Illness and treatment beliefs in Kathmandu valley Nepalis under hypertensive care
Deepak S. Shrestha, Andrea M. Straus, Ram Kishor Sah, Hari Har Khanal, Roshani Gautam, Bishnu Dutta Paudel, Talea M. Cornelius, Richard R. Love

TL;DR
This study explores how Nepalis in Kathmandu understand and manage hypertension, highlighting the need for culturally tailored patient education.
Contribution
The study identifies unique Nepali beliefs about hypertension that differ from Western perspectives, suggesting a need for localized patient communication strategies.
Findings
Patients reported experiencing multiple physical and emotional symptoms linked to hypertension.
Concerns about long-term medication effects and dependency were common among participants.
There is a belief that successful blood pressure control might allow a return to natural remedies or no treatment.
Abstract
The prevalence of actionable (i.e., stage 2 = BP > 140/90) hypertension among Nepalis approaches one-third in the adult population. Long-term drug treatment adherence is low. Western-developed assessment tools present an incomplete picture of the regional Nepali beliefs that guide patient treatment adherence, and the present study seeks to substantiate qualitative findings that suggest a reorientation of patient education content for more effective patient-oriented, culturally consonant care. We conducted a cross-sectional structured interview of 500 men and women under treatment for hypertension in three urban Kathmandu hospital clinics. Interview items were developed from a qualitative survey and investigated patient beliefs about hypertension causes, symptoms, and consequences; treatment costs and sequelae; and general health maintenance. Patients reported experiencing multiple and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
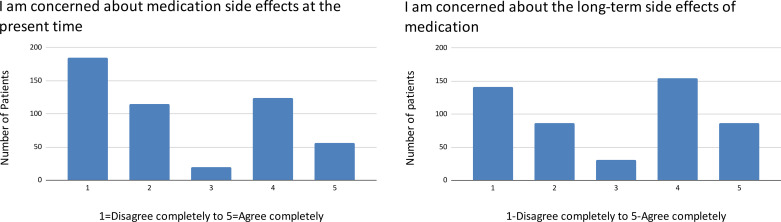 Fig 1
Fig 1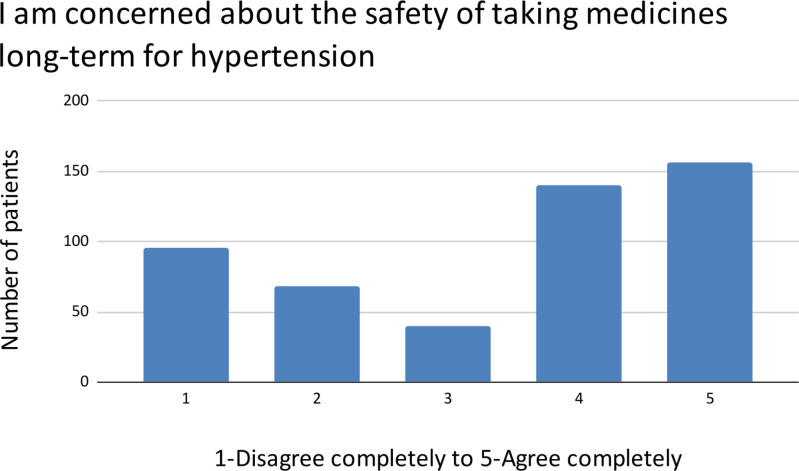 Fig 2
Fig 2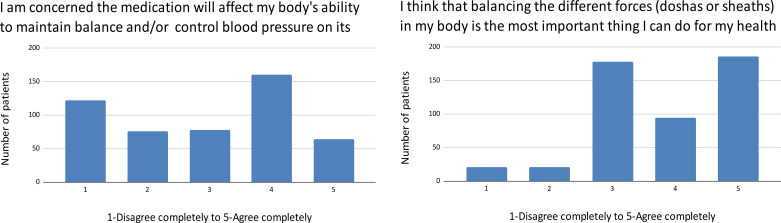 Fig 3
Fig 3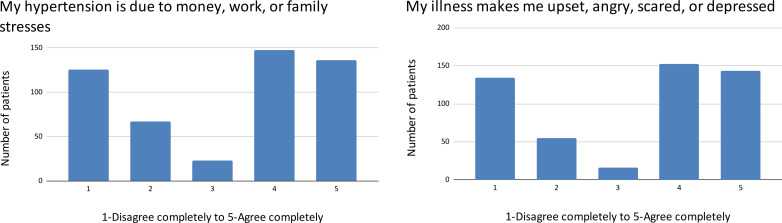 Fig 4
Fig 4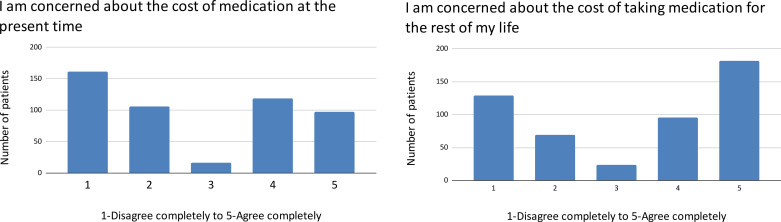 Fig 5
Fig 5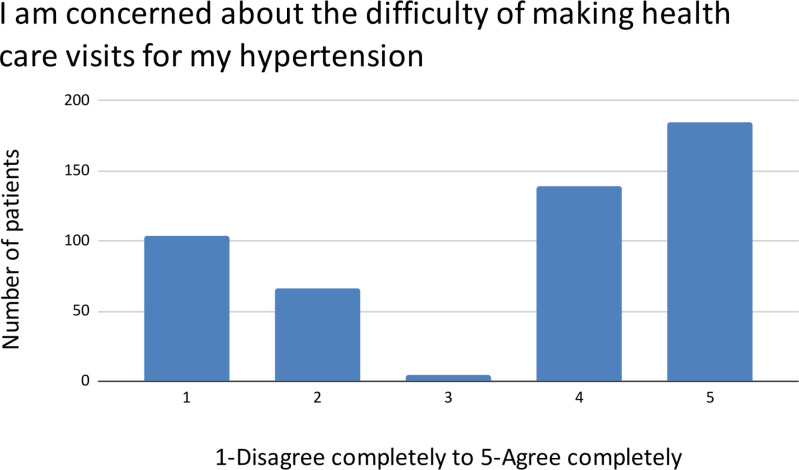 Fig 6
Fig 6- —Prof. Richard R. Love
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmaceutical Practices and Patient Outcomes · Medication Adherence and Compliance · Global Maternal and Child Health
Introduction
The prevalence of actionable, i.e., stage 2 = BP > 140/90, hypertension among Nepalis approaches one-third in the adult population and may be increasing [1–5]. Despite the availability of effective and inexpensive drugs, long-term treatment adherence is poor and population reductions in the morbidity and mortality associated with hypertension are not being observed [5,6]. Nonadherence to hypertensive drug treatment was found to be approximately 50% at the time of assessment in two Nepalese studies, consistent with what is believed to be a challenging problem worldwide [7–9]. A Cochrane Report on treatment adherence suggested that there have been limited insights in recent years into this major issue [10]. In particular, there are limited data about the role of cultural models and social determinants in treatment adherence despite their significance for behavioral medicine [11].
Previously, the investigators conducted an exploratory study of patients under treatment for hypertension in the outpatient clinic of a tertiary-care institution in Kathmandu [12]. Hypertension was identified as having multiple, widely varying symptoms by 42 of the 50 patients interviewed, including behavioral and affective elements. It was also identified as a serious disease like other noncommunicable conditions. There were frequent expressions of concern about long-term medication as well as barriers to treatment. Patients appeared to be influenced by the holistic Ayurvedic and Yoga frameworks that emphasize wellness maintenance rather than “…the suppression of sickness with life-long consumption of drugs” [13]. Yoga practices and theory are part of school curricula and Ayurvedic medicine is a licensed mainstream practice that identifies illness as an imbalance in the basic forces underlying body, mind, and behavior. It emphasizes as well that long-term use of medicine will impair the body’s ability to maintain, in this case, blood pressure. [13,14]. We conducted observational cross-sectional interviews in a larger population to confirm these qualitative themes that suggest how we might adapt Western-developed patient communications to address Nepali misconceptions in the context of Nepali experience.
Methods
Ethics statement
This study was approved by the Ethics Committee of the Nepal Health Research Council I.D. # 622/ 2020 P on November 10, 2020, and subsequently by the Institutional Review Board at Marquette University in the United States. Additional information regarding the ethical, cultural, and scientific considerations specific to inclusivity in global research is included in the supporting information S1 Checklist. Formal written consent was obtained from all respondents.
Study protocol
Observational cross-sectional interviews were conducted with 500 clinic patients over 18 years old who self-identified as hypertensive. No other exclusion criteria were employed. Interview items were developed from the themes and language identified in the English translations of our earlier qualitative investigation of Nepali beliefs about hypertension and its treatment [12], consistent with the phenomenological approach of our investigations. The interview instrument was translated into Nepali by the Nepali researchers relying on patient phrasing from the qualitative study, then back translated to English. In the absence of any knowledge about how beliefs may cluster in subgroups of this culturally diverse city, we chose a large sample.
Male and female interviewers were trained in structured interview technique as well as Leventhal’s “Common-Sense Model of Self-Regulation” (CSM), a widely used theoretical framework describing the dynamic process by which patients become aware of an illness, formulate an image of the threat and potential treatment, adopt action plans for addressing the threat, and integrate feedback on treatment efficacy and illness progression [15]. The interviewers did not present themselves as clinicians to avoid the impression that they were evaluating patients on their recall of doctor communications rather than their own beliefs.
Interviews were conducted at three hospital outpatient clinics with services provided self-pay (Table 1) from 05-04-2021 till 27-04-2021. Two are government facilities drawing from a diverse national population, although the majority of patients are from the Kathmandu Valley: The referral center Shahid Gangalal National Heart Center, Bansbari, Kathmandu and the tertiary facility National Academy of Medical Sciences’ Bir Hospital, Kathmandu. The third site, the Lalitpur Heart Clinic, Lalitpur, Kathmandu Valley, is a private clinic with somewhat higher fees and a more local catchment area.
Table 1: Patient demographics.
In the outpatient clinics of these institutions, individuals who self-identified as hypertensive patients were recruited with a financial incentive of 600 rupees NPR, a little under $5.00 USD. Recruitment included description of the study protocol and duration, as well as assurance that participation would not delay their visit and nonparticipation would have no effect on clinic services. Ten percent of eligible male and female individuals declined study participation. Written informed consent was obtained from 268 male and 232 female participants. Interviews were conducted in Nepali in quiet private rooms and lasted approximately 30 minutes. Care was taken to avoid interfering with the clinic visit and standardized assessment tools were not included to curtail interview time. Following a brief set of open questions, patients indicated agreement with questionnaire items using a graphic 5-point bimodal Likert scale presented with instructions appropriate for literate and illiterate respondents. The complete interview schedule is provided in the supporting S1 file Protocol. Subjects’ demographic information and response record were entered into a computer database in English with the file identified by number only.
Patient responses were summarized by measures of central tendency and dispersion appropriate to their distribution. Using SAS, an analysis of K-means clustering was employed to identify naturally occurring groupings of these beliefs, and Pearson product-moment correlations with pair-wise deletions were conducted between items indexing concerns with disease and its treatment.
Results
The interviewed patient sample (N = 500) is described in Table 1. The majority of patients came from the public hospitals that served the general Kathmandu Valley population, while 18% came from the more expensive private clinic. The preponderance of male respondents and the mean age of 57.1% were not unexpected in a sample of hypertensive patients as was the language mix. While patients were asked about a subset of comorbidities, other conditions were also volunteered.
Patients reported that hypertension not only affected their physical well-being, but also their emotions and their behavior (Table 2). Less than 10% reported that they could not tell when their blood pressure was high and those who reported being symptomatic had an average of 5.3 symptoms.
Table 2: Signs of high blood pressure reported by patients (N = 500).
Many symptoms are ones associated with stage 3 hypertension [16] including the two most commonly reported, headache and dizziness or fainting, but also heart palpitations, tingling sensations in arms or legs, blurred vision or flashes of light, fearfulness or panic, shortness of breath, gastritis or nausea, tinnitus, feeling confused or disoriented, and ear pain. Other symptoms appeared less associated with high blood pressure in the medical literature, most prominently aggressive behavior, the third most common symptom, but also fatigue or lethargy, sweating, insomnia, restlessness, body pain, unhappiness or depression, shivering, slurred speech or numb tongue and even paralysis.
Majorities of patients rated high agreement with statements that they were symptomatic at diagnosis, that their high blood pressure had symptoms, and that they could tell when their blood pressure was high. A majority also reported that treatment should affect their symptoms although they pursued treatment to prevent serious future consequences (Table 3).
Table 3: Likert scores of patient health beliefs.
Patient temporal expectations for hypertension and its treatment were also assessed. Patients endorsed the beliefs that both their hypertension and their treatment are life-long and disagreed with medicating only when symptomatic. There was not as much agreement on whether hypertension comes and goes and whether the need for medication could be superseded by natural treatments or life-style change, or even stopped altogether (Table 3).
There is a bimodal distribution of patient concern about immediate and long-term side effects of medication (Fig 1) as well as the long-term safety of medication (Fig 2).
Concerns about medication side effects.
Concerns about long-term medication safety.
The Ayurvedic belief that long-term medication damages the body’s ability to control blood pressure received a spectrum of agreement, while the item employing Ayurvedic and Yoga terminology varied between “Neither Agree or Disagree” and “Agree completely” (Fig 3).
Ayurvedic belief and specific Ayurvedic terminology.
Pearson product-moment correlations were computed for the short- and long-term concerns about side effects and treatment safety as well as barriers to treatment (Table 4). Weak positive correlations are found among these concerns with the following exceptions:
Table 4: Correlations of medication concerns and barriers to treatment.
Short- and long-term concerns about side effects or costs of treatment have strong positive correlations. Both short- and long-term concerns with side effects have moderate positive correlations with the three measures of treatment barriers: short- and long-term costs and difficulties making healthcare visits. Between those three measures, both short- and long-term concerns with treatment costs have a moderate positive correlation with difficulty of healthcare visits.
Beliefs about the role of emotional distress as a cause and a consequence of hypertension produced a bimodal distribution (Fig 4).
Emotional stress and hypertension.
A bimodal distribution is also found in concerns about the treatment barriers of current and future costs (Fig 5) as well as clinic accessibility (Fig 6).
Financial barriers to care.
Treatment barriers.
The cluster analysis did not produce any interpretable patterns or groupings. The complete dataset is provided in S1 Dataset.
Discussion
The wide range and large numbers of symptoms reported may be misattributed manifestations of other conditions, medication side effects, or even symptoms from high levels of hypertension. This divergence from the asymptomatic presentation in Western countries is also consistent with Nepali mainstream Ayurvedic and Yoga illness models, in which disease is a state of imbalance manifested in the whole person: body, mind, and behavior [12,13]. WHO and the American Heart Association emphasize that hypertension is a “silent disease” and promote detection and control in the absence of symptoms [16,17], but this characterization diverges so greatly from our population’s experience that greater consonance and therefore credibility may be achieved by focusing on the need to rely solely on blood pressure readings for assessing treatment effectiveness. This in turn requires access to blood pressure monitoring, if possible through the provision of blood pressure machines to patients themselves. Regular monitoring can demonstrate on the one hand that medication is effective even though “symptoms” are being experienced and on the other that blood pressure may be high in the absence of symptoms.
Patients were concerned that long-term medication would create a dependency or damage the natural ability to control blood pressure. While successful blood pressure control demonstrates the value of treatment to the clinician, it may signal the need to stop for the patient. Care should be taken to explain that treatment must be ongoing because hypertension is life-long and that medication supports the body’s ability to maintain wellness. Although these concerns with long-term treatment are consistent with Ayurvedic science, familiarity with the terms specific to that tradition were not as widespread and the belief should be addressed in colloquial language familiar to a wider population.
Patients also expressed concerns about treatment side effects, safety, and cost. The different treatment concerns have a highly significant weak correlation indicating that these concerns are not limited to a population segment generally anxious or fearful of medication. It is not enough to disseminate information on hypertension’s threats and the effectiveness of treatment - people also need to know that the treatment will be worth the costs, the barriers, and its potential damaging (side) effects. Crucial to this approach is encouraging clinicians to inform patients that side effects can be managed and to elicit and respond to reports of side effects and other treatment concerns.
Such clinical attention could also benefit the majority of patients who reported feeling upset, angry, scared or depressed by their hypertension. This might further be addressed in public health communications in which positive socially known figures who have (controlled) hypertension message that they have a serious disease, but they are calm and confident knowing they have their blood pressure under control with medication and healthy life habits. “I don’t need to worry because I take my medication and monitor my blood pressure.”
Limitations
The data reported here are from Kathmandu Valley self-identified patients under clinical care. These individuals are likely to be better educated with greater financial resources and healthcare access than the majority of Nepalis, who live in ethnically distinct rural areas. Absent widespread screening, clinic consultation is typically scheduled in response to a symptom, therefore our population is more likely to consider themselves symptomatic. All patients were under treatment and thus the role of the observed beliefs in treatment abandonment could not be addressed, nor was patient blood pressure control, the ultimate goal, known.
Conclusion
Kathmandu Valley hypertension beliefs suggest the need to adapt Western-developed patient educational materials to address Nepali patient experience and concerns. Clinical and public health communications that describe hypertension as a “silent” disease contradict the multiple wide-ranging symptoms experienced by our Kathmandu Valley population. Patient education might more profitably focus instead on the greater reliability of sphygmomanometer readings. The life-long need for medication should be clearly attributed to the disease’s nature and not medication habituation or dependence, with message reinforcement as blood pressure is brought under control. Individual clinical intervention should be supported by increasing access to medication and blood pressure monitoring.
The foregoing suggestions for patient-oriented and culturally appropriate public health and clinical communications should be rigorously tested in clinical trials. Similar investigations of patient representations of hypertension should be conducted in Nepal’s regional and rural populations with careful consideration of representative sampling to better guide communications about this condition.
Supporting information
S1 ProtocolInterview Instrument.(DOCX)
S1 ChecklistGlobal ethical, cultural, and scientific inclusivity considerations.(DOCX)
S1 DatasetComplete data set.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hasan M, Sutradhar I, Akter T, Das Gupta R, Joshi H, Haider MR, et al. Prevalence and determinants of hypertension among adult population in Nepal: Data from Nepal Demographic and Health Survey 2016. P Lo S One. 2018;13(5):e 0198028. doi: 10.1371/journal.pone.0198028 29852006 PMC 5978874 · doi ↗ · pubmed ↗
- 2Dhital S, Arjun K. Dealing with the burden of hypertension in Nepal: current status, challenges and health system issues. Reg Heal For. 2013;17:44–52. https://api.semanticscholar.org/Corpus ID:26930267
- 3Society for Local Integrated Development Nepal, Central Bureau of Statistics N. Nepal STEPS noncommunicable disease risk factors survey 2005. Geneva: World Health Organization. 2005.
- 4Sharma SK, Ghimire A, Radhakrishnan J, Thapa L, Shrestha NR, Paudel N, et al. Prevalence of hypertension, obesity, diabetes, and metabolic syndrome in Nepal. Int J Hypertens. 2011;2011:821971. doi: 10.4061/2011/821971 21629873 PMC 3095978 · doi ↗ · pubmed ↗
- 5Institute for Health Metrics and Evaluation. Global burden of disease: Nepal. https://www.healthdata.org/nepal. Accessed 2023 October 1.
- 6Thapa A, KCB, Shakya B, Yadav DK, Lama K, Shrestha R. Changing Epidemiology of Stroke in Nepalese Population. Nep J Neurosci. 2018;15(1):10–8. doi: 10.3126/njn.v 15i 1.20021 · doi ↗
- 7Bhandari B, Bhattarai M, Bhandari M, Ghimire A, Pokharel PK, Morisky DE. Adherence to Antihypertensive Medications: Population Based Follow up in Eastern Nepal. J Nepal Health Res Counc. 2015;13(29):38–42. 26411711 · pubmed ↗
- 8Hossain A. Adherence to Medications among Nepali Hypertensive Population: A Hospital-Based Cross-Sectional Study. BJSTR. 2018;3(5). doi: 10.26717/bjstr.2018.03.000964 · doi ↗