Local Ablative Treatment of the Primary Tumour in Patients With Metastatic Breast Cancer: A Retrospective Observational Study
Maria Marín Alcalá, Marta Andrés Granyó, Dánae Guerra Fernández, Jairo Cortés Prados, Esther Rubio Calatayud, Ignasi Roig Quilis, Nuria Camiña, Ramón Roca Puig, Remei Blanco Guerrero, Marc Campayo

TL;DR
This study examines the benefits of local surgery or radiotherapy for the primary tumor in metastatic breast cancer patients who respond well to systemic treatment.
Contribution
The study provides real-world evidence on the effectiveness of local ablative treatment in metastatic breast cancer patients with good systemic response.
Findings
Patients showed excellent progression-free survival up to 60 months from diagnosis.
Local ablative treatment was associated with a 78% probability of not relapsing at 60 months.
Most patients had luminal breast cancer and were classified as oligometastatic.
Abstract
Background: Metastatic disease is the cause of death in most patients with breast cancer. The potential benefits of breast surgery (i.e., mastectomy or lumpectomy) of the primary tumour in patients with metastatic breast cancer are controversial. In clinical practice, selected multimetastatic and oligometastatic patients who show a complete metabolic response to systemic treatment receive local ablative treatment (breast surgery and/or radiotherapy) of their primary tumour. Objectives: We described the local ablative treatment of primary tumours received by patients with oligometastatic and multimetastatic breast cancer with good systemic treatment response and analysed our cohort’s progression-free survival (PFS). Patients and methods: A retrospective, descriptive cohort study was conducted at the Consorci Sanitari de Terrassa, Spain, from March 2013 to November 2023. We included all…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
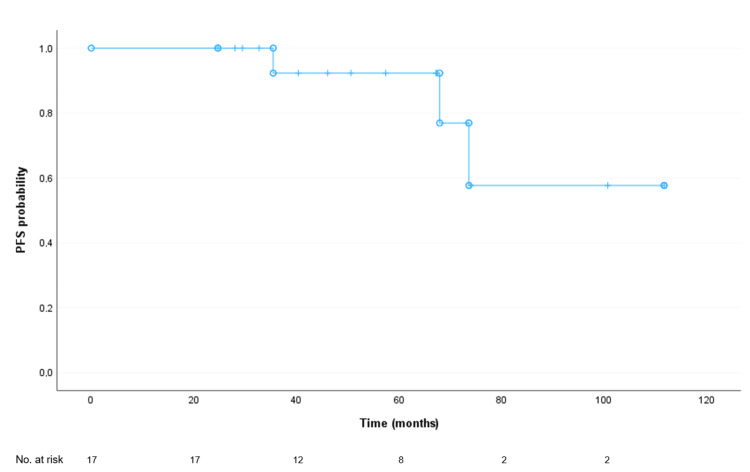 Figure 1
Figure 1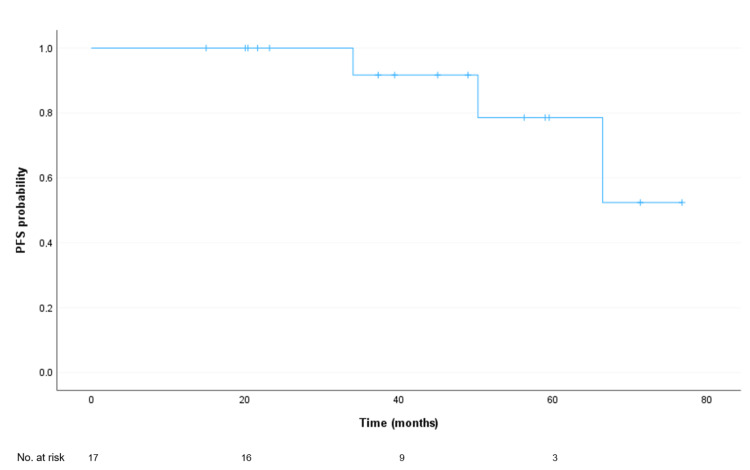 Figure 2
Figure 2| Variables | Overall (n = 17) | Luminal (n = 9) | HER2 (n = 6) | TN (n = 2) |
| Sex, n (%) | ||||
| Female | 16 (94) | 8 (89) | 6 (100) | 2 (100) |
| Male | 1 (6) | 1 (11) | 0 (0) | 0 (0) |
| Age at diagnosis (years), median (range) | 50 (26-72) | 50 (26-72) | 52 (34-64) | 50 (47-53) |
| Race, n (%) | ||||
| Caucasian | 17 (100) | 9 (100) | 6 (100) | 2 (100) |
| Tumour size, n (%) | ||||
| ≤5 cm (T1 and T2) | 10 (59) | 5 (56) | 4 (67) | 1 (50) |
| >5 cm (T3 and T4) | 7 (41) | 4 (44) | 2 (33) | 1 (50) |
| Nodal involvement, n (%) | ||||
| N0 | 4 (24) | 3 (33) | 1 (17) | 0 (0) |
| N1-N3 | 13 (76) | 6 (67) | 5 (83) | 2 (100) |
| Oestrogen receptor, n (%) | ||||
| Positive ≥1% | 11 (65) | 9 (100) | 2 (33) | 0 (0) |
| Negative <1% | 6 (35) | 0 (0) | 4 (67) | 2 (100) |
| Progesterone receptor, n (%) | ||||
| Positive ≥1% | 10 (59) | 8 (89) | 2 (33) | 0 (0) |
| Negative <1% | 7 (41) | 1 (11) | 4 (67) | 2 (100) |
| Ki-67 expression, n (%) | ||||
| High (>20%) | 13 (76) | 5 (56) | 6 (100) | 2 (100) |
| Low (≤20%) | 4 (24) | 4 (44) | 0 (0) | 0 (0) |
| Type of metastatic disease, n (%) | ||||
| Oligometastatic | 12 (71) | 7 (78) | 3 (50) | 2 (100) |
| Multimetastatic | 5 (29) | 2 (22) | 3 (50) | 0 (0) |
| Variables | Overall (n = 17) | Oligometastatic (n = 12) | Multimetastatic (n = 5) |
| Sex, n (%) | |||
| Female | 16 (94) | 11 (92) | 5 (100) |
| Male | 1 (6) | 1 (8) | 0 (0) |
| Age at diagnosis (years), median (range) | 50 (26-72) | 50 (26-72) | 58 (34-60) |
| Race, n (%) | |||
| Caucasian | 17 (100) | 12 (100) | 5 (100) |
| Tumour size, n (%) | |||
| ≤5 cm (T1 and T2) | 10 (59) | 8 (67) | 2 (40) |
| >5 cm (T3 and T4) | 7 (41) | 4 (33) | 3 (60) |
| Nodal involvement, n (%) | |||
| N0 | 4 (24) | 4 (33) | 0 (0) |
| N1-N3 | 13 (76) | 8 (67) | 5 (100) |
| HER2 overexpression, n (%) | |||
| Yes | 6 (35) | 3 (25) | 3 (60) |
| No | 11 (65) | 9 (75) | 2 (40) |
| Oestrogen receptor, n (%) | |||
| Positive ≥1% | 11 (65) | 9 (75) | 2 (40) |
| Negative <1% | 6 (35) | 3 (25) | 3 (60) |
| Progesterone receptor, n (%) | |||
| Positive ≥1% | 10 (59) | 8 (67) | 2 (40) |
| Negative <1% | 7 (41) | 4 (33) | 3 (60) |
| Ki-67 expression, n (%) | |||
| High (>20%) | 13 (76) | 8 (67) | 4 (80) |
| Low (≤20%) | 4 (24) | 4 (33) | 1 (20) |
| Variables | Overall (n = 17) | Luminal (n = 9) | HER2 (n = 6) | TN (n = 2) |
| Initial systemic treatment | ||||
| EC + Taxanes | 4 (24) | 3 (33) | 0 (0) | 1 (50) |
| EC + Taxanes + Carboplatin | 1 (6) | 0 (0) | 0 (0) | 1 (50) |
| EC + Taxanes + Anti-HER2 | 2 (12) | 0 (0) | 2 (33) | 0 (0) |
| Taxanes + Anti-HER2 | 4 (24) | 0 (0) | 4 (67) | 0 (0) |
| HT | 1 (6) | 1 (11) | 0 (0) | 0 (0) |
| HT + CDK4/6-i | 5 (29) | 5 (56) | 0 (0) | 0 (0) |
| Local ablative treatment | ||||
| Primary | ||||
| Tumourectomy | 2 (12) | 1 (11) | 1 (17) | 0 (0) |
| Tumourectomy + SLNB | 2 (12) | 1 (11) | 1 (17) | 0 (0) |
| Tumourectomy + Lymphadenectomy | 3 (18) | 1 (11) | 1 (17) | 1 (50) |
| Mastectomy + SLNB | 1 (6) | 1 (11) | 0 (0) | 0 (0) |
| Mastectomy + Lymphadenectomy | 7 (41) | 4 (44) | 2 (33) | 1 (50) |
| RT | 2 (12) | 1 (11) | 1 (17) | 0 (0) |
| Metastasis | ||||
| None | 9 (53) | 4 (44) | 5 (83) | 0 (0) |
| RT bone M1 | 5 (29) | 5 (56) | 0 (0) | 0 (0) |
| RT nodal M1 | 2 (12) | 0 (0) | 1 (17) | 1 (50) |
| RT nodal and bone M1 | 1 (6) | 0 (0) | 0 (0) | 1 (50) |
| Adjuvant treatment | ||||
| RT | 6 (35) | 3 (33) | 1 (17) | 2 (100) |
| RT + Anti-HER2 | 1 (6) | 0 (0) | 1 (17) | 0 (0) |
| RT + HT | 2 (12) | 2 (22) | 0 (0) | 0 (0) |
| HT | 2 (12) | 1 (11) | 1 (17) | 0 (0) |
| RT + Anti-HER2 + HT | 1 (6) | 0 (0) | 1 (17) | 0 (0) |
| None | 5 (29) | 3 (33) | 2 (33) | 0 (0) |
| Variables | Overall (n = 17) | Oligometastatic (n = 12) | Multimetastatic (n = 5) |
| Initial systemic treatment | |||
| EC + Taxanes | 4 (24) | 4 (33) | 0 (0) |
| EC + Taxanes + Carboplatin | 1 (6) | 1 (8) | 0 (0) |
| EC + Taxanes + Anti-HER2 | 2 (12) | 2 (17) | 0 (0) |
| Taxanes + Anti-HER2 | 4 (24) | 1 (8) | 3 (60) |
| HT | 1 (6) | 0 (0) | 1 (20) |
| HT + CDK4/6-i | 5 (29) | 4 (33) | 1 (20) |
| Local ablative treatment | |||
| Primary | |||
| Tumourectomy | 2 (12) | 0 (0) | 2 (40) |
| Tumourectomy + SLNB | 2 (12) | 2 (17) | 0 (0) |
| Tumourectomy + Lymphadenectomy | 3 (18) | 3 (25) | 0 (0) |
| Mastectomy + SLNB | 1 (6) | 1 (8) | 0 (0) |
| Mastectomy + Lymphadenectomy | 7 (41) | 5 (42) | 2 (40) |
| RT | 2 (12) | 1 (8) | 1 (20) |
| Metastatic | |||
| None | 9 (53) | 5 (42) | 4 (80) |
| RT bone M1 | 5 (29) | 5 (42) | 0 (0) |
| RT nodal M1 | 2 (12) | 1 (8) | 1 (20) |
| RT nodal and bone M1 | 1 (6) | 1 (8) | 0 (0) |
| Adjuvant treatment | |||
| RT | 6 (35) | 5 (42) | 1 (20) |
| RT + Anti-HER2 | 1 (6) | 0 (0) | 1 (20) |
| RT + HT | 2 (12) | 2 (17) | 0 (0) |
| HT | 2 (12) | 2 (17) | 0 (0) |
| RT + Anti-HER2 + HT | 1 (6) | 1 (8) | 0 (0) |
| None | 5 (29) | 2 (17) | 3 (60) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Breast Lesions and Carcinomas · Cancer Diagnosis and Treatment
Introduction
Breast cancer is the most commonly diagnosed cancer in women worldwide, with more than 2.3 million new cases identified in 2022, and it is also the most common cause of cancer-related deaths in women [1]. In the European Union, 390,675 new cases were diagnosed in 2022, and 431,334 are estimated to be diagnosed in 2040 [2]. The five-year relative survival of women diagnosed with breast cancer in Europe is 82%, ranging from 74% in Eastern Europe to 85% in Northern Europe [3]. Although breast cancer-related deaths have been decreasing in developed countries, metastatic disease remains the underlying cause of death in most of these patients [4]. In this sense, a French study estimated that the overall survival of metastatic breast cancer patients was 37.22 months (95% confidence interval (CI): 36.3-38.04), with notable differences among the luminal (42.12 months, 95% CI: 40.90-43.10), HER2-positive (44.91 months, 95% CI: 42.51-47.90), and triple-negative (TN) (14.52 months, 95% CI: 13.70-15.24) subgroups [5]. In metastatic breast cancer, systemic therapy is initially recommended and, for patients showing good response, treating the primary tumour should be considered [6].
The standard therapy for metastatic breast cancer patients depends on the cancer's molecular subtype, varies between centres, and should be individualised according to patient tolerability [7]. However, some general trends can be established. In hormone receptor-positive/HER2-negative patients, the therapeutic approach consists of serial hormonal and targeted therapies until the disease becomes hormone-resistant; then, treatment should transition to chemotherapy or drugs being evaluated in clinical studies [7]. In HER2-positive patients, HER2-target agents combined with chemotherapy and hormonal therapy, if hormone receptor-positive, are advisable [7]. TN patients usually receive chemotherapy, and immunotherapy has been recently incorporated into the first-line regimens in some patients [7].
The potential benefits of breast surgery (i.e., mastectomy or lumpectomy) of the primary tumour in metastatic breast cancer patients remain controversial [8]. This procedure has been considered more appropriate in oligometastatic patients [8], although the definition of oligometastasis lacks consensus [9,10]. However, in clinical practice, selected multimetastatic patients who show a complete metabolic response to systemic treatment (leaving only residual locoregional disease) receive local ablative treatment (breast surgery and/or radiotherapy) of their primary tumour as well, albeit the evidence regarding this practice is non-existent.
Therefore, we evaluated the clinical outcomes of patients with stage IV breast cancer receiving local ablative treatment in our centre to improve our understanding of the benefits of this approach in this setting. We aimed to describe the baseline characteristics and treatments (initial systemic, local ablative, and adjuvant) of a group of patients with oligometastatic and multimetastatic (with good systemic treatment response) breast cancer. In addition, we analysed the progression-free survival (PFS) of our cohort from the date of diagnosis and from the date of local ablative treatment.
Materials and methods
Study design and setting
This retrospective, descriptive cohort study was carried out at the Consorci Sanitari de Terrassa (CST, Spain) from March 2013 to November 2023, with a follow-up of at least 14 months after local ablative treatment. The study was approved by the Clinical Research Ethics Committee of the CST, and we obtained written informed consent from all study participants.
Participants
We included all consecutive patients aged ≥18 years with histologically confirmed metastatic breast cancer who underwent local ablative treatment after receiving systemic therapy. The definition of oligometastatic cancer is still a matter of debate. We chose the definition endorsed by the European Society for Medical Oncology to classify patients as oligometastatic if presenting a maximum of five metastatic lesions, not necessarily located in the same site, and all potentially susceptible to local ablative treatment [11]. Patients were otherwise classified as multimetastatic. We classified patients as multimetastatic when they presented metastatic disease (including patients with a high metastatic tumour burden) after receiving systemic treatment. They showed a complete metabolic response of distant lesions by PET/CT, but locoregional disease persisted.
Immunohistochemistry
We performed immunostaining for ERb on 4 µm sections of formalin-fixed, paraffin-embedded (FFPE) samples using the HercepTest™ mAb pharmDx (Dako Omnis) immunostaining system. We carried out antigen retrieval by immersing the preparations in Target Retrieval Solution Low pH for 30 minutes at 97 °C with the mouse monoclonal antibody clone DG44 RTU, incubating it for 10 minutes. We conducted immunohistochemistry for hormone receptors and Ki-67 on FFPE samples, starting with a 3 µm section stained with haematoxylin and eosin to verify the presence of an adequate number of invasive tumour cells. We prepared 4 µm serial sections and mounted them on adhesive slides specifically for immunostaining oestrogen receptor (ER), progesterone receptor (PR), and Ki-67. We performed all immunostaining using the Dako OMNIS equipment with the Envision Flex (Dako Omnis) visualisation system, and we immersed the preparations in Target Retrieval Solution for antigen retrieval. For ER immunostaining, we used the EP1 clone; for PR, the PgR 1294 clone from Dako; and for Ki-67, the MIB-1 clone from Dako.
According to the immunohistochemistry evaluation, we considered tumours positive for ER and PR when at least 1% of the tumour cells showed unequivocal nuclear staining, according to American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines [12]. HER2 was scored according to the pattern of membranous staining and percentage of stained malignant cells (0, no staining or faint incomplete staining in <10% of cells; 1, faint incomplete staining in >10% of cells; 2, weak to moderate complete staining in >10% of cells; and 3, strong complete staining in >10% of cells). Scores 2 (with FISH (fluorescence in situ hybridisation) amplification) and 3 were considered positive. Regarding Ki-67, the fraction of proliferating cells was based on a count of at least 500 tumour cells. Ki-67 values were expressed as the percentage of positive cells in each case. Cases with >20% positive nuclei were classified as high Ki-67 expression, and those with ≤20% were classified as low Ki-67 expression [13].
Intervention
Our patients formed a heterogeneous group and presented with varying metastatic patterns and histological subtypes. Therefore, distinct systemic treatment approaches were required, following the recommendations of scientific societies at the different times our patients were diagnosed over the years [11,14-16].
The local ablative treatment of the primary tumour received by patients included mastectomy, axillary lymphadenectomy, lumpectomy, selective lymph node biopsy, or any combination. Non-surgical radiotherapy radical treatment of the residual locoregional disease was also considered a local ablative treatment. The ablative treatment of metastases was always radiotherapy. For the breast, we used hypofractionated doses of 40.05 Gy at 2.67 Gy/s using the three-dimensional conformal radiation therapy technique; in cases of conservative surgery, a boost was also performed. For oligometastatic lesions, stereotactic body radiotherapy (SBRT) was performed using the volumetric modulated arc therapy technique, except for cases that did not meet SBRT criteria and were treated with the conventional technique.
Outcomes and measures
We gathered participants’ sociodemographic and clinicopathological variables before receiving local ablative treatment, including tumour size, nodal involvement, number of metastases, molecular subtype, and treatment received.
We analysed patients with luminal (ER- and/or PR-positive and HER2-negative), HER2 (ER- and PR-negative and HER2-positive), and TN (ER- and PR-negative and HER2-negative) breast cancers separately [17]. Because of our small sample size, we decided to merge into one group all patients with luminal histology, regardless of the luminal A (Ki-67 <20%) and luminal B (Ki-67 ≥20%) subtypes. We collected data on the type of local ablative treatment received, the need for adjuvant treatments, and whether the patient received treatment for the metastasis. We decided to analyse PFS in two ways: as the time between the date of the initial diagnosis and the date of the first progression or relapse, and as the time between the date of local ablative treatment and the date of disease progression.
Statistical analysis
We used absolute frequencies and percentages to describe categorical variables, and median and range for quantitative variables. We assessed PFS using the Kaplan-Meier product-limit method and compared distributions of the survival curves using log-rank tests. We used multivariate analyses (Cox regression model) to test the following variables for their impact on progression: tumour size (greater or less than 5 cm), nodal status (positive or negative), site of metastasis (nodal or bone versus visceral), molecular type of the tumour, first treatment received (including or excluding anthracyclines, and chemotherapy versus targeted treatment), radiological response of metastases to initial systemic treatment (according to RECIST (Response Evaluation Criteria in Solid Tumors) Criteria v.1.1), type of local ablative treatment of the primary tumour (surgery versus radiotherapy), type of surgery, and whether or not local ablative treatment of residual metastatic disease was performed. We calculated two-sided P-values and set the statistical significance level at P ≤ 0.05.
Results
Baseline characteristics
A total of 17 patients were included in our study, 16 females and one male, with a median age of 50 years (range: 26-72 years). Most patients had luminal breast cancer (9, 53%), followed by HER2 (6, 35%) and TN (2, 12%). The majority, in all groups, presented with nodal involvement, whereas hormone sensitivity varied between groups (Table 1).
When considering the metastatic status of study participants, most were classified as oligometastatic (12, 71%) and the remaining as multimetastatic (5, 29%). Nodal involvement was present in all multimetastatic patients (5, 100%) and in most oligometastatic patients (8, 67%). Again, hormone sensitivity varied between groups (Table 2).
Treatment
The initial systemic treatment of patients was mostly chosen according to their molecular subtype: hormone therapy alone or in combination for luminal cancers, and anti-HER2 therapy for HER2-positive cancers. In two patients (12%), no surgery was performed on the primary tumour; instead, radical radiotherapy was administered to the locoregional residual disease following systemic treatment (Table 3).
Oligometastatic patients generally received combinations of chemotherapy with anthracyclines and taxanes (4, 33%), with the addition of anti-HER2 monoclonal antibodies when overexpression of this receptor was detected (3, 25%). For most patients with metastatic disease, the initial treatment regimen consisted of taxanes and anti-HER2 monoclonal antibodies (3, 60%) and hormone therapy alone or in combination for the two patients (40%) with hormone receptor-positive tumours (Table 4).
Overall, the most frequently performed local ablative treatment was mastectomy with axillary lymphadenectomy (7, 41%), and eight patients (47%) received local ablative treatment (radiotherapy) for metastatic lesions (always nodal or bone metastases). A total of 12 patients (71%) received some form of adjuvant treatment, most commonly radiotherapy, and systemic treatment was added based on their molecular profile (Tables 3, 4).
Progression-free survival analysis
The median PFS from the date of diagnosis was not reached, with an estimated mean follow-up of 91.8 months. At 60 months of follow-up, there was a 92% probability of not relapsing (Figure 1). The median PFS from the date of local ablative treatment was also not reached, with an estimated mean follow-up of 67.05 months. At 60 months of follow-up after this treatment, there was a 78% probability of not relapsing (Figure 2). None of the clinicopathological factors analysed showed a correlation with PFS (data not shown).
Progression-free survival (PFS) of study participants from breast cancer diagnosisMedian PFS: Not reached.Mean PFS (limited to the longest survival time, if censored): 91.8 months (95% confidence interval: 73.9-109.7 months.
Progression-free survival (PFS) of study participants from intervention or local ablative treatmentMedian PFS: Not reached.Mean PFS (limited to the longest survival time, if censored): 67.1 months (95% confidence interval: 58.1-76.0 months).
Discussion
Our 17 patients formed a small and heterogeneous cohort with metastatic breast cancer, 12 of whom were oligometastatic and five had multimetastatic disease. The histological types were also varied, and their initial systemic treatment depended on their molecular subtype. The most common local ablative treatment was mastectomy with lymphadenectomy. Almost half of our cohort received radiotherapy for metastatic lesions, and most were irradiated as part of their adjuvant treatment. Neither the median PFS from the date of diagnosis nor from the date of local ablative treatment was reached.
In our study, nearly all patients were progression-free five years after receiving their first treatment for metastatic breast cancer. This result exceeded the expected PFS in the general population of patients with metastatic breast cancer [5,18-20] and is consistent with the findings of other retrospective series on oligometastatic breast cancer [21-23]. However, these observations should be interpreted with caution. The oligometastatic condition has been hypothesised to carry a better prognosis, as it reflects less aggressive tumour biology (more cellular adhesion, less mobility, reduced survival in the blood or lymphatic stream, and a diminished capacity to proliferate in secondary tissues) [24]. Therefore, the value of a radical approach to treating metastatic lesions and the primary tumour should be established through randomised prospective studies, which are very limited in this context.
Turning to randomised trials, the MF07-01 [25], ABCSG-POSITIVE [26], ECOG-ACRIN 2108 [27], Tata Memorial Centre [28], and NRG-BR002 [29] studies did not demonstrate an increase in overall survival for patients who underwent local ablative treatment. However, the first study did show a trend towards achieving this goal with a longer follow-up than initially planned. These studies suffered from significant heterogeneity in terms of the molecular subtypes of the included patients, the systemic treatments administered, and whether ablative treatments were performed on metastases (in oligometastatic patients) beyond the radical treatment of the primary tumour. Given everything mentioned above, drawing conclusions about the potential benefit of ablative treatment of the primary tumour in patients with metastatic breast cancer is complex. However, a single study seemed to detect a certain benefit in patients with the luminal phenotype [25].
Due to the small size of our series, we did not expect to obtain significant results to emphasise the use of local ablative treatment in a specific group of patients defined by clinicopathological factors. For the same reason, we did not consider it appropriate to analyse overall survival results. Nonetheless, we considered it important to present our findings, since our impression was that, overall, our patients benefited from local ablative treatments of their primary tumours, as demonstrated by their high PFS values. Notably, previous reports did not consider the response to systemic treatment a criterion for considering local ablative treatment and, contrary to our study, did not include patients with multimetastasis showing a complete metabolic response, leaving only locoregional residual disease. In our cohort, these patients represented 29% of those analysed (among whom 60% were HER2-positive) and, to the best of our knowledge, they have not been specifically evaluated before. This patient selection may explain the difference between our data and the results of the studies mentioned above [25-29]. This suggests that perhaps not only the magnitude of metastatic disease, but also tumour biology and the response to systemic treatment, could be determining factors in considering local treatment for oligometastatic and multimetastatic patients.
However, our results should be interpreted in light of the study’s limitations, mainly stemming from its descriptive and retrospective nature and, therefore, the absence of a control group. In addition, the small sample size could preclude extrapolation of our patients’ outcomes to larger populations. The short minimum follow-up and the heterogeneity of our sample should also be taken into account when evaluating our findings.
Conclusions
Treatments received by patients with oligometastatic or multimetastatic (with good systemic treatment response) breast cancer who underwent local ablative treatment of their primary tumour depended on the molecular subtype. The analysis of our cohort’s follow-up showed excellent PFS from the date of diagnosis and from the date of local ablative treatment. Although highly limited, we considered that our results were sufficiently compelling to encourage further research in this area. Specifically, we call for prospective, randomised studies that take into account the different molecular subtypes and the patient’s response to systemic treatments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I Jemal A 2292637420243857275110.3322/caac.21834 · doi ↗ · pubmed ↗
- 2ECIS - European cancer information system 1 2024 2024 https://ecis.jrc.ec.europa.eu/
- 3Survival of women with cancers of breast and genital organs in Europe 1999-2007: results of the EUROCARE-5 study Eur J Cancer Sant M Chirlaque Lopez MD Agresti R 219122055120152642182210.1016/j.ejca.2015.07.022 · doi ↗ · pubmed ↗
- 4Breast cancer as a systemic disease: a view of metastasis J Intern Med Redig AJ Mc Allister SS 11312627420132384491510.1111/joim.12084 PMC 3711134 · doi ↗ · pubmed ↗
- 5Time trends of overall survival among metastatic breast cancer patients in the real-life ESME cohort Eur J Cancer Gobbini E Ezzalfani M Dieras V 17249620182966059610.1016/j.ejca.2018.03.015 · doi ↗ · pubmed ↗
- 6Aggressive local therapy for de novo metastatic breast cancer: challenges and updates (Review)Oncol Rep Liu B Liu H Liu M 1635020233744954210.3892/or.2023.8600 PMC 10394734 · doi ↗ · pubmed ↗
- 7Breast cancer treatment: a review JAMA Waks AG Winer EP 28830032120193066750510.1001/jama.2018.19323 · doi ↗ · pubmed ↗
- 8Breast surgery for metastatic breast cancer Cochrane Database Syst Rev Tosello G Torloni MR Mota BS Neeman T Riera R 03201810.1002/14651858.CD 011276.pub 2PMC 649419829542106 · doi ↗ · pubmed ↗