Psychological Symptom Risks in Spouses of Cancer Patients and Barriers to Seeking Mental Health Counselling: A Descriptive and Correlational Study
Nazan Turan, Meltem Anafarta Şendağ

TL;DR
This study finds that spouses of cancer patients experience high psychological symptoms and avoid mental health help due to stigma and lack of awareness.
Contribution
The study identifies specific psychological risks and barriers to mental health counselling among spouses of cancer patients.
Findings
Spouses showed high levels of somatization, depression, and anxiety.
Stigma and lack of knowledge prevent spouses from seeking mental health help.
Income, gender, and residence duration are significant predictors of barriers to counselling.
Abstract
This study aims to examine the risk of psychological symptoms in spouses of cancer patients and the barriers to and determinants of seeking mental health counselling. The study was conducted with a descriptive and correlational design. The data were obtained from spouses (n = 201) of cancer patients. Data collection involved the Participant Information Form (PIF), Psychological Symptom Screening Test (SCL 90‐R) and Barriers to Seeking Mental Health Counselling Scale (BMHC). Descriptive statistics and regression analysis were used to analyse the data. Participants exhibited high levels of risk in somatization (1.67 ± 0.86), depression (1.94 ± 0.92), anxiety (1.72 ± 0.68) and additional items (1.55 ± 0.53). In multiple linear regression analysis, the longest place of residence (β = −0.137), gender (β = −0.144), income level (β = 1.152) and depression were associated with BMHC.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
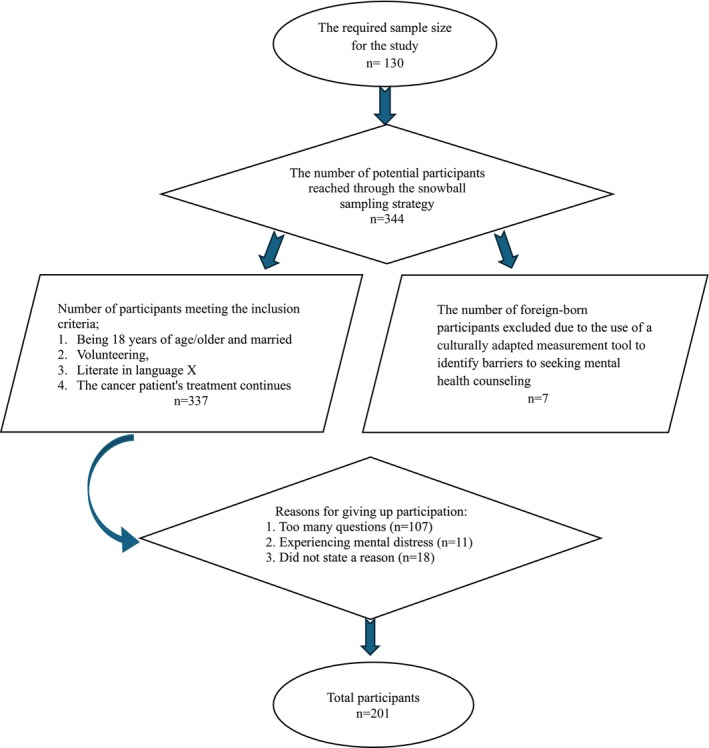 FIGURE 1
FIGURE 1| Characteristics ( |
| Characteristics ( |
|
|---|---|---|---|
| Age, years | 54.12 ± 1.17 (46–68) | Partner's cancer stage | |
| Longest place of residence | Stage 1 | 24 (11.94) | |
| Rural area | 49 (24.38) | Breast cancer | 9 (4.47) |
| Urban area | 152 (75.62) | Prostate cancer | 5 (2.48) |
| Colon cancer | 2 (1.00) | ||
| Gender | Lung cancer | 8 (3.99) | |
| Female | 58 (28.86) | Stage 2 | 16 (7.96) |
| Male | 143 (71.14) | Breast cancer | 7 (3.48) |
| Education level | Prostate cancer | 3 (1.49) | |
| Primary education | 29 (14.43) | Lung cancer | 6 (2.99) |
| High school | 127 (63.18) | Stage 3 | 98 (48.76) |
| University and above | 45 (22.39) | Breast cancer | 42 (20.90) |
| Number of children | Prostate cancer | 25 (12.44) | |
| None or one | 23 (11.44) | Colon cancer | 31 (15.42) |
| More than one | 178 (88.56) | Stage 4 | 63 (31.34) |
| Income level | Breast cancer | 26 (12.93) | |
| ≤ 33.750 TL | 115 (57.21) | Prostate cancer | 19 (9.45) |
| > 33.750 TL | 86 (42.79) | Colon cancer | 18 (8.96) |
| Needing psychological help | Receive psychological help | ||
| Yes | 189 (94.03) | Yes | 0 |
| No | 12 (5.97) | No | 201 (100) |
| Scale sub‐dimensions | Min | Max | Mean ± SD | Scale sub‐dimensions | Min | Max | Mean ± SD |
|---|---|---|---|---|---|---|---|
| Obsessive‐compulsive | 0.00 | 2.29 | 1.02 ± 0.65 | Anger‐hostility | 0.00 | 2.78 | 1.03 ± 0.78 |
| Phobic anxiety | 0.00 | 2.50 | 0.74 ± 0.54 | ||||
| Somatization | 0.00 | 3.50 | 1.67 ± 0.86 | Paranoid ideation | 0.00 | 3.54 | 1.25 ± 0.70 |
| Interpersonal sensitivity | 0.00 | 2.96 | 0.75 ± 0.59 | Psychoticism | 0.00 | 2.81 | 0.93 ± 0.67 |
| Depression | 0.00 | 3.26 | 1.94 ± 0.92 | Additional items | 0.00 | 3.72 | 1.55 ± 0.53 |
| Anxiety | 0.00 | 4.00 | 1.72 ± 0.68 | General symptom index | 0.05 | 3.17 | 1.16 ± 0.69 |
| Scale sub‐dimensions | 0.00–1.50 score (normal) | 1.51–2.50 score (high risk) | 2.51–4.00 score (very high risk) |
|---|---|---|---|
| Obsessive‐compulsive | 171 (85.07) | 30 (14.93) | 0 |
| Somatization | 58 (28.86) | 143 (71.14) | 0 |
| Interpersonal sensitivity | 174 (86.57) | 27 (13.43) | 0 |
| Depression | 45 (22.39) | 156 (77.61) | 0 |
| Anxiety | 52 (25.87) | 149 (74.13) | 0 |
| Anger‐hostility | 137 (68.16) | 64 (31.84) | 0 |
| Phobic anxiety | 183 (91.04) | 18 (8.96) | 0 |
| Paranoid ideation | 191 (95.02) | 10 (4.98) | 0 |
| Psychoticism | 198 (98.51) | 3 (1.49) | 0 |
| Additional items | 65 (32.34) | 136 (67.66) | 0 |
| General symptom index | 107 (53.23) | 94 (46.77) | 0 |
| Scale sub‐dimensions | Min | Max | Mean ± SD | Scale sub‐dimensions | Min | Max | Mean ± SD |
|---|---|---|---|---|---|---|---|
| Negative perceived value | 4 | 24 | 6.48 ± 1.95 | Lack of knowledge | 3 | 18 | 17.90 ± 6.44 |
| Discomfort with emotions | 5 | 30 | 7.54 ± 3.56 | Lack of access | 4 | 24 | 5.85 ± 2.51 |
| In‐group stigma | 5 | 30 | 21.47 ± 9.70 | Cultural barriers | 5 | 30 | 7.71 ± 4.36 |
| Covariates/factors | Simple model | Multiple model | |||
|---|---|---|---|---|---|
|
|
|
|
| VIF | |
| Longest place of residence (Ref: Urban area) | −0.012 |
| −0.137 |
| 1.314 |
| Gender (Ref: Male) | −1.006 |
| −0.144 |
| 1.217 |
| Educational level (Ref: High school) | −0.124 |
| −0.268 | 0.475 | 2.719 |
| Number of children (Ref: More than one) | −0.047 | 0.065 | |||
| Income level (Ref: > 33.750 TL) | −1.122 |
| −1.152 |
| 1.486 |
| Partner's cancer stage (Ref: Stage 3 and 4) | 0.121 | 0.083 | |||
| Somatization | 0.357 | 0.062 | |||
| Depression | 1.532 |
| 0.128 |
| 1.253 |
| Anxiety | 0.041 | 0.069 | |||
| Additional items | 1.019 | 0.093 | |||
| Covariates/factors | Simple model | Multiple model | |||
|---|---|---|---|---|---|
|
|
|
|
| VIF | |
| Longest place of residence (Ref: Urban area) | −0.254 |
| −1.007 |
| 1.908 |
| Gender (Ref: Male) | −1.962 |
| −0.368 |
| 1.762 |
| Educational level (Ref: High school) | −0.857 |
| −0.765 | 0.584 | 2.401 |
| Number of children (Ref: More than one) | 1.149 | 0.842 | |||
| Income level (Ref: > 33.750 TL) | −0.072 |
| −0.674 |
| 1.675 |
| Partner's cancer stage (Ref: Stage 3 and 4) | −1.106 |
| 0.742 | 0.327 | 2.430 |
| Somatization | 0.137 |
| 0.056 |
| 1.817 |
| Depression | 0.104 |
| 0.251 |
| 2.739 |
| Anxiety | 1.402 | 0.096 | |||
| Additional items | 0.286 |
| 1.108 |
| 1.633 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily Support in Illness · Mental Health Treatment and Access · Counseling Practices and Supervision
Introduction
1
The World Health Organisation announced that approximately 41 million people die from non‐communicable diseases every year, accounting for 74% of all deaths in the world. In the announcement, it was reported that cancer is the second leading cause of death among the top 10 causes [1]. In the statement made by the International Cancer Research Center, it was stated that one in every five people worldwide has cancer [2]. Therefore, cancers, which cause 9.3 million deaths annually [1], have become one of the most prominent public health issues of the 21st century [3].
A serious illness such as cancer can be a psychologically disturbing experience for the individual, starting from the diagnosis phase until the end of their life [3]. An individual's existential concerns may intensify following a cancer diagnosis [4]. The individual may experience mental health issues such as depression, anxiety, fear of recurrence [5, 6], post‐traumatic stress [7], and may be at risk of suicidal behaviour [8]. This situation may lead to an increase in psychiatric symptoms among cancer patients, adding to their physical symptom burden and posing significant risks to their overall quality of life [9].
Cancer can also cause psychiatric symptoms in caregivers (spouse/romantic partner). Thus, couples are often affected by cancer as a patient‐partner duo and can respond as a whole, employing dual coping [10]. Evidence has shown that spouses experience high levels of anxiety and depression [11], concern [12], stress [13], and sleep disorders [14] during this period. This may negatively affect the quality of support and care spouses provide the patient. Spouses, the most important sources of emotional and social support and care for cancer patients, play critical roles in monitoring and evaluating the patient's symptoms and making care decisions [15]. Therefore, they may often need the assistance of supportive resources and seek help to address the challenges they experience as a couple [16].
Help‐seeking is essential in achieving better support and quality of life for patients and those who care for them. It also encompasses professional behaviours aimed at seeking assistance from healthcare providers for health changes that surpass individual resources and are influenced by various factors [17, 18]. However, studies indicate that many people view seeking professional help as a last resort [18], and individuals may avoid or delay seeking professional help for mental health problems [19].
The literature states that factors hindering individuals' behaviour in seeking professional mental health services generally include lack of awareness of the problem, denial, uncertainty about where to seek help, lack of time and difficulty expressing emotions [20, 21]. Additionally, variables such as age, social and self‐stigma [21, 22], lack of knowledge, cultural understanding and financial barriers can influence individuals' decisions to seek mental health help [23].
The Present Study
1.1
There is significant evidence in the literature that spouses of patients with terminal illnesses such as cancer may experience psychological distress and other mental health problems [11, 13]. However, it seems that the reasons why spouses do not seek psychological help despite experiencing psychological problems have not yet been adequately explained. The barriers spouses face in seeking psychological help must be identified, and solutions must be developed. Therefore, spouses can be encouraged to seek psychological help at an early stage, potentially preventing the progression of psychological problems. Achieving improved well‐being in the spouse's mental state can have a two‐way effect, increasing the quality of life for both the spouse and the cancer patient. It has been noted that in the cancer care environment, the health status of a spouse has a bidirectional effect (from the spouse to the cancer patient and vice versa) [24]. In this context, this study aims to examine the risk of psychological symptoms in spouses of cancer patients and the barriers to and determinants of seeking mental health counselling. Research hypotheses are as follows:
- Spouses of cancer patients experience a high level of psychological symptom risk.
- Spouses of cancer patients have high scores on barriers to seeking mental health counselling.
- High levels of psychological symptom risk and other factors (e.g., age and gender) predict barriers to seeking mental health counselling.
Methods
2
Study Design
2.1
The study was designed as a descriptive and correlational study and was conducted online using the snowballing technique between June and September 2023. The STROBE guidelines were adopted when the study was reported.
Participants and Procedure
2.2
The sample size for the study was calculated based on the formula suggested by Tabachnick and Fidell [25] for regression analysis, N > 50 + 8 m. According to this calculation, it was determined that the sample size should be 130. Participants were selected based on inclusion criteria, which included (1) being 18 years of age or older and married, (2) volunteering, (3) literate in Turkish and (4) the cancer patient's treatment continued. Foreign nationals were excluded as a criterion because of using a culturally adapted measurement tool to determine participants' barriers to seeking mental health counselling.
Nonprobability sampling contained the risk of self‐selection bias. This could pose a significant challenge to the accuracy and reliability of research findings [26]. Additionally, in an online survey, there is no information about who participated, which can lead to the risk of failing to identify the target population [27]. Therefore, cancer patients were contacted first to ensure that all participants were spouses of cancer patients and to enhance the accuracy and reliability of the findings. In this regard, personal and social collaborations were first established. Then, using an online snowball sampling strategy, cancer patients were reached through social media platforms such as Twitter and Facebook, as well as the WhatsApp channels of eight oncology doctors, and an announcement about the research was made. A total of 344 cancer patients responded to the periodically repeated announcement. Subsequently, the spouses of the cancer patients were contacted through them and informed about the research. The participants who met the criteria were administered an online survey consisting of a Participant Information Form, the Psychological Symptom Screening Test (SCL‐90‐R) and the Barriers to Seeking Mental Health Counselling Scale (BMHC), which included 125 questions. The study was completed with 201 participants (Figure 1). All procedures conducted in the study were carried out in accordance with the Helsinki Declaration. Additionally, the study received ethical approval from the review board of University Çankırı Karatekin, and informed consent was obtained from all participants.
Flow chart.
Measures
2.3
A participant information form consisting of nine questions was used to determine the characteristics of the participants, including age, longest place of residence, gender, education level, income level (poverty threshold for a family of four), number of children, partner's cancer stage, need for psychological help and receipt of psychological help.
The Psychological Symptom Screening Test (SCL‐90‐R) developed by Derogatis and Cleary [28] was applied to assess the participants' risk for psychological symptoms. This psychiatric screening tool consists of 90 items on a 5‐point Likert‐type scale. It includes 10 sub‐dimensions: Obsessive‐Compulsive, Somatization, Interpersonal Sensitivity, Depression, Anxiety, Anger and Hostility, Phobic Anxiety, Paranoid Ideation, Psychoticism and Additional Items (e.g., item 19, ‘poor appetite’). Each sub‐dimension and the general symptom score are interpreted as follows: 0.00–1.50 is considered ‘normal’, 1.51–2.50 indicates ‘high risk,’ and 2.51–4.00 suggests ‘very high risk’. The Turkish adaptation of the scale, which demonstrated an internal reliability coefficient of 0.97 [29], was used in this study. The internal reliability coefficient of the scale in this study was found to be 0.95.
The Barriers to Seeking Mental Health Counselling Scale (BMHC), developed by Shea et al. [30], assessed participants' barriers to seeking psychological help. This 6‐point Likert‐type scale consists of 26 items and includes six sub‐dimensions: Negative Perceived Value, Discomfort with Emotions, In‐Group Stigma, Lack of Knowledge, Lack of Access and Cultural Barriers. A higher score in each sub‐dimension indicates a more significant perceived disability in that dimension. The scale is scored by averaging the scores of its sub‐dimensions, providing a total score ranging from 27 (lowest) to 162 (highest). In the Turkish adaptation of the scale, the internal reliability coefficient of the total score was 0.87, while for the sub‐dimensions, the coefficients were found to be 0.73, 0.87, 0.85, 0.85, 0.73 and 0.75, respectively [31]. In this study, the internal reliability coefficient of the total score was 0.84, with sub‐dimension coefficients determined as 0.75, 0.78, 0.85, 0.87, 0.76 and 0.80, respectively.
Statistical Analysis
2.4
SPSS 26.0 statistical software was utilised for data analysis. Normality plots and skewness/kurtosis statistics were examined to assess the distributions of quantitative variables. Descriptive statistics, including counts, percentages, means and standard deviations, were used to summarise participant characteristics and calculate scores for scale sub‐dimensions and totals. The relationships between scales and their sub‐dimensions were evaluated using Pearson correlation analysis. Univariate and multiple linear regression analyses were conducted to investigate the relationships between the study's dependent variables (SCL‐90‐R and barriers to seeking mental health counselling) and independent variables (longest place of residence, gender and number of children). A significance level of p < 0.05 was accepted. The multiple linear regression analysis included independent variables significant in univariate regression analysis. The significance level for the multiple regression was also set at p < 0.05.
Results
3
Characteristics of Participants
3.1
The mean age was 54.12 ± 1.17 years. Of the participants, 71.14% (n = 143) were male and 28.86% (n = 58) were female. Among them, 75.62% (n = 152) resided in urban areas, 24.38% (n = 49) lived in rural areas and 88.56% (n = 178) had more than one child. Most of the participants had income below the country's poverty line (57.21%, n = 115) and (63.18%, n = 127) had a high school education. Approximately half of the participants (48.76%, n = 98) reported that their partner had stage 3 cancer (breast cancer (20.90%, n = 42), prostate cancer (12.44%, n = 25), colon cancer (15.42%, n = 31)). All participants (100%, n = 201) did not receive psychological help, while 94.03% (n = 189) expressed a need for psychological help (Table 1).
Participants' Psychological Symptoms and Barriers to Seeking Mental Health Counselling
3.2
The scores of the participants from the SCL 90‐R sub‐dimensions were grouped as 0.00–1.50 (normal), 1.51–2.50 (high risk) and 2.51–4.00 (very high risk). According to SCL‐90 R test results, participants had a high level of risk in somatization (1.67 ± 0.86), depression (1.94 ± 0.92), anxiety (1.72 ± 0.68) and additional items (1.55 ± 0.53) sub‐dimension. Obsessive‐compulsive (1.02 ± 0.65), interpersonal sensitivity (0.75 ± 0.59), anger and hostility (1.03 ± 0.78), phobic anxiety (0.74 ± 0.54), paranoid ideation (1.25 ± 0.70), psychoticism (0.93 ± 0.67) and the general symptom index (1.16 ± 0.69) were found to be within the normal range (Table 2).
It was found that 2 participants (1.00%) had high‐risk scores in all sub‐dimensions of the SCL‐90‐R, while 135 participants (67.16%) had high‐risk scores in at least one sub‐dimension. A total of 64 participants (31.84%) had scores within the normal range for all sub‐dimensions of the SCL‐90‐R. Participants were determined not to have very high‐risk scores in any SCL‐90‐R sub‐dimensions (Table 3).
Of the participants identified as high risk, 30 (14.93%) had obsessive‐compulsive disorder, 143 (71.14%) had somatisation, 27 (13.43%) had interpersonal sensitivity, 156 (77.61%) had depression, 149 (74.13%) had anxiety, 64 (31.84%) had anger‐hostility, 18 (8.96%) had phobic anxiety, 10 (4.98%) had paranoid ideation, 3 (1.49%) had psychoticism, 136 (67.66%) had additional items and 94 (46.77%) had general symptom index (Table 3).
Participants' scores on the negative perceived value sub‐dimension of the BMHC scale were 6.48 ± 1.95 (min = 4, max = 24), discomfort with emotions sub‐dimension 7.54 ± 3.56 (min = 5, max = 30), in‐group stigma sub‐dimension 21.47 ± 9.70 (min = 5, max = 30), lack of knowledge sub‐dimension 17.90 ± 6.44 (min = 3, max = 18), lack of access sub‐dimension 5.85 ± 2.51 (min = 4, max = 24) and cultural barriers sub‐dimension 7.71 ± 4.36 (min = 5, max = 30) (Table 4). Since the scale does not have a specific cut‐off score, based on the average scores, participants' scores on the in‐group stigma and lack of knowledge sub‐dimension were high. In contrast, scores on the sub‐dimension of negative perceived value, discomfort with emotions, lack of access, cultural barriers and the total BMHC level can be described as low.
Factors Associated With Barriers to Seeking Mental Health Counselling
3.3
Univariate and multiple linear regression analyses were conducted to examine the impact of participants' characteristics and high‐risk psychological symptoms on BMHC subscales. The established models for negative perceived value, discomfort with emotions, lack of access and cultural barriers, which had low average scores in the BMHC subdimensions, were not found to be significant (p > 0.05). Univariate linear regression analysis was conducted to assess the impact of participants' characteristics and high‐risk psychological symptoms on in‐group stigma. Independent variables found to be significant in the analysis—longest place of residence, gender, education level, income level, partner's cancer stage and depression—were included in the multiple linear regression model. The longest place of residence (β = −0.137), gender (β = −0.144), income level (β = −1.152) and depression (β = 0.128) were associated with BMHC. According to the established model, gender, education level, income level and depression explained 36.7% of the variance in BMHC (Table 5).
Univariate linear regression analysis assessed the impact of participants' characteristics and high‐risk psychological symptoms on lack of knowledge. Independent variables found to be significant in the analysis—longest place of residence, gender, education level, income level, partner's cancer stage, somatization, depression and additional items—were included in the multiple linear regression model. The longest place of residence (β = −1.007), gender (β = −0.368), income level (β = −0.674), somatization (β = 0.056), depression (β = 0.251) and additional items (β = 1.108) were found to be associated with BMHC. In this model, the combination of longest place of residence, gender, income level, somatization, depression and additional items explained 18.2% of the variance in BMHC (Table 6).
Discussion
4
This descriptive and correlational study examined the risk of psychological symptoms in spouses of cancer patients and the barriers to and determinants of seeking mental health counselling. The study found that spouses of cancer patients exhibited high‐risk psychological symptoms, while lack of information and in‐group stigmatisation were identified as barriers to seeking help. Furthermore, specific psychological symptoms and sociodemographic characteristics were found to be associated with barriers to seeking mental health counselling and the tested hypotheses were accepted.
First, it was determined that 2 study participants (1.00%) had high‐risk scores in all sub‐dimensions of the SCL‐90‐R, while 135 participants (67.16%) had high‐risk scores in at least one sub‐dimension. Additionally, an analysis of the total scores obtained from all participants revealed that the mean depression and anxiety scores were in the high‐risk range. When this result is evaluated about the sociodemographic characteristics of the participants, it aligns with studies suggesting that a lower quality of life and the psychological symptoms of cancer patient caregivers are significantly associated with gender (male), low‐income levels, living in the same household as the patient, and being a caregiver for an advanced‐stage cancer patient [32, 33, 34]. The high caregiving burden of male spouses, their role in supporting the family, and financial difficulties may increase their risk of anxiety and depression [35, 36].
The study also found a high risk in additional items assessing somatisation, sleep disturbances, and other related problems in spouses of cancer patients. The high risk of somatisation may be related to the increased risk of depressive symptoms among spouses, as depression leads to negative and pessimistic cognitive schemas [37]. Indeed, the heavy caregiving burden, the long‐term dependency associated with caring for cancer patients, and changing social roles may place family caregivers at a higher risk for mental disorders and hopelessness [38]. This situation may unconsciously reveal somatisation as a dysfunctional and maladaptive coping mechanism [39]. On the other hand, sleep disturbance is a common problem among caregivers of cancer patients [40, 41]. In this direction, recent studies have provided evidence that sleep disturbance and/or poor sleep quality are seen in advanced cancer caregivers [42, 43].
Regarding the results on barriers to seeking psychological help, it was determined that the scores for lack of information and in‐group stigma were higher among the spouses of cancer patients compared to other barriers. This result is not surprising, as depression and anxiety are positively correlated with stigma [44], and a high risk of depression and anxiety was found among the spouses in this study. Additionally, the public presentation of psychological symptoms (such as depression) can affect stigma and mental health literacy [45]. The ability to recognise the symptoms and risk factors of mental disorders, seek professional help accordingly, and know available resources, accessible professionals, and treatment facilities are key components of mental health literacy [46]. Thus, although many individuals express an intention to seek professional help for mental health issues or to seek help for themselves when experiencing such difficulties, the actual number of those who follow through with seeking help remains low due to a lack of knowledge in this area [47, 48].
Multiple linear regression analysis also showed that increased levels of in‐group stigma among spouses were associated with depression. Additionally, it was determined that higher levels of lack of knowledge were associated with increased somatization, depression and additional symptoms. Factors that prevent patients suffering from mild to moderate depression, anxiety, sleep, eating, or somatization‐related mental disorders from seeking help may include fear of stigma or a desire to cope with problems without professional help [49]. In this regard, the study results support the literature. Although most of the participants stated that they needed psychological help, none of them indicated that they received help.
In the current study, the results of multiple linear regression analysis revealed that in‐group stigma and lack of knowledge scores, which are barriers to seeking mental health counselling, were significantly associated with the longest place of residence, gender and income level among spouses of cancer patients. Specifically, spouses with lower income, residing in rural areas, and female gender exhibited higher levels of in‐group stigmatisation and lack of knowledge. Females in low‐ and middle‐income countries often require family permission to seek professional help. Additionally, they may face barriers to accessing psychological support due to a lack of knowledge about symptoms, fear of social consequences (e.g., divorce or rejection in marriage), shame associated with cancer and financial constraints. Stigmatising attitudes may also be more pronounced when the identified individual is a woman exhibiting depressive symptoms [50].
Limitations
5
There are several limitations to the study. Firstly, conducting the study quantitatively using a survey method may have affected the accuracy of the results. Questions may not be uniformly understood in survey‐based research, and responses are limited to the provided options [51]. Therefore, a mixed‐method approach could provide a more comprehensive understanding of psychological symptoms and barriers to seeking psychological help among spouses of cancer patients.
Secondly, the study did not include cancer patients themselves, which might have influenced the findings, as cancer patients and their spouses are typically mutually affected by the disease as a unit [10]. Consequently, it remains challenging to assess the reciprocal impact between spouses.
Finally, the predominance of male participants in the study may have introduced a significant selection bias, limiting the findings' generalizability. Additionally, collecting data exclusively online may have excluded individuals without internet access or those with low digital literacy. In contrast, reliance on self‐reported data may have increased the risk of response bias. Therefore, future studies with similar objectives could be analysed with a larger population and more detailed tests.
Conclusion
6
This study found that spouses of cancer patients are at risk of psychological symptoms but often refrain from seeking psychological help due to in‐group stigmatisation and lack of knowledge. Furthermore, demographic characteristics were associated with in‐group stigma, while demographic factors, somatisation, depression and additional symptoms were linked to a lack of knowledge. Therefore, the study underscores an important clinical implication that the focus of health services should not only be on the diagnosed cancer patient but also their spouse. These implications are important for healthcare professionals because spouses lack a systematic support system to manage their psychological symptoms during the cancer patient's treatment process. Hence, healthcare professionals can organise informative campaigns and workshops addressing psychological symptoms in spouses and provide tailored psychological resources. Additionally, mental health professionals can design group‐based awareness interventions for spouses of cancer patients. This can ensure that dysfunctional thoughts and behaviours related to seeking psychological help are replaced with more functional ones, thereby encouraging spouses to seek psychological support.
Author Contributions
The conception and design of the study: N.T. and M.A.Ş.; acquisition of data: N.T.; analysis and interpretation of data: N.T.; drafting the article or revising it critically for important intellectual content: N.T. and M.A.Ş.; final approval: N.T. and M.A.Ş.
Ethics Statement
All procedures performed in the study were in accordance with the 1964 Helsinki Declaration and its later amendments. The study was approved by the Çankırı Karatekin University Review Board (2023/8). Informed consent was obtained from all participants included in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization , “World Health Statistics 2022: Monitoring Health for the SD Gs, Sustainable Development Goals,” World Health Organization, accessed December 20, 2023, https://hpfhub.info/wp‐content/uploads/2023/03/World‐Health‐Statistics‐2022‐Monitoring‐Health‐for‐the‐SD Gs‐Sustainable‐Development‐Goals‐WHO‐2022.pdf.
- 2International Agency for Research on Cancer , “IARC Publications,” accessed December 21, 2023, https://www.iarc.who.int/cards_page/iarc‐publications/.
- 3E. C. Tarbi and S. H. Meghani , “Existential Experience in Adults With Advanced Cancer: A Concept Analysis,” Nursing Outlook 67, no. 5 (2019): 540.31040052 10.1016/j.outlook.2019.03.006PMC 6764914 · doi ↗ · pubmed ↗
- 4K. M. Piderman , S. Kung , S. M. Jenkins , et al., “Respecting the Spiritual Side of Advanced Cancer Care: A Systematic Review,” Current Oncology Reports 17, no. 2 (2015): 6.25681038 10.1007/s 11912-014-0429-6 · doi ↗ · pubmed ↗
- 5Y. Yang , H. Sun , X. Luo , et al., “Network Connectivity Between Fear of Cancer Recurrence, Anxiety, and Depression in Breast Cancer Patients,” Journal of Affective Disorders 309 (2022): 358–367.35472477 10.1016/j.jad.2022.04.119 · doi ↗ · pubmed ↗
- 6L. Schapira , Y. Zheng , S. I. Gelber , et al., “Trajectories of Fear of Cancer Recurrence in Young Breast Cancer Survivors,” Cancer 128, no. 2 (2022): 335–343.34614212 10.1002/cncr.33921 PMC 9397577 · doi ↗ · pubmed ↗
- 7A. Leano , M. B. Korman , L. Goldberg , and J. Ellis , “Are We Missing PTSD in Our Patients With Cancer? Part I,” Canadian Oncology Nursing Journal 29, no. 2 (2019): 141–146.31148714 PMC 6516338 · pubmed ↗
- 8N. G. Zaorsky , Y. Zhang , L. Tuanquin , S. M. Bluethmann , H. S. Park , and V. M. Chinchilli , “Suicide Among Cancer Patients,” Nature Communications 10, no. 1 (2019): 207.10.1038/s 41467-018-08170-1PMC 633159330643135 · doi ↗ · pubmed ↗