Severe Early-Onset Pulmonary Hypertension in a Six-Month-Old With Down Syndrome and Isolated Secundum Atrial Septal Defect
Fatima Abeer, Aasim Ayaz Wani, Bisma Javid, Aisha Mahmood, Gazala Andleeb

TL;DR
A six-month-old with Down syndrome developed severe pulmonary hypertension from a small heart defect, requiring urgent treatment and highlighting the need for early intervention in such cases.
Contribution
Highlights the atypical progression of secundum ASD to severe PAH in infants with Down syndrome and the effectiveness of early pulmonary vasodilator therapy.
Findings
Infant with Down syndrome developed severe PAH from a rapidly enlarging secundum ASD.
Early treatment with sildenafil and oxygen stabilized the infant within five days.
Emphasizes the importance of early cardiac evaluation and multidisciplinary care in Down syndrome infants with heart defects.
Abstract
Infants with Down syndrome (trisomy 21) commonly present with congenital heart defects and immune dysregulation, significantly increasing the risk of early-onset pulmonary arterial hypertension (PAH). Although secundum atrial septal defects (ASDs) are often considered hemodynamically mild in non-syndromic children, they can progress aggressively in the presence of trisomy 21. We describe a six-month-old male infant with karyotype-confirmed trisomy 21 who developed severe PAH secondary to a rapidly enlarging secundum ASD - a highly atypical presentation for an isolated lesion. The infant presented with fever, respiratory distress, vomiting, and diarrhea, alongside a clinical history of neonatal sepsis, recurrent infections, failure to thrive (weight below the 5th percentile), and subclinical hypothyroidism (TSH 8.12 μIU/mL). Echocardiography revealed that the ASD had enlarged from 6 mm…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
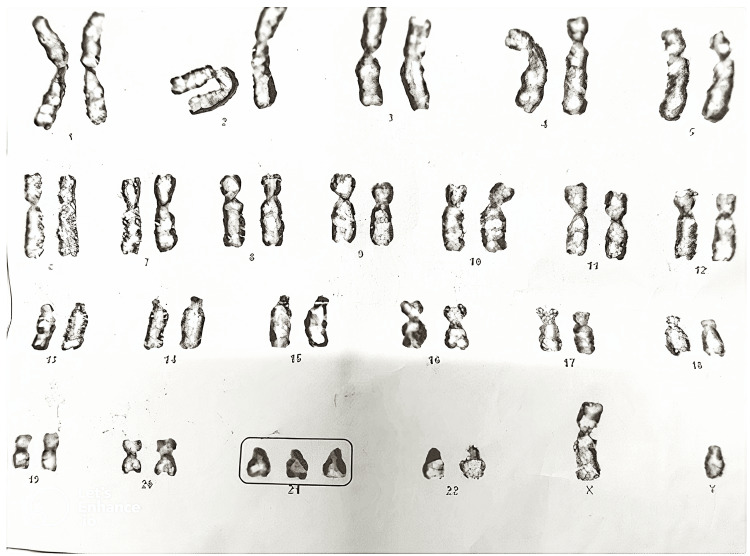 Figure 1
Figure 1| Parameter | Value | Unit | Reference Range | Interpretation |
|---|---|---|---|---|
| WBC | 5.18 | ×10³/μL | 5.0 – 19.5 | Low-normal |
| Neutrophils | 34.1 | % | 20 – 40 | Normal |
| Lymphocytes | 49.4 | % | 40 – 70 | Normal |
| Monocytes | 9.7 | % | 2 – 10 | High-normal |
| Eosinophils | 6.1 | % | 1 – 4 | ↑ Mild eosinophilia |
| Basophils | 0.7 | % | <1 | Normal |
| RBC | 3.79 | ×10⁶/μL | 4.1 – 5.5 | ↓ Anemia |
| Hemoglobin | 9.7 | g/dL | 10.5 – 14.0 | ↓ Mild anemia |
| Hematocrit | 28.6 | % | 32 – 44 | ↓ Low |
| MCV | 75.6 | fL | 70 – 86 | Normal |
| MCH | 25.6 | pg | 23 – 31 | Normal |
| MCHC | 33.9 | g/dL | 30 – 35 | Normal |
| RDW-CV | 19.6 | % | <14.5 | ↑ Anisocytosis |
| Platelet Count | 438 | ×10³/μL | 150 – 400 | ↑ Mild thrombocytosis |
| MPV | 9.1 | fL | 6.5 – 10.5 | Normal |
| Parameter | Value | Unit | Reference Range | Interpretation |
|---|---|---|---|---|
| pH | 7.41 | Unitless | 7.35 – 7.45 | Normal |
| pCO₂ | 40 | mmHg | 35 – 45 | Normal |
| pO₂ | 43 | mmHg | 60 – 100 | ↓ Mild hypoxemia |
| Bicarbonate | 18.0 | mmol/L | 22 – 28 | ↓ Metabolic acidosis |
| BUN | 3.86 | mg/dL | 5 – 18 | ↓ Slightly low |
| Creatinine | 0.39 | mg/dL | 0.3 – 0.7 | Normal |
| Sodium | 143 | mmol/L | 135 – 145 | Normal |
| Potassium | 4.6 | mmol/L | 3.5 – 5.5 | Normal |
| Calcium | 9.5 | mg/dL | 8.5 – 10.5 | Normal |
| Phosphate | 5.0 | mg/dL | 4.5 – 6.7 | Normal |
| Bilirubin (T) | 0.5 | mg/dL | <1.2 | Normal |
| Parameter | Value | Unit | Reference Range | Interpretation |
|---|---|---|---|---|
| Total T3 | 1.78 | ng/mL | 1.05 – 2.45 | Normal |
| Total T4 | 11.78 | μg/dL | 5.92 – 13.06 | Normal |
| TSH | 8.12 | μIU/mL | 0.70 – 6.40 | ↑ Subclinical hypothyroidism |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPulmonary Hypertension Research and Treatments · Congenital Heart Disease Studies · Cardiac Structural Anomalies and Repair
Introduction
Down syndrome (trisomy 21), which occurs in approximately 1 in 700 live births, is well recognized for its strong association with congenital heart defects (CHDs), notably atrial septal defects (ASDs), present in up to half of affected individuals [1]. In typical pediatric populations, secundum ASDs rarely cause significant clinical issues in early infancy. However, Down syndrome-related genetic and immunologic factors place these infants at disproportionately high risk for early-onset pulmonary arterial hypertension (PAH), often within the first year of life [2,3]. This susceptibility is driven by multiple trisomy 21-specific mechanisms, including overexpression of genes such as DYRK1A and RCAN1 (contributing to endothelial dysfunction), alveolar hypoplasia, and an exaggerated hemodynamic response to left-to-right shunts [4-6]. Accordingly, Down syndrome confers a nearly ten-fold increase in the likelihood of developing PAH compared to non-syndromic infants, with early-onset disease carrying a poor prognosis if not identified and treated promptly [4,7].
We describe a rare presentation of severe PAH in a six-month-old infant with Down syndrome and an isolated secundum ASD that expanded from 6 mm to 10 mm over the course of a single month. This rapid progression was accompanied by recurrent infections, including neonatal sepsis, and failure to thrive, culminating in life-threatening respiratory compromise. To our knowledge, this represents one of the earliest documented instances of severe PAH arising from an ostensibly uncomplicated ASD in an infant with Down syndrome, demonstrating the need for vigilant echocardiographic surveillance and timely intervention. We also discuss the potential role of pulmonary vasodilators, specifically sildenafil, as a bridge to surgical closure in medically fragile infants, emphasizing the delicate balance between the benefits of early repair and the risks associated with operating on clinically unstable patients.
Case presentation
Background and neonatal history
A six-month-old male infant, born full-term by cesarean section to non-consanguineous parents, displayed characteristic phenotypic features of Down syndrome (DS) at birth, including hypotonia, upslanting palpebral fissures, a flat facial profile with epicanthic folds, a protruding tongue, and a broad neck. Although karyotyping was pending early on, the clinical diagnosis of trisomy 21 was evident (see Figure 1). His birth weight was 2.8 kg (slightly below average).
The image displays a complete chromosomal complement arranged in pairs from chromosomes 1 to 22, along with sex chromosomes (XY).Notably, there are three copies of chromosome 21 (highlighted in the box), consistent with Trisomy 21 (Down syndrome). This chromosomal abnormality is the most common genetic cause of intellectual disability and is frequently associated with congenital heart defects, hypotonia, characteristic facial features, and increased risk of pulmonary hypertension.
Growth and early morbidities
From the neonatal period, the infant exhibited poor weight gain, weighing only 3.5 kg at six months (<5th percentile for age) and often tiring during feeds. At 17 days of life, he developed omphalitis that progressed to neonatal sepsis, necessitating IV antibiotics and supportive care; no cardiovascular assessments (such as an echocardiogram) were performed at that time. Recurrent mild respiratory infections occurred throughout infancy, though no formal pneumonia diagnosis was made until the current illness.
Presenting illness
In early March 2025, the infant arrived at the pediatric emergency department with one day of high-grade fever (up to 39°C), frequent vomiting, and multiple episodes of watery diarrhea. The mother reported increased work of breathing and poor feeding, with the infant appearing irritable, lethargic, and far less active than usual. There were no recent travel exposures or known tuberculosis contacts. Immunizations were age-appropriate.
Physical examination
On arrival, the infant was febrile (38.5°C), tachypneic (respiratory rate 80-85/min), and tachycardic (heart rate 150/min), with room-air oxygen saturation of 88%. Both his weight (3.5 kg) and length (60 cm) fell below the 5th percentile, confirming failure to thrive. Dysmorphic features consistent with Down syndrome were evident (e.g., flat occiput, single transverse palmar crease), and generalized hypotonia was noted. Respiratory findings included subcostal retractions, nasal flaring, and bibasilar crackles, indicating pneumonia. Cardiovascular examination revealed a hyperdynamic precordium and a right ventricular heave, with a grade 3/6 systolic ejection murmur at the left upper sternal border. The murmur was accompanied by wide, fixed splitting of the second heart sound (S2) - a hallmark of atrial septal defect (ASD) physiology. A loud pulmonic component (P2) of S2 suggested pulmonary hypertension (PH). Mild hepatomegaly (liver 3 cm below the right costal margin) was also detected, likely reflecting right-sided volume overload.
Initial investigations
(a) Routine laboratory tests indicated leukopenia (WBC 4.2×10^9^/L) with a slightly low absolute neutrophil count (~1.5×10^9^/L), moderate anemia (Hb 9.0 g/dL), and a markedly elevated C-reactive protein (CRP) (234 mg/L), suggestive of significant infection or sepsis. Liver enzymes were mildly elevated [Aspartate transaminase (AST) 57 U/L, alanine transaminase (ALT) 105 U/L] without hyperbilirubinemia, compatible with either reactive hepatitis or mild congestive hepatopathy (see Table 1). Blood and urine cultures were negative, presumably due to prompt antibiotic administration. A stool sample was negative for common bacterial pathogens. (b) Thyroid function tests showed a thyroid-stimulating hormone (TSH) of 8.12 μIU/mL with normal free T4 - diagnostic of subclinical hypothyroidism (a recognized comorbidity in Down syndrome). Given the infant’s acute condition and normal T4, endocrine follow-up was planned rather than immediate hormone replacement. (c) Chest radiography demonstrated bilateral perihilar infiltrates (consistent with bronchopneumonia), along with cardiomegaly and a prominent pulmonary artery segment - raising suspicion of a significant cardiac shunt and pulmonary hypertension (see Table 2).
Cardiac evaluation
An urgent transthoracic echocardiogram revealed a 10 mm secundum ASD with a left-to-right shunt (Qp:Qs >1.5:1), along with right atrial and ventricular enlargement. There was moderate tricuspid regurgitation, and Doppler estimates of right ventricular systolic pressure indicated severe pulmonary arterial hypertension (PAH). Retrospectively, an ASD measurement of 6 mm had been documented during a screening echocardiogram performed one month earlier as part of the routine cardiac evaluation recommended for infants with Down syndrome - already accompanied by elevated pulmonary pressures - suggesting rapid progression of pulmonary vascular pathology. No other structural cardiac anomalies were identified (e.g., no ventricular septal defect or patent ductus arteriosus).
Although the two echocardiograms were performed by different pediatric cardiologists, both assessments were conducted at the same center using standardized pediatric protocols. Minor inter-observer variability in measuring ASD size is possible, but the accompanying clinical deterioration, right heart dilation, and increased shunt volume suggest genuine progression in both anatomical and hemodynamic terms. While idiopathic PAH remains a differential consideration - especially in Down syndrome - the presence of a significant left-to-right shunt, radiologic signs of volume overload, and modest improvement in PA pressures following infection control collectively support ASD-related PAH as the primary etiology in this case. Although right heart catheterization and advanced workup (e.g., autoimmune or hematologic evaluation) were not performed due to the patient's clinical instability, no clinical or laboratory features suggested an alternative cause.
Working diagnosis
Combining clinical and investigational findings, the team arrived at the following key diagnoses: (a) Down syndrome (Trisomy 21) - with associated features and subclinical hypothyroidism (see Table 3). (b) Congenital heart disease - an isolated secundum ASD (~10 mm), now significantly shunting left-to-right. (c) Severe pulmonary arterial hypertension - presumably driven by the large ASD in the context of Down syndrome’s predisposition to early-onset PH. (d) Acute pneumonia and sepsis - evidenced by fever, respiratory distress, high CRP, and improvement on antibiotics. (e) Acute gastroenteritis - manifesting with vomiting and diarrhea, likely viral or antibiotic-related. (f) Failure to thrive - multifactorial (cardiac burden, recurrent infections, DS-related feeding challenges). (g) Subclinical hypothyroidism - common in DS, potentially contributing to poor growth and delayed metabolic adaptation.
Hospital course and management overview
Upon admission to the pediatric intensive care unit, antibiotic therapy (IV ceftriaxone) and supportive measures (oxygen supplementation, IV fluids for dehydration, careful monitoring of fluid balance) were initiated. Given severe PAH, sildenafil (a phosphodiesterase-5 inhibitor) was started at a low dose to reduce pulmonary artery pressure. The infant tolerated the regimen without hypotension and showed gradual clinical improvement by the third hospital day. Oxygen saturation increased from 88% to 93-94% on room air; however, this improvement likely reflected resolution of pneumonia rather than a direct effect of sildenafil, given the left-to-right nature of the shunt. Bronchodilators and antiemetics were administered as indicated, and nutritional support was optimized to address failure to thrive. By Day 5, fever resolution, improved WBC count (8×10^9^/L), and reduced CRP (50 mg/L) reflected infection control. A repeat echocardiogram continued to show severe PAH, though with a modest decrease in estimated pulmonary pressures. Definitive ASD closure was deemed essential to prevent progression to irreversible pulmonary vascular disease; however, the cardiac surgery team recommended delaying repair until the infant was more stable, had gained weight, and the risk of perioperative complications was lower.
Discussion
This case illustrates the unusually rapid progression of pulmonary arterial hypertension (PAH) in a six-month-old infant with Down syndrome (DS) and an isolated secundum atrial septal defect (ASD) - a combination not typically associated with severe early-onset PAH. While ASDs are generally well tolerated in non-syndromic infants, DS confers a nearly 10-fold increased risk of PAH due to trisomy 21-specific genetic, immunologic, and pulmonary vulnerabilities [1,4]. Although rarely reported, similar cases in the literature describe early PAH in DS infants with pre-tricuspid shunts, suggesting that even isolated ASDs can be clinically significant in this population. Our patient represents one of the youngest documented cases of such progression, emphasizing the need for vigilant, high-frequency echocardiographic surveillance and multidisciplinary care to prevent irreversible pulmonary vascular disease.
Pathophysiology: a multifaceted cascade
Down syndrome confers unique genetic and anatomical vulnerabilities that intensify the hemodynamic impact of intracardiac shunts. Overexpression of genes such as DYRK1A and RCAN1 in trisomy 21 may promote smooth muscle proliferation and impair nitric oxide-mediated vasodilation, priming the pulmonary vasculature for hyper-reactivity [5,6]. Concurrently, alveolar simplification, impaired lymphatic drainage, and reduced pulmonary vascular capacity further predispose affected infants to earlier and more severe PAH [5]. In our patient, an ASD that expanded from 6 mm to 10 mm over just 1.5 months imposed a substantial left-to-right shunt on an already compromised pulmonary circuit. While inter-operator variability in echocardiographic measurements cannot be excluded, the consistent progression in both imaging and clinical status supports a true increase in shunt size and hemodynamic burden.
Environmental and clinical stressors further magnified this risk [7]. Additional factors, such as the concurrent pneumonia, likely worsened respiratory compromise and further elevated pulmonary pressures. However, it is important to recognize that diagnosing severe PAH during active respiratory infection is inherently challenging, as transient hypoxia and inflammation can acutely increase pulmonary artery pressures. In our case, the modest reduction in PA pressures following antibiotic therapy and pulmonary vasodilator initiation suggests that the infection acted as an acute exacerbating factor on top of an evolving pulmonary vascular pathology. Therefore, reassessment of PAH after clinical stabilization is critical to avoid overestimation and to determine the optimal timing for intervention.
The infant’s history of neonatal sepsis at 17 days of life likely triggered an early systemic inflammatory response, contributing to pulmonary vascular remodeling through hypoxic vasoconstriction and pro-inflammatory cytokine release (e.g., IL-6, TNF-α) [8]. Subclinical hypothyroidism (TSH 8.12 μIU/mL) may also have impaired cardiac output and metabolic reserve, though treatment was deferred due to normal free T4 levels. Collectively, the interplay of genetic predisposition, infection-related inflammation, and metabolic dysfunction culminated in an unusually aggressive PAH phenotype requiring urgent and coordinated intervention.
Comorbidities as accelerants of PAH
Immune Dysregulation and Infections
DS-associated T- and B-cell dysfunction, compounded by neutrophil chemotaxis deficits, heightens susceptibility to infections [9]. Neonatal sepsis and recurrent pneumonia in our patient likely exacerbated pulmonary inflammation and hypoxia, hastening PAH progression. Aggressive antibiotic therapy and respiratory support mitigated these effects, emphasizing infection control as a cornerstone of PAH management.
Failure to Thrive
Poor weight gain (<5th percentile) reflects the interplay of increased cardiac workload, feeding difficulties, and recurrent infections in DS [10,11]. Nutritional rehabilitation was pivotal in preparing the infant for eventual surgery, demonstrating the need for early dietetic intervention in such cases.
Subclinical Hypothyroidism
Though asymptomatic, elevated TSH levels may impair metabolic and cardiac resilience over time [12,13]. Close endocrine follow-up was prioritized post-stabilization to address this comorbidity.
Management: decoding the therapeutic strategy
Acute Medical Therapy
Initiation of sildenafil (2 mg twice daily) targeted pulmonary vasodilation, leveraging evidence that PAH in Down syndrome infants can remain partially reversible if addressed early [14]. By Day 5 of treatment, oxygen saturations improved to 93-94% on room air, suggesting a favorable response. Additional therapies included antibiotics for pneumonia, ondansetron for vomiting, and bronchodilators, reflecting a comprehensive, multimodal approach to reduce all exacerbating factors contributing to PAH [8,14].
Surgical Deferral
Despite the severity of PAH, ASD closure was deferred, underscoring the heightened perioperative risks in a small, acutely ill infant with active infections [14,15]. Literature supports timely surgical intervention prior to the development of irreversible pulmonary vascular disease, yet in this case, the surgical team determined that immediate repair was too high-risk given the infant’s weight of 3.5 kg and concurrent pneumonia. A “stabilize now, operate later” strategy was adopted, with expectations that weight gain, infection resolution, and continued pulmonary vasodilator therapy would reduce operative morbidity and improve surgical outcomes [14,16].
Multidisciplinary Collaboration
Close coordination among cardiology, pulmonology, infectious disease, nutrition, and cardiothoracic surgery specialists proved crucial. Cardiologists directed PAH management, pulmonologists focused on respiratory support and infection control, while surgeons evaluated the timing of intervention. This team-based strategy ensured that interrelated comorbidities - immune vulnerability, hypothyroidism, and growth deficits - were addressed concurrently, optimizing the patient’s readiness for definitive ASD closure [10,14].
Insights from the literature and clinical implications
Down syndrome infants with congenital heart defects are at particularly high risk for early-onset PAH. Registry data indicate a median age of PH diagnosis at approximately six months in this population [15]. Notably, PH diagnosed before six months of age has a significantly higher likelihood of resolution following surgical repair compared to diagnoses made later (54% vs. 29% resolution) [15]. Our case thus reinforces the value of vigilant echocardiographic follow-up - monthly if necessary - in high-risk infants, particularly those showing growth failure or recurrent infections [10,15].
Therapeutically, the use of sildenafil aligns with emerging evidence supporting pulmonary vasodilators in Down syndrome-associated PAH [14,16]. Although the optimal dosing regimen remains under investigation, early administration in our patient facilitated clinical stabilization, enabling deferment of surgery until less hazardous circumstances arose. From a surgical standpoint, timing remains a delicate balance: early ASD closure may arrest PAH progression, but operating on a critically ill infant with ongoing infections and malnutrition poses significant perioperative risks [16]. This case illustrates the prudence of a staged strategy - initial medical stabilization followed by definitive curative intervention.
The rapid evolution of severe PAH in this six-month-old with Down syndrome and a secundum ASD provides a stark reminder that Down syndrome can significantly modify the natural course of congenital heart lesions [17]. A convergence of factors - recurrent infections, immune dysregulation, and subclinical hypothyroidism - alongside a substantial left-to-right shunt, created a high-stakes scenario necessitating urgent pharmacologic intervention and meticulously timed surgical planning [8,9,11,18]. By prioritizing infection control, nutritional support, and pulmonary vasodilation, the multidisciplinary team aimed to optimize the infant’s condition for eventual ASD closure. Ultimately, this case underscores the critical importance of early and frequent cardiac evaluation in infants with Down syndrome, aggressive management of associated comorbidities, and adaptable intervention strategies - a model that may improve outcomes in similarly complex pediatric cases.
Conclusions
This six-month-old infant with Down syndrome developed severe pulmonary arterial hypertension (PAH) secondary to an ostensibly “benign” secundum atrial septal defect (ASD), illustrating how comorbidities in Down syndrome - recurrent infections, immune dysregulation, and failure to thrive - can precipitate aggressive PAH at an unexpectedly early age. Prompt multidisciplinary management, which included pulmonary vasodilators, infection control, and nutritional support, stabilized the patient and set the stage for planned ASD closure to potentially reverse PAH. Given Down syndrome’s 10-fold higher risk of PAH, vigilant echocardiographic screening is crucial, as timely recognition and intervention can prevent irreversible pulmonary vascular damage. This case underscores the importance of aggressively managing infections, tracking growth and thyroid status, and considering relatively early surgical intervention in Down syndrome infants with significant shunts. Long-term follow-up will ultimately clarify optimal timing for both closure of the defect and tapering of pharmacological support, guiding future management strategies in this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The role of genetics in development of congenital heart disease Pediatric Cardiology: Fetal, Pediatric, and Adult Congenital Heart Diseases Yamagishi H 117147 Cham Springer 2024
- 2Pulmonary manifestations of autoimmune diseases In: Translational Autoimmunity Calcagno TM Mirsaeidi M 265294 Academic Press 42022
- 3Clinical practice. The care of children with Down syndrome Eur J Pediatr Weijerman ME de Winter JP 1445145216920102063218710.1007/s 00431-010-1253-0PMC 2962780 · doi ↗ · pubmed ↗
- 4Down syndrome Cassidy and Allanson's Management of Genetic Syndromes Korlimarla A Hart SJ Spiridigliozzi GA Kishnani PS 355387 John Wiley & Sons, Inc.2021
- 5The regulator of calcineurin (RCAN 1) an important factor involved in atherosclerosis and cardiovascular diseases development J Med Life Torac E Gaman L Atanasiu V 48148772014 https://pmc.ncbi.nlm.nih.gov/articles/PMC 431612325713607 PMC 4316123 · pubmed ↗
- 6Adults with Down syndrome challenge another paradigm: when aging no longer entails arterial hypertension J Clin Hypertens (Greenwich) Roy-Vallejo E Galván-Román JM Moldenhauer F Real de Asúa D 112711332220203264428510.1111/jch.13930 PMC 8030086 · doi ↗ · pubmed ↗
- 7Life stress, genes, and depression: multiple pathways lead to increased risk and new opportunities for intervention Sci STKE Charney DS Manji HK 02004200410.1126/stke.2252004 re 515039492 · doi ↗ · pubmed ↗
- 8Pulmonary arterial hypertension: pathogenesis and clinical management BMJ Thenappan T Ormiston ML Ryan JJ Archer SL 0360201810.1136/bmj.j 5492 PMC 688997929540357 · doi ↗ · pubmed ↗