A case of culture-proven cutaneous atypical mycobacterial infection caused by Mycobacterium immunogenum
Faraz Yousefian, Aysham Chaudry, Francesca Ceci, Charay Jennings-Dover, Dionne Louis

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1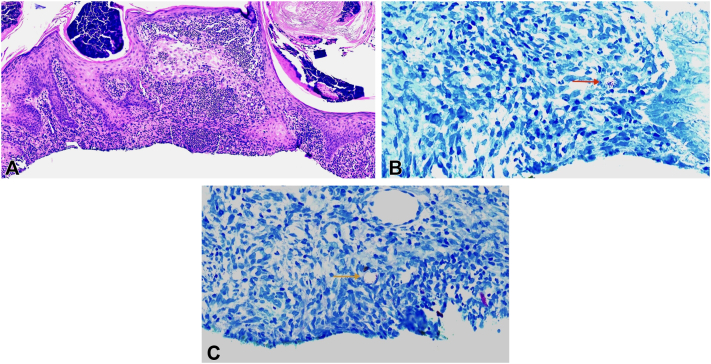 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Mycology · Tuberculosis Research and Epidemiology
Introduction
Mycobacterium immunogenum is an atypical, rapidly growing mycobacterium related to the M chelonae-M abscessus group. Infection with this pathogen can cause a variety of clinical manifestations, with cutaneous involvement being particularly common. Cutaneous infections include folliculitis, ulceration due to exposure to contaminated water, and postsurgical and postinjection skin infections.1 Additionally, M immunogenum may also present as erythematous papules, nodules, and plaques, often following invasive procedures.2, 3, 4, 5 Beyond the skin, it is most commonly implicated in hypersensitivity pneumonitis, associated with metalworking fluids.There have also been reports of keratitis, tenosynovitis, and cerebral abscess caused by the pathogen.1 Here we present a case of cutaneous nontuberculous atypical mycobacterial infection caused by M immunogenum in a patient with no identifiable risk factors, highlighting an unusual presentation of this pathogen.
Case presentation
A 73-year-old Caucasian female with a past medical history of coronary artery disease, chronic kidney dysfunction, hyperlipidemia, and diabetes presented to our outpatient dermatology clinic for easy bruising of the upper and lower extremities for 2 years. She denied any past medical or family history of bleeding and autoimmune disorders. Review of systems was noncontributory. She denied any recent travel, recent trauma, or sick contacts. Her current medications included amlodipine, aspirin, chlorthalidone, ezetimibe, and empagliflozin.
Physical examination revealed violaceous patches on bilateral upper and lower extremities, which were consistent with senile purpura. Additionally, two 1 centimeter nontender nodules were incidentally found on the upper arm (Fig 1). Two punch biopsies of the nodules revealed suppurative and granulomatous dermatitis that was suggestive of an infection by atypical mycobacteria (Fig 2, A). Consequently, two acid-fast bacilli cultures and Fite stains were performed from the biopsy tissue with eventual confirmation and identification of M immunogenum (Fig 2, B and C). Serum testing for HIV was negative. The patient was referred to infectious disease and started on a regimen of intravenous amikacin, intravenous omadacycline, and oral azithromycin with initial improvement of the lesions within 2 months (Fig 3). The patient then developed hearing and vision problems secondary to amikacin, at which point the medication was discontinued. The patient was then started on linezolid but developed diarrhea and mild abdominal pain and this was also discontinued. Currently, the patient is tolerating oral azithromycin 500 mg and oral omadacycline 300 mg with a slow improvement of the lesions. The patient has been advised to continue the current regimen for a total duration of 12 months.Fig 1. Physical examination revealing violaceous patches distributed on left upper extremity and two 1 cm nontender nodules on the upper arms.Fig 2. Microscopic results. A, A hematoxylin & eosin (H&E) stain (100×) demonstrates a suppurative and granulomatous inflammatory pattern with overlying hyperkeratotic crust, epidermal hyperplasia, a mixed inflammatory infiltrate of histiocytes, neutrophils, and lymphocytes. B, An acid-fast bacillus stain (400×). C, Fite stain (400×) both demonstrate clusters of intracellular and extracellular acid-fast bacilli (arrows).Fig 3. Physical examination revealing improvement on left upper extremity post-treatment.
Discussion
M immunogenum is a recently discovered pathogen that shares phenotypic and genotypic characteristics with M chelonae and M abscessus. They are rapidly growing, atypical mycobacteria that commonly cause waterborne nosocomial outbreaks and hypersensitivity pneumonitis associated with metalworking fluid due to their ability to create biofilms.1 Like these atypical mycobacteria, M immunogenum has also been reported to cause hypersensitivity pneumonitis in association with metalworking fluid. There have also been reports of keratitis, tenosynovitis, and cerebral abscess with M immunogenum infection.2^,^4
There has been an increasing incidence of cutaneous nontuberculous mycobacterial infection caused by M immunogenum (Table I). Majority of these cases have been described in the postprocedural setting or in the setting of immunosuppression. In one study, 28 patients developed skin lesions at the injection site after mesotherapy.5 There have been at least two cases of postsurgical wound infection caused by surgical material contamination. There was also a case of a tattoo infection caused by a contaminated tattoo reservoir.4 One case report describes disseminated infection from M immunogenum in the setting of immunosuppression in a renal transplant patient with cutaneous manifestations.6 Other reported cases include skin ulceration with exposure to contaminated water and a single case of folliculitis.3^,^4 Our case differs because this patient did not have any invasive surgeries or injections prior to disease manifestation. The patient also did not have any known risk factors such as exposure to contaminated water or immunosuppression. Only one other case has been described that is similar to ours, with presentation of erythematous papules and pustules of the abdomen and successful treatment with clarithromycin.4Table ICases of M immunogenumInfection settingDescriptionPostprocedural28 patients developed skin lesions at the injection site following mesotherapySurgical material contaminationTwo cases of postsurgical wound infections due to contaminated surgical materialTattoo infectionOne case of a tattoo infection linked to a contaminated tattoo ink reservoirImmunosuppressionOne case of disseminated infection in an immunosuppressed renal transplant patient with cutaneous manifestationsContaminated water exposureSkin ulceration following exposure to contaminated waterFolliculitisSingle reported case of folliculitis associated with M immunogenum exposure
Treatment of M immunogenum is challenging due to the lack of clinical guidelines or a standardized approach for treatment attributed to ill-defined antimicrobial susceptibility patterns. Previously discussed cases were treated largely with clarithromycin and a possible addition of a fluoroquinolone or amikacin with successful resolution of lesions.4 Although limited, some information regarding susceptibility patterns exists and can be used to guide management until susceptibilities become available.7 Further research and a standardized approach to treatment are warranted to address the challenges posed by newly discovered bacterial species like M immunogenum in guiding medical management effectively.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wilson R.W.Steingrube V.A.Böttger E.C.Mycobacterium immunogenum sp. nov., a novel species related to Mycobacterium abscessus and associated with clinical disease, pseudo-outbreaks and contaminated metalworking fluids: an international cooperative study on mycobacterial taxonomy Int J Syst Evol Microbiol 51520011751176410.1099/00207713-51-5-175111594606 · doi ↗ · pubmed ↗
- 2Okinaka T.Fujimura K.Hamasaki Y.Hasegawa Y.Matono T.Significance of early diagnosis and surgical management in treating Mycobacterium immunogenum-related pyogenic extensor tenosynovitis: a case report BMC Infect Dis 24202439510.1186/s 12879-024-09249-538609847 PMC 11010399 · doi ↗ · pubmed ↗
- 3Mc Neil E.P.Goldfarb N.Hannon G.R.Miller D.D.Farah R.S.Mycobacterium immunogenum folliculitis on the lower extremities of a healthy young adult Clin Exp Dermatol 443201932833010.1111/ced.1370329920742 · doi ↗ · pubmed ↗
- 4Garcia-Zamora E.Sanz-Robles H.Elosua-Gonzalez M.Rodriguez-Vasquez Lopez-Estebaranz J.L.Cutaneous infection due to Mycobacterium immunogenum: an European case report and review of the literature Dermatol Online J 231020171410.5070/D 3231003699229469779 · doi ↗ · pubmed ↗
- 5Del-Castillo M.Palmero D.Lopez B.Mesotherapy-associated outbreak caused by Mycobacterium immunogenum Emerg Infect Dis 152200935735910.3201/eid 1502.08112519193300 · doi ↗ · pubmed ↗
- 6Biggs H.M.Chudgar S.M.Pfeiffer C.D.Rice K.R.Zaas A.K.Wolfe C.R.Disseminated Mycobacterium immunogenum infection presenting with septic shock and skin lesions in a renal transplant recipient Transpl Infect Dis 144201241542110.1111/j.1399-3062.2012.00730.x 22548769 · doi ↗ · pubmed ↗
- 7Hunkins J.J.de-Moura V.C.N.Eddy J.J.Daley C.L.Khare R.In vitro susceptibility patterns for rapidly growing nontuberculous mycobacteria in the United States Diagn Microbiol Infect Dis 1053202311588210.1016/j.diagmicrobio.2022.11588236610383 · doi ↗ · pubmed ↗