect simulation.
Materials and methods
Case description of clinical details and treatment modalities
This study, approved by the Institutional Review Board, analyzed patient data from the Department of Radiation Oncology at William Beaumont Hospital. The patient, a 13-year-old teenager diagnosed in April 2021 with malignant bone and articular cartilage neoplasm and bilateral whole-lung metastasis (Figure 1A), had their personal information anonymized. In June 2021, the patient underwent 15 Gy of WLI in 10 fractions with volumetric modulated arc therapy (VMAT).Figure 1. The SPArc versus IMPT and VMAT treatment plan. (A) SPArc plan dose, (B) IMPT plan dose, (C) VMAT plan dose, and (D) DVH comparison. Abbreviations: DVH, dose-volume histogram; IMPT, intensity-modulated proton therapy; SPArc, spot-scanning proton arc therapy; and VMAT, volumetric modulated arc therapy.Figure 1
The lung internal target volume was defined as 1919.75 cm³, encompassing the maximum lung expansion volume on 4D computed tomography simulation scans.1 Given the substantial size of the target, VMAT delivered a considerable dose to both the heart and the overall body. To evaluate alternatives, IMPT and SPArc plans were generated.
Treatment planning and dosimetric plan quality comparison
For the clinical VMAT plan, 3 full arcs utilizing a 6 MV beam from the Elekta Versa HDTM were employed. The IMPT plan (Figure 1B) was generated using a dual-isocenter and 4 treatment fields with the single field optimization in the RayStation (Stockholm, Sweden). The SPArc plan was generated through a published in-house developed optimization algorithm and implemented in RayStation through scripting.12 SPArc employed a full 360-degree arc trajectory at 2.5-degree intervals from a single isocenter (Figure 1C).
Both IMPT and SPArc plans incorporated the same robustness settings (±5 mm setup, ±3.5% range) and used 3 mm dose grids. Each plan delivered 15 Gy in 10 fractions, requiring at least 98% of the internal target volume to receive the full prescription. Comparative evaluations, including heart dose-volume histograms and integral body dose assessments in VMAT, IMPT, and SPArc nominal plans.
Delivery time calculation
The delivery efficiency for both IMPT and SPArc was simulated using a previously published machine delivery sequence model for the IBA ProteusONE machine.17 The VMAT delivery time was obtained from the LINAC machine’s log file.
Interplay effect evaluation
A 4D computed tomography data set comprising 10 phase images was utilized to simulate a 4-second patient breathing cycle. The interplay effect was evaluated using a 4D dynamic dose accumulation approach.18 For each treatment fraction, the dynamic dose calculation involved accumulating the dose from each phase image onto the reference phase (50%) using deformable image registration. The D98 metric was used to assess target coverage.
Results
Result of diagnostic assessment
As illustrated in Figure 1, the patient's SPArc plan was evaluated alongside the IMPT and VMAT plans, with their respective optimized parameters detailed in Table 1. Notably, SPArc's total monitor units were lower than IMPT's, although SPArc utilized a slightly higher number of energy layers and spots.Table 1. Optimized plan parameters comparison.Table 1. PlanNumber of energy layersNumber of spotsTotal MUsVMATNot applicableNot applicable721IMPT11924 7434050SPArc13427 4073822Abbreviations: MU, monitor unit; VMAT, volumetric modulated arc therapy; IMPT, intensity-modulated proton therapy; SPArc, spot-scanning proton arc.
Result of dose metrics comparison
SPArc demonstrated a notable reduction in dose to healthy tissue compared to IMPT and VMAT, while maintaining comparable coverage of clinical target volumes (Table 2). Specifically, the mean heart dose in the SPArc plan was 5.41 Gy, significantly lower than 8.48 Gy in IMPT and 9.56 Gy in VMAT. In terms of D50 (the dose received by at least 50% of the heart's volume), SPArc achieved 3.06 Gy, substantially less than IMPT's 9.13 Gy and VMAT's 9.12 cGy. Furthermore, the integral body dose was remarkedly reduced in SPArc (98 Gy·L) compared to VMAT (136 Gy·L) and IMPT (112 Gy·L).Table 2. Dose metrics statistics and delivery time comparison among VMAT, IMPT, and SPArc.Table 2. Comparison indexVMATIMPTSPArcITVMax dose (cGy)159416231599Mean dose (cGy)160015261530D98 (cGy)149415001500HeartMax dose (cGy)154115961595Mean dose (cGy)956848541D50 (cGy)912913306Body-integral dose (Gy·L)13611298Irradiation timesa (s)N/A746973Total delivery timeb (s)3171046985Abbreviations: VMAT, volumetric modulated arc therapy; IMPT, intensity-modulated proton therapy; SPArc, spot-scanning proton arc; ITV, internal target volume.aThe irradiation time for proton beam therapy includes the delivery of all the spot and energy layer at a fixed-beam angle. It includes spot drill time, spot-scanning time, energy layer switching time, and burst to switch time.bTotal delivery time includes the irradiation time, the estimated iso shift workflow, imaging verification time,14 as well as the gantry rotation time.
Result of delivery efficiency comparison
The LINAC log file indicated that VMAT completed its 3-arc delivery in 317 seconds. In comparison, the total IMPT treatment delivery for WLI is approximately 1046 seconds. Conversely, SPArc achieves dynamic arc delivery in a total time of 985 seconds.17 This represents a 5.83% reduction in treatment delivery time compared to the 4-field IMPT approach.
Result of interplay effect evaluation
SPArc achieved a mean D98 dose of 14.45 ± 0.19 Gy, surpassing the 13.85 ± 0.26 Gy achieved by IMPT (Figure 2). Statistically, SPArc demonstrated superior target coverage compared to IMPT, as indicated by a significant difference in a t test (P value < .01).Figure 2. Comparison of interplay effect between SPArc and IMPT. Abbreviations: IMPT, intensity-modulated proton therapy; SPArc, spot-scanning proton arc therapy.Figure 2
Discussion
A fundamental principle of radiation therapy is to minimize the dose to nontarget normal tissues, which is critical to pediatric patients. The tumor rarely invades the heart in children with lung metastasis. However, it is unavoidable during WLI because of its anatomic proximity to the lungs.4, 19, 20, 21 Such complicated geometry makes conventional radiation therapy less effective in cardiac structure sparing. Thus, we reported a first feasibility study of utilizing a novel treatment technique, SPArc, for such a challenging case who received WLI in our institution. The result demonstrated a significant heart dose and body-integral dose sparing compared to VMAT, multifield IMPT, and SPArc. The study found that SPArc also reduces the patient’s total body-integral dose. Such dosimetric improvement has the potential to reduce normal tissue complications such as cardiac mobility22 and secondary malignancy,23 which is critical to childhood cancer survivors. Additionally, the study found that the demonstrated treatment efficiency of SPArc could be comparable to that of IMPT. Furthermore, this case study indicated that SPArc was able to mitigate the intrafractionation motion uncertainties, which agrees with the previous finding in the mobile target treatment such as advanced staged and early-stage non–small cell lung cancer treatment.24 These findings indicated that free-breathing conditions with a 4D scan could provide sufficient plan robustness in terms of the target coverage in the SPArc WLI. However, this is a case study. More patient data are needed to provide more concrete data and evidence to support the recommendation.
Conclusion
SPArc technique in whole-lung irradiation offers substantial dosimetric benefits over VMAT and IMPT, particularly in reducing cardiac and overall body exposure. Additionally, SPArc simplifies the clinical workflow and effectively manages the interplay effect compared to IMPT.
Ethics
The study is approved by IRB 2017-455, and consent is waived by the participant.
Author Contributions
Conceptualization: X.D., R.D.; Data curation: P.L.,L.Z.,G.L., X.D.; Formal analysis: P.L., L.Z.; Investigation: P.L., L.Z.,G.L.,X.C., A.Q.,D.Y.,C.S., R.D., X.L., X.D.; Methodology: X.D., P.L.,L.Z.,G.L.; Supervision: X.D., R.D., C.S.; Writing: P.L., L.Z.,G.L.,X.C.,X.D.
Declaration of Conflicts of Interest
The authors declare the following financial interests/personal relationships, which may be considered as potential competing interests: Xuanfeng Ding reports that financial support was provided by Ion Beam Applications SA. Xuanfeng Ding reports that financial support was provided by Corewell Health William Beaumont University Hospital. Xuanfeng Ding reports a relationship with Ion Beam Applications SA that includes speaking and lecture fees. Xuanfeng Ding has a patent licensed to Ion Beam Application SA. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Suzuki G.Ogata T.Aibe N.Effective heart-sparing whole lung irradiation using volumetric modulated arc therapy: a case report J Med Case Rep 1312019277–27710.1186/s 13256-019-2209-2PMC 671797731474226 · doi ↗ · pubmed ↗
- 2Spunt S.L.Mc Carville M.B.Kun L.E.Selective use of whole-lung irradiation for patients with Ewing sarcoma family tumors and pulmonary metastases at the time of diagnosis J Pediatr Hematol/Oncol 232200193981121671310.1097/00043426-200102000-00005 · doi ↗ · pubmed ↗
- 3Nicolin G.Taylor R.Baughan C.Outcome after pulmonary radiotherapy in Wilms’ tumor patients with pulmonary metastases at diagnosis: a UK Children’s Cancer Study Group, Wilms’ Tumour Working Group Study Int J Radiat Oncol Biol Phys 70120081751801798050610.1016/j.ijrobp.2007.05.053 · doi ↗ · pubmed ↗
- 4Kalapurakal J.A.Zhang Y.Kepka A.Cardiac-sparing whole lung IMRT in children with lung metastasis Int J Radiat Oncol Biol Phys 85320137617672281841310.1016/j.ijrobp.2012.05.036 · doi ↗ · pubmed ↗
- 5Scobioala S.Ranft A.Wolters H.Impact of whole lung irradiation on survival outcome in patients with lung relapsed Ewing sarcoma Int J Radiat Oncol Biol Phys 102320185845923024487910.1016/j.ijrobp.2018.06.032 · doi ↗ · pubmed ↗
- 6D’angio G.J.Breslow N.Beckwith J.B.Treatment of Wilms’ tumor. Results of the third national Wilms’ tumor study Cancer 6421989349360254424910.1002/1097-0142(19890715)64:2<349::aid-cncr 2820640202>3.0.co;2-q · doi ↗ · pubmed ↗
- 7Pein F.Sakiroglu O.Dahan M.Cardiac abnormalities 15 years and more after adriamycin therapy in 229 childhood survivors of a solid tumour at the Institut Gustave Roussy Br J Cancer 911200437441516214210.1038/sj.bjc.6601904 PMC 2364747 · doi ↗ · pubmed ↗
- 8Tukenova M.Guibout C.Oberlin O.Role of cancer treatment in long-term overall and cardiovascular mortality after childhood cancer J Clin Oncol 2882010130813152014260310.1200/JCO.2008.20.2267 · doi ↗ · pubmed ↗