Polysomnographic Analysis in Snoring Patients
Yan Li

TL;DR
This study analyzed sleep data from snoring patients to identify patterns linked to age, gender, and severity of breathing issues.
Contribution
The study systematically characterizes snoring patients using PSG parameters across demographic and severity groups.
Findings
Male patients had higher AHI, ODI, and SI values than females under the same BMI.
Elderly patients showed significantly higher AHI and ODI compared to younger patients.
ODI had the strongest correlation with BMI at moderate AHI levels.
Abstract
Objective: This study aimed to investigate differences and correlations in polysomnography (PSG) parameters among snoring patients in the otolaryngology department by gender, age group, and apnea-hypopnea index (AHI) severity level. Methods: Differences in parameters (AHI, oxygen desaturation index (ODI), snoring index (SI), body mass index (BMI), and age (AGE)) were compared across genders, age groups, and AHI severity levels. Relationships among these parameters were analyzed using bar charts, box plots, and correlation matrices to characterize snoring patients. Results: Under the same BMI, male patients exhibited significantly higher values for AHI, ODI, and SI compared to female patients (p < 0.01). Both AHI and ODI increased with age, showing significantly higher values in elderly patients (≥60 years) compared to younger patients (<40 years) (p < 0.01). No significant differences…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
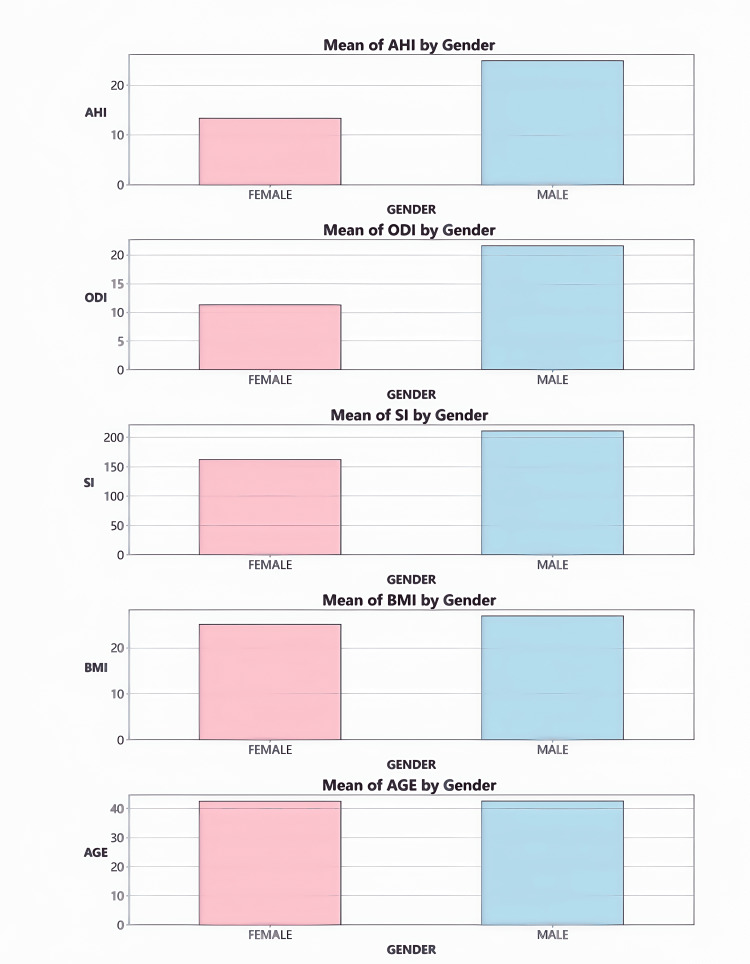 Figure 1
Figure 1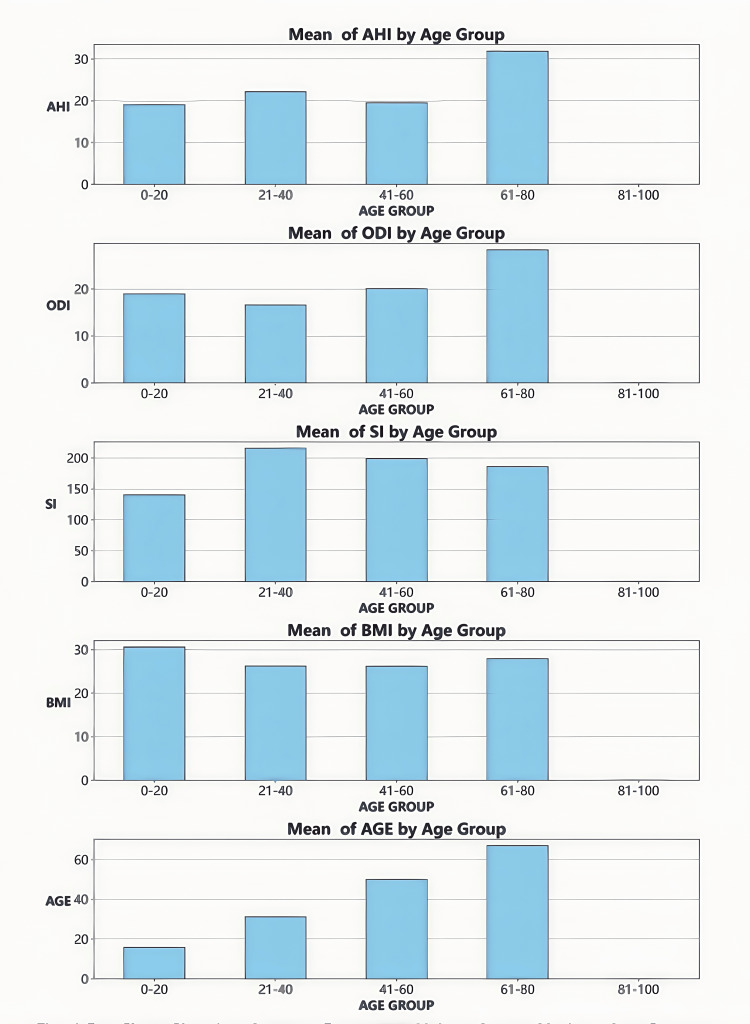 Figure 2
Figure 2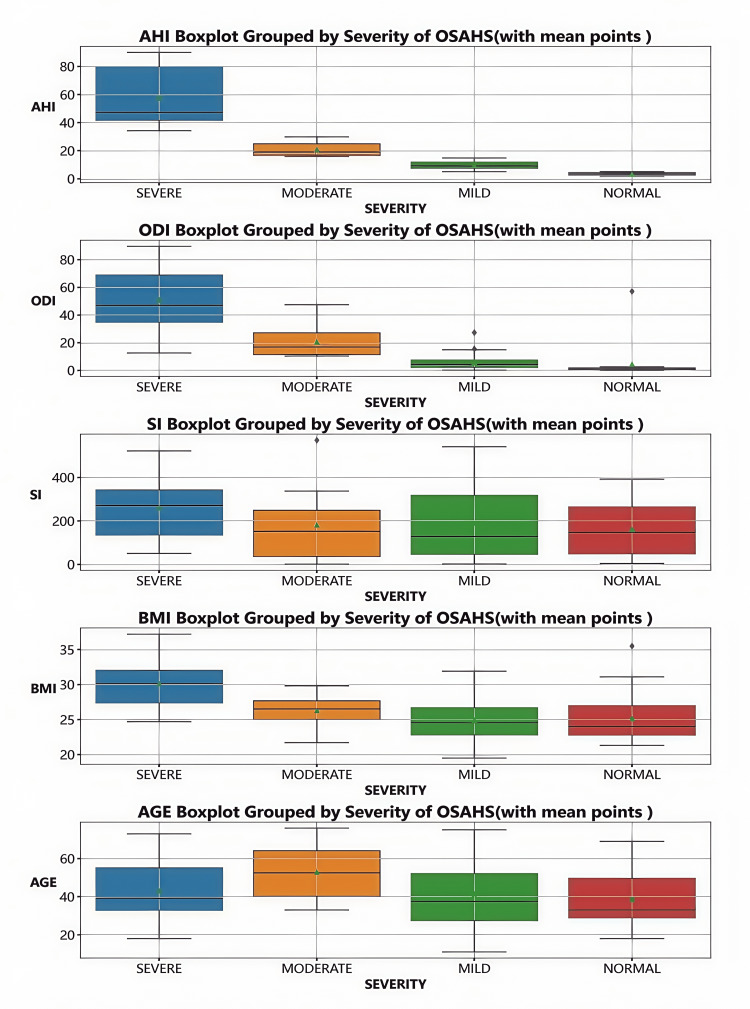 Figure 3
Figure 3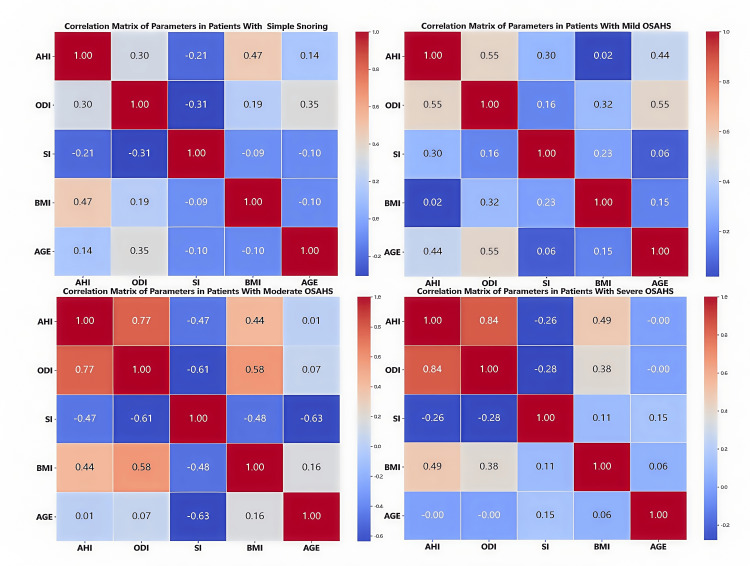 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObstructive Sleep Apnea Research · Neuroscience of respiration and sleep · Cardiovascular and Diving-Related Complications
Introduction
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a prevalent sleep-related breathing disorder, characterized by recurrent episodes of apnea and hypopnea during sleep due to upper airway obstruction [1]. It affects a significant portion of the global population, with prevalence rates varying between 2% and 10% worldwide. Notably, the incidence of OSAHS increases with age, with a higher prevalence observed in individuals over 65 years old, particularly in men, where the prevalence can reach up to 24% [2]. OSAHS is strongly associated with numerous health risks, including but not limited to respiratory difficulties, impaired sleep quality, cardiovascular diseases, metabolic disorders, respiratory infections, gastroesophageal reflux disease, mood disturbances, sexual dysfunction, and an elevated risk of accidents [3-8]. Consequently, the early detection and effective management of OSAHS are essential for enhancing patients' quality of life and mitigating potential complications [4,6,9].
Polysomnography (PSG) is universally recognized as the gold standard for diagnosing OSAHS [10]. In this study, we employ a 22-channel PSG device developed in Beijing, China. This advanced device enables real-time tracking and recording of multiple physiological parameters, thereby providing robust data support for evaluating patients' sleep quality and associated pathological characteristics.
This study aims to establish a more comprehensive and scientifically grounded reference framework for the early diagnosis, personalized treatment planning, and dynamic monitoring of OSAHS by systematically analyzing the differences and correlations among key parameters, including the apnea-hypopnea index (AHI), oxygen desaturation index (ODI), snoring index (SI), body mass index (BMI), and age (AGE), across various demographic groups defined by gender, age, and AHI severity levels [11-13].
Materials and methods
Ninety patients diagnosed with snoring by PSG in the Otolaryngology Department of Shanghai Yida Hospital, Shanghai, China, between January 2023 and January 2024, were recruited as subjects, and their clinical data and PSG parameters were collected. The inclusion criteria included patients aged six to 80 years with suspected OSAHS, Epworth Sleepiness Scale (ESS) score≥9 [14], no conditions significantly impacting sleep or respiratory function, and who provided informed consent for PSG evaluation and follow-up. The exclusion criteria are patients with central sleep apnea, non-snoring-related sleep disorders, anatomical abnormalities affecting assessment accuracy [15], medication use impacting sleep or respiratory function, or inability to complete PSG monitoring. Using IBM SPSS Statistics for Windows, Version 27.0 (released 2020, IBM Corp., Armonk, NY) to test the power value (power > 0.8), the sample size has a high probability of detecting the real differences between parameters. This study was approved by the Ethics Committee of Shanghai Yida Hospital (approval number: 2023-0101). All patients were informed of the study and provided their written informed consent.
Methods
Patients were grouped by age (0-20, 20-40, 40-60, 60-80 years), gender (male, female), and AHI severity (normal: zero to five times/hour, mild: five to 15 times/hour, moderate: 15-30 times/hour, severe: >30 times/hour [16]).
Statistical software (Python and Jupyter Notebook in Anaconda3, Anaconda, Inc., USA) was used to analyze parameters (AHI, ODI, SI, BMI, and age) across groups. Methods included bar charts for mean comparisons, box plots for distributions, and heatmaps for correlations. The Pearson correlation coefficient assessed linear relationships, with values indicating weak (0.1-0.3), moderate (0.3-0.5), strong (0.5-0.7), and very strong (0.7-1) correlations [17].
Results
Gender differences in PSG parameters
The bar chart (Figure 1) vividly illustrates the disparities in PSG parameters between genders. Notably, male participants exhibited significantly higher values in AHI, ODI, and SI compared to female participants (p < 0.01). It is important to highlight that, within this study, no significant gender differences were observed in the distribution of BMI and age (p > 0.05).
Bar chart of average parameter values by genderCreated with statistical software Python and Jupyter Notebook in Anaconda3 (Anaconda, Inc., USA)
PSG parameter differences by age group
The bar chart(Figure 2) illustrates the variations in PSG parameters across different age groups. AHI and ODI exhibit an increasing trend with age, reaching their highest levels in the 60-80 age group and the lowest in the 0-20 age group. SI is relatively elevated in the 21-40 age group; however, no significant differences are observed among age groups. BMI is slightly higher in the 0-20 age group, yet no statistically significant differences exist across age groups. AGE differences are defined by the grouping criteria and serve to validate the accuracy of the classification.
Bar chart showing average parameter values across various age groupsCreated with statistical software Python and Jupyter Notebook in Anaconda3 (Anaconda, Inc., USA)
In summary, age demonstrates a positive correlation with AHI and ODI, with significantly higher values observed in the elderly group (≥60 years) compared to the young group (<40 years) (p < 0.05).
Differences in PSG parameters across groups by AHI severity
The differences in PSG parameters among different AHI severity groups were presented by box plots (Figure 3). ODI and BMI gradually increased with the severity of AHI and reached the highest values in severe AHI. There was no significant difference in SI among the groups. Although there was no obvious pattern in the age distribution, moderate AHI was more common in the elderly.
Box plot illustrating parameters across various OSAHS severity levelsOSAHS: obstructive sleep apnea-hypopnea syndromeCreated with statistical software Python and Jupyter Notebook in Anaconda3 (Anaconda, Inc., USA)
Correlation matrix of parameters across AHI levels
Based on the AHI grouping and matrix chart analysis, the correlations among parameters are summarized as follows (Figure 4):
Linear correlation among parameters at various OSAHS severity levelsOSAHS: obstructive sleep apnea-hypopnea syndromeCreated with statistical software Python and Jupyter Notebook in Anaconda3 (Anaconda, Inc., USA)
AHI and Other Parameters
AHI is positively correlated with ODI (strongest at severe levels, r = 0.84). AHI is positively correlated with BMI (strongest at severe levels, r = 0.49). AHI correlates most strongly with AGE at mild levels (r = 0.44). AHI correlates positively with SI at mild levels (r = 0.3) and negatively at moderate levels (r = -0.47).
ODI and Other Parameters
ODI is positively correlated with AHI. At mild AHI, ODI correlates most strongly with AGE (r = 0.44). At moderate AHI, ODI correlates most strongly with BMI (r = 0.58) and negatively with SI (r = -0.61).
SI and Other Parameters
SI correlates negatively with AGE (r = -0.63), positively with ODI (r = 0.61), negatively with BMI (r = -0.48), and negatively with AHI (r = -0.47).
Age and Other Parameters
At mild AHI, AGE correlates most strongly with ODI (r = 0.44). At moderate AHI, AGE correlates most strongly negatively with SI (r = -0.63).
BMI and Other Parameters
For the BMI-AHI correlation, mild was r = 0.47, moderate was r = 0.44, and severe was r = 0.49. For the BMI-ODI correlation, moderate was r = 0.58 and severe was r = 0.38. For the BMI-SI correlation, the strongest negative at moderate levels was r = -0.48.
In summary, AHI correlates positively with ODI and BMI, while its relationships with AGE and SI are complex. Correlations vary by AHI severity, with significant findings under specific conditions.
Discussion
Gender factor
Gender differences are particularly pronounced in patients with sleep apnea. Specifically, when BMI is matched, male patients exhibit significantly higher mean values of AHI, ODI, and SI compared to female patients (p < 0.01). This gender disparity may result from multiple factors. From an anatomical and physiological perspective, men typically have a narrower upper airway structure than women, which increases the likelihood of airway obstruction. In addition, lifestyle differences may also play a critical role in the onset and progression of sleep apnea. For instance, men are more likely to smoke and drink alcohol, habits that can exacerbate airway inflammation or impair respiratory regulation. Hormonal variations are another potential influencing factor; studies indicate that estrogen may protect against airway collapse, thereby reducing the risk of sleep apnea in women. Thus, a deeper understanding of gender differences can facilitate the development of personalized prevention and treatment strategies for different genders, enhancing intervention efficacy [18-21].
Age factor
Age is a key determinant of PSG parameters in snoring patients. Children and adolescents (0-20 years old) generally demonstrate better PSG parameters, likely due to their relatively normal airway structure and robust respiratory regulation function. As individuals age, especially during middle and older adulthood, various bodily functions decline, with the reduction in upper airway regulation being particularly notable. This decline may increase the risk of airway collapse and susceptibility to hypoxia. Furthermore, common age-related phenomena such as muscle relaxation and soft tissue hyperplasia may alter airway structure, further exacerbating snoring. Consequently, age serves not only as an important indicator of snoring risk but also indirectly influences disease severity through multiple mechanisms [22, 23].
Factors influencing AHI severity
AHI is a critical metric for assessing the severity of sleep apnea. Different AHI levels reflect varying stages of the disease and their impact on patient health. As AHI values rise, respiratory function and hypoxia become increasingly impaired, leading to issues such as daytime sleepiness, reduced attention, and heightened cardiovascular disease risk. Research has identified a significant positive correlation between BMI and AHI, underscoring the pivotal role of obesity in sleep apnea pathogenesis [24-27]. Notably, the relationship between age and AHI is complex; while AHI tends to increase with age, substantial individual variation exists. Therefore, age should not be used as the sole criterion for evaluating sleep apnea severity in clinical practice.
Limitations
Although this study provides a relatively comprehensive analysis of PSG parameters in ENT patients with snoring, several limitations warrant acknowledgment. First, the sample source may exhibit geographical bias, as regional differences in physical constitution and lifestyle could influence the generalizability of the findings. For example, dietary habits in certain areas may contribute to higher obesity rates, affecting AHI distribution patterns. Second, the study does not fully account for other factors that may influence PSG parameters, such as medication history and family genetic history. These factors could potentially confound accurate identification of snoring etiology. Future research should expand the sample size and incorporate additional variables for a more thorough and reliable analysis [28].
Conclusions
By analyzing the PSG parameters of snoring patients in the otorhinolaryngology department across different genders, ages, and AHI levels, we have elucidated the variations and correlations of each parameter among distinct population characteristics. These findings not only enhance our understanding of snoring but also offer critical references for clinicians in early diagnosis, personalized treatment planning, and disease evaluation. In addition, they provide a solid foundation for further investigating the pathogenesis of snoring.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cognitive function and life quality of patients with moderate-to-severe obstructive sleep apnea-hypopnea syndrome in China Expert Rev Respir Med Liu Y Han J Ning L Chen L Jiang X Ke A Zhang Y 4354401520213331546610.1080/17476348.2021.1852081 · doi ↗ · pubmed ↗
- 2An update on obstructive sleep apnea syndrome-a literature review Medicina (Kaunas) Platon AL Stelea CG Boișteanu O 59202310.3390/medicina 59081459 PMC 1045688037629749 · doi ↗ · pubmed ↗
- 3Obstructive sleep apnea hypopnea syndrome and vascular lesions: an update on what we currently know Sleep Med Mao Z Zheng P Zhu X 29631111920243872357510.1016/j.sleep.2024.05.010 · doi ↗ · pubmed ↗
- 4Polycystic ovary syndrome in obstructive sleep apnea-hypopnea syndrome: an updated meta-analysis Front Endocrinol (Lausanne) He J Ruan X Li J 14189331520243924791410.3389/fendo.2024.1418933 PMC 11377251 · doi ↗ · pubmed ↗
- 5Unveiling the molecular and cellular links between obstructive sleep apnea-hypopnea syndrome and vascular aging Chin Med J (Engl) Liu W Zhang L Liao W 15517113820253964799110.1097/CM 9.0000000000003352 PMC 11745861 · doi ↗ · pubmed ↗
- 6Obstructive sleep apnea-hypopnea syndrome (OSAHS) in patients with acromegaly in Colombia Cureus Abreu Lomba A Montoya Ospina JM Vernaza Trujillo DA 017202510.7759/cureus.77557 PMC 1182980939958072 · doi ↗ · pubmed ↗
- 7Impact of comorbidities in COPD clinical control criteria. The CLAVE study BMC Pulm Med Almagro P Soler-Cataluña JJ Huerta A González-Segura D Cosío BG 62420243816696510.1186/s 12890-023-02758-0PMC 10759491 · doi ↗ · pubmed ↗
- 8Association of obstructive sleep apnea and nocturnal hypoxemia with the circadian rhythm of myocardial infarction J Am Heart Assoc Liu X Wang B Hao W 014202510.1161/JAHA.124.036729 PMC 1207474939868516 · doi ↗ · pubmed ↗