Associations between early tumor shrinkage/depth of response and survival from the ARCAD database
Hideaki Bando, Yuriko Takeda, Toshihiro Misumi, Tomomi Nishikawa, Masashi Wakabayashi, Kentaro Yamazaki, Eiji Oki, Jean-Yves Douillard, Cornelis J A Punt, Miriam Koopman, Eric Van Cutsem, Carsten Bokemeyer, Alan P Venook, Heinz-Josef Lenz, Yoshihiko Maehara, Thierry Andre

TL;DR
This study shows that early tumor shrinkage and depth of response are strong predictors of survival in patients with metastatic colorectal cancer treated with anti-EGFR or bevacizumab therapies.
Contribution
The study identifies optimal cutoff values for depth of response in anti-EGFR and bevacizumab therapies to predict survival outcomes in RAS wild-type metastatic CRC.
Findings
Early tumor shrinkage and depth of response significantly stratify survival outcomes across treatment groups.
Anti-EGFR therapy showed a trend toward better outcomes compared to bevacizumab-based therapy.
Optimal depth of response cutoffs of 0.55 and 0.47 predict a median overall survival of 32 months for anti-EGFR and bevacizumab therapies, respectively.
Abstract
Early tumor shrinkage and depth of response have emerged as potential prognostic indicators in metastatic colorectal cancer (CRC). However, their associations with overall survival, progression-free survival (PFS), and postprogression survival in patients receiving anti–epidermal growth factor receptor (EGFR) antibodies or bevacizumab remain unclear. We analyzed 3219 treatment-naive patients with RAS wild-type metastatic CRC from 8 randomized studies (CRYSTAL, OPUS, PRIME, CAIRO2, CALGB80405, WJOG4407G, ATOM, PARADIGM) in the Aid and Research in Digestive Cancerology database. Early tumor shrinkage was defined as a 20% or more reduction in tumor size at 8 ± 2 weeks, whereas depth of response was assessed by maximum tumor shrinkage at nadir. Cox regression models evaluated the associations of early tumor shrinkage and depth of response with overall survival, PFS, and postprogression…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
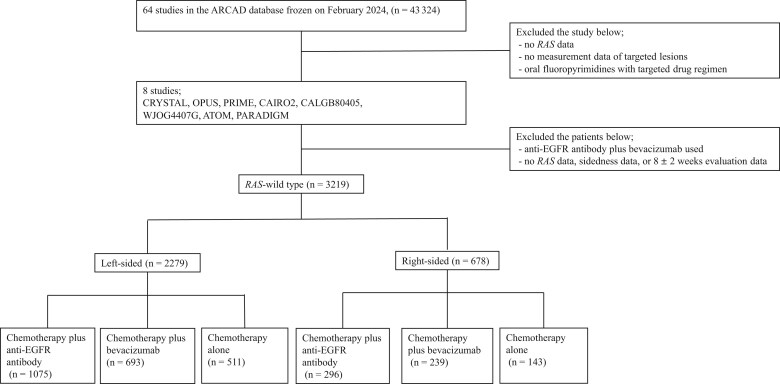 Figure 1
Figure 1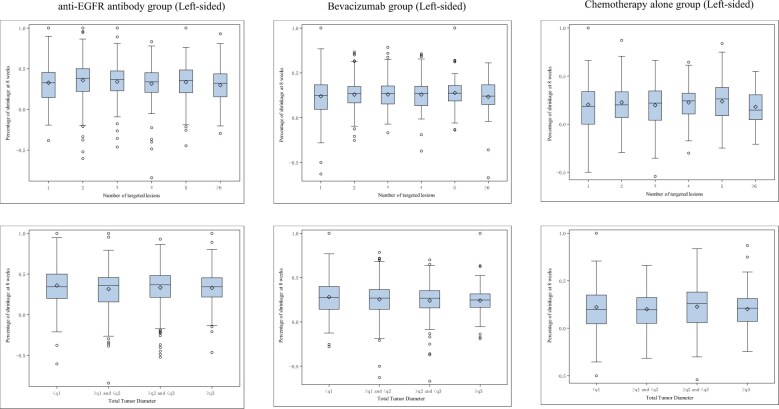 Figure 2
Figure 2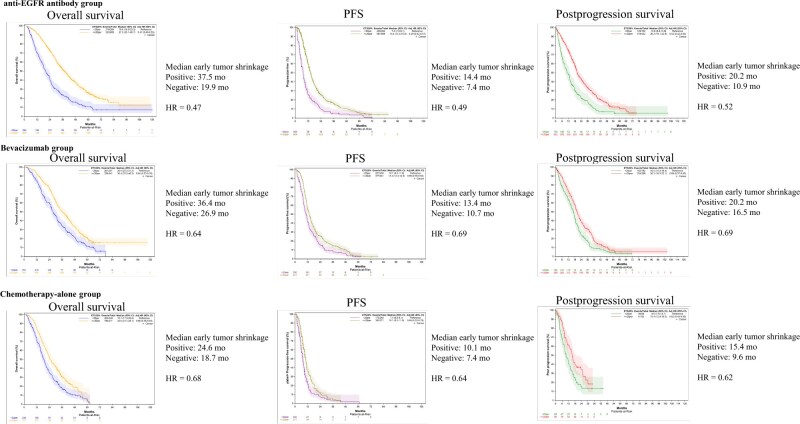 Figure 3
Figure 3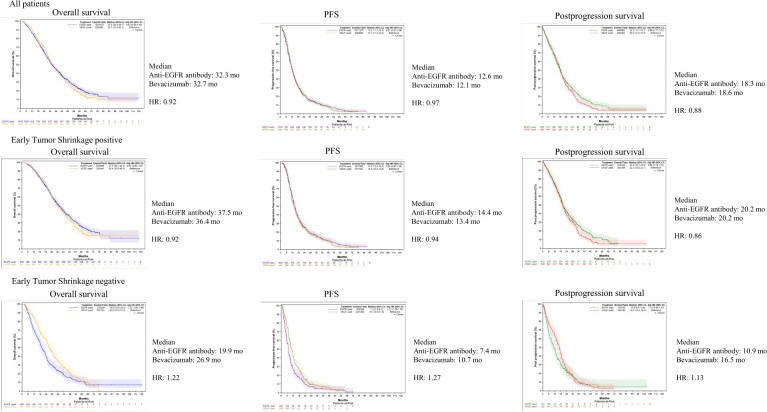 Figure 4
Figure 4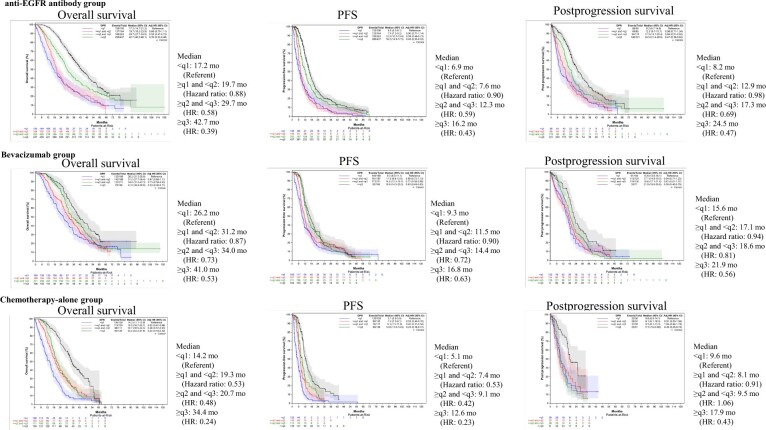 Figure 5
Figure 5| Study | Evaluation criteria | First assessment, wk | Study treatment | Patients randomly assigned, No. |
|
|---|---|---|---|---|---|
| CRYSTAL | World Health Organization | 8 ± 2 | FOLFIRI + cetuximab | 610 | 259 |
| FOLFIRI | 611 | 300 | |||
| OPUS | World Health Organization | 8 ± 2 | FOLFOX + cetuximab | 173 | 73 |
| FOLFOX | 171 | 86 | |||
| PRIME (C203) | RECIST 1.0 | 8 ± 2 | FOLFOX4 | 590 | 268 |
| FOLFOX4 + panitumumab | 593 | 247 | |||
| CAIRO2 | RECIST 1.0 | 9 ± 2 | oxaliplatin and capecitabine + bevacizumab | 378 | 95 |
| CALGB-80405 | RECIST 1.0 | 8 ± 2 | Chemotherapy + bevacizumab | 897 | 389 |
| Chemotherapy + cetuximab | 897 | 406 | |||
| WJOG4407G | RECIST 1.0 | 8 ± 2 | FOLFOX + bevacizumab | 200 | 30 |
| FOLFIRI + bevacizumab | 202 | 34 | |||
| ATOM | RECIST 1.1 | 8 ± 2 | Modified FOLFOX6 + bevacizumab | 61 | 56 |
| Modified FOLFOX6 + cetuximab | 61 | 58 | |||
| PARADIGM | RECIST 1.1 | 8 ± 2 | Modified FOLFOX6 + panitumumab | 411 | 328 |
| Modified FOLFOX6 + bevacizumab | 412 | 328 |
- —National Cancer Center Research and Development Fund
- —ARCAD Foundation
- —ARCAD Asia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Treatments and Studies · Genetic factors in colorectal cancer · Cancer Genomics and Diagnostics
Introduction
In 2020, colorectal cancer (CRC) ranked as the third-most prevalent cancer worldwide in terms of new cases, with 1 148 515 cases diagnosed in the colon and 732 210 cases diagnosed in the rectum. In addition, CRC was the second-leading cause of cancer-related deaths globally, with 935 000 deaths attributed to colon cancer and 339 022 to rectal cancer.1
According to guidelines from the European Society for Medical Oncology, the adapted European Society for Medical Oncology Pan-Asian guidelines, and the American Society of Clinical Oncology, the preferred therapy for patients with KRAS, NRAS, and BRAF wild-type left-sided metastatic CRC involves combining 5-fluorouracil and leucovorin with oxaliplatin (FOLFOX) or irinotecan (FOLFIRI), alongside an anti–epidermal growth factor receptor (EGFR) antibody (cetuximab or panitumumab).2-4 This recommendation is based on a meta-analysis of 6 randomized trials.5 Furthermore, the Japanese PARADIGM trial demonstrated the superiority of first-line modified FOLFOX6 plus panitumumab over modified FOLFOX6 plus bevacizumab in populations with KRAS/NRAS wild-type left-sided primary tumors, establishing the use of first-line FOLFOX plus an anti-EGFR antibody in this subgroup.6 For patients presenting with KRAS and NRAS mutations; BRAF V600E mutations; or KRAS, NRAS, and BRAF wild-type right-sided disease, the preferred therapy is a doublet (eg, FOLFOX or FOLFIRI or oxaliplatin plus capecitabine) or triplet (oxaliplatin plus irinotecan plus 5-fuluorouracil and leucovorin) combined with anti–vascular endothelial growth factor antibody (bevacizumab).3^,^7
In CRC, the effectiveness of systemic treatments is typically assessed using objective response rate, progression-free survival (PFS), and overall survival. Although overall survival serves as the primary measure for evaluating the efficacy of a new therapy, PFS is considered an early endpoint and frequently used as a reliable surrogate for overall survival. However, beyond a median overall survival of 30 months and a median PFS of 10 months, the impact of postprogression treatment becomes more substantial, raising questions about the reliability of PFS as a predictor of overall survival.8^,^9 Indeed, past phase 3 trials comparing chemotherapy plus an anti-EGFR antibody with chemotherapy plus bevacizumab reproducibly demonstrated a clinically significant difference in overall survival, despite no difference being observed in PFS.6^,^8^,^9 Therefore, alternative surrogate endpoints for overall survival that measure the direct effect of the agents used on tumor size are currently being discussed.
Early assessment of tumor reduction may serve as a valuable tool in guiding treatment strategies during the initial restaging phase. Recently, early tumor shrinkage has garnered attention among clinicians as a promising prognostic indicator for overall survival in patients with metastatic CRC undergoing first-line therapy.10-15 Although early tumor shrinkage, akin to any response to anticancer therapy, represents a continuous parameter, a cutoff-based assessment has been introduced to delineate early tumor shrinkage–positive cases from early tumor shrinkage–negative cases. Although the optimal cutoff values and timing for early tumor shrinkage assessment have yet to be precisely defined, 8 weeks after initiating therapy and a tumor shrinkage of 20% or more are likely to be established, regardless of the regimen.10-15 In addition, depth of response, which signifies the maximum observed tumor reduction in a patient, has emerged as a continuous efficacy metric with potential implications for predicting long-term treatment outcomes.11-14^,^16-18
For CRC, individual patient data from clinical trials concerning metastatic CRC have been shared across Europe, Japan, and the United States through the Aid and Research in Digestive Cancerology (ARCAD) Foundation database project since 2006.19 The CRC ARCAD global database project has been established as a comprehensive repository of historical individual patient data, encompassing information from more than 43 324 patients across more than 64 studies worldwide, and it continues to expand. These trials have been sponsored by various entities, including industry, governments, and academic groups, ensuring the inclusion of high-quality clinical data.19^,^20 In this study, we evaluated the potential of early tumor shrinkage and depth of response as surrogate endpoints for overall survival and postprogression survival, defined as survival following first-line therapy, in patients treated with chemotherapy plus an anti-EGFR antibody or bevacizumab.
Methods
Patient selection and study cohort
From the individual patient data extracted from 64 studies within the ARCAD metastatic CRC database, we selected a cohort of treatment-naive patients diagnosed with unresectable RAS wild-type metastatic CRC who subsequently received either chemotherapy combined with an anti-EGFR antibody or bevacizumab or chemotherapy alone.
Definition and assessment of early tumor shrinkage and depth of response
In this analysis, early tumor shrinkage was defined as a reduction in tumor size of 20% or more at 8 ± 2 weeks. Cases were categorized as early tumor shrinkage positive if the patients achieved a reduction of 20% or greater in the sum of the sizes of targeted lesions and as early tumor shrinkage negative if the reduction was less than 20%. Depth of response was defined as the maximum percentage reduction in targeted lesions from baseline following treatment. To validate the reliability of early tumor shrinkage and depth of response as tumor evaluation metrics, we summarize these measures based on the number of tumor lesions and the total tumor diameter.
Statistical analysis
The impact of early tumor shrinkage positivity and negativity, depth of response, and the use of anti-EGFR antibodies and bevacizumab on overall survival, PFS, and postprogression survival was assessed using multivariate Cox regression analysis, adjusted for age, sex, and ECOG-ACRIN performance status. Depth of response was evaluated across each quantile of the maximum percentage reduction. Survival analyses were conducted using the Kaplan-Meier method to generate survival curves and estimate median survival times. In these analyses, the starting point was the date of random assignment; overall survival was defined as the time from random assignment to death from any cause, PFS was defined as the time from random assignment to disease progression or death from any cause, and postprogression survival was defined as the time from the date of progression after first-line therapy to death from any cause for patients who experienced disease progression during first-line therapy. To determine the optimal cutoff value for depth of response and its corresponding sensitivity and specificity, receiver operating characteristic curve analysis using the Youden index was performed. The hazard ratio (HR) for overall survival was calculated for each percentage cutoff using multivariate Cox regression analysis, adjusted for age, sex, and ECOG-ACRIN performance status. All analyses were prespecified, and a 2-sided test was conducted with a significance level of .05. However, no adjustments for multiplicity were made due to the exploratory nature of the study. Statistical analyses were performed using SAS, version 9.4, statistical software (SAS Institute Inc).
Ethical approval and compliance
The clinical protocol was approved by the Institutional Review Board of the National Cancer Center Japan (Protocol No. 2021-096 and 2021-192). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Patient selection and background
We extracted individual patient data from 64 studies within the ARCAD metastatic CRC database. Patients were selected from 8 randomized trials (CRYSTAL, OPUS, PRIME, CAIRO2, CALGB80405, WJOG4407G, ATOM, and PARADIGM) that involved first-line therapy and conducted the initial tumor evaluation at 8 ± 2 weeks, excluding trials that used oral fluoropyrimidine-based treatments (Table 1). Among these cases, we excluded those without data on RAS status, tumor sidedness, or target lesion measurements; those whose tumor evaluations were not performed at 8 ± 2 weeks; and where the participants were treated with an anti-EGFR antibody plus bevacizumab. Finally, a total of 3219 patients with confirmed RAS wild-type tumors were enrolled, of whom 2279 had left-sided tumors and 678 had right-sided tumors (Figure 1).
Patient selection CONSORT diagram. This diagram outlines the process of patient selection across 8 studies (CRYSTAL, OPUS, PRIME, CAIRO2, CALGB80405, WJOG4407G, ATOM, and PARADIGM) included in the ARCAD database. A total of 3219 patients with RAS wild-type metastatic colorectal cancer were analyzed, categorized by tumor sidedness and treatment (chemotherapy plus anti-EGFR antibody, chemotherapy plus bevacizumab, or chemotherapy alone). ARCAD = Aid and Research in Digestive Cancerology; EGFR = epidermal growth factor receptor.
Patient characteristics for patients treated with chemotherapy plus an anti-EGFR antibody and for patients treated with chemotherapy plus bevacizumab were comparable with respect to ECOG-ACRIN performance status, sex, age at enrollment, carcinoembryonic antigen levels, sum of target lesion diameters, presence of liver metastasis, number of metastatic sites, BRAF mutation, and surgical history. The rate of missingness was less than 5% for each variable, except for metastatic sites, carcinoembryonic antigen levels, and BRAF mutation, which were not collected in the original study (Tables S1 and S2).
Summary of early tumor shrinkage and depth of response by tumor lesion count and total tumor diameter
In this analysis, 766 cases were evaluated using the World Health Organization criteria21; 1676 cases using Response Evaluation Criteria in Solid Tumors (RECIST), version 1.0, criteria22; and 777 cases using RECIST, version 1.1, criteria.23 Given the potential for variability in the number of lesions assessed under each criterion, we first examined whether early tumor shrinkage and depth of response differed based on the number of tumor lesions or the total tumor diameter. Among patients treated with chemotherapy plus an anti-EGFR antibody (anti-EGFR antibody group), chemotherapy plus bevacizumab (bevacizumab group), and chemotherapy alone (chemotherapy-alone group), the median early tumor shrinkage was 0.3 to 0.4 in the anti-EGFR antibody group, 0.2 to 0.3 in the bevacizumab group, and 0.2 to 0.3 in the chemotherapy-alone group, regardless of the number of baseline targeted lesions or total tumor diameter (Figure 2). Furthermore, irrespective of the number of baseline targeted lesions or total tumor diameter, the median depth of response was 0.5 to 0.7 in the anti-EGFR antibody group, 0.4 to 0.5 in the bevacizumab group, and 0.4 to 0.5 in the chemotherapy-alone group (Figure S1). We examined whether early tumor shrinkage and depth of response differed based on the presence or absence of liver metastases and found that liver metastasis status did not affect the assessment of early tumor shrinkage and depth of response (Tables S3 and S4). For peritoneal dissemination and lung metastases, a high rate of missing data prevented us from conducting a valid analysis.
Correlations between early tumor shrinkage and baseline targeted lesions/total tumor diameter. The figure illustrates the relationship between early tumor shrinkage and the number of baseline targeted lesions or total tumor diameter. Data are presented for 3 treatment groups (anti–epidermal growth factor receptor [EGFR] antibody, bevacizumab, and chemotherapy alone), showing the percentage of tumor shrinkage at 8 weeks in left-sided tumors.
Correlations between early tumor shrinkage and survival
To evaluate the statistical significance of achieving early tumor shrinkage, we first examined its implications in the anti-EGFR antibody group, in the bevacizumab group, and in the chemotherapy-alone group. Our findings suggest that early tumor shrinkage in patients with RAS wild-type metastatic CRC may serve as a prognostic marker for overall survival, PFS, and postprogression survival, irrespective of the type of targeted therapy used or the primary tumor location (Figure 3, Figure S2). Specifically, in patients with left-sided RAS wild-type metastatic CRC, the hazard ratios for early tumor shrinkage–positive cases compared with early tumor shrinkage–negative cases in the anti-EGFR antibody group were as follows: overall survival, 0.47 (95% confidence interval [CI] = 0.40 to 0.55); PFS, 0.49 (95% CI = 0.42 to 0.57); and postprogression survival, 0.52 (95% CI = 0.42 to 0.64). For the bevacizumab group, the hazard ratios were as follows: overall survival, 0.64 (95% CI = 0.53 to 0.76); PFS, 0.69 (95% CI = 0.59 to 0.82); and postprogression survival, 0.69 (95% CI = 0.57 to 0.85). In the chemotherapy-alone group, the hazard ratios were as follows: overall survival, 0.68 (95% CI = 0.56 to 0.83); PFS, 0.64 (95% CI = 0.52 to 0.79); and postprogression survival, 0.62 (95% CI = 0.43 to 0.90) (Figure 3). When comparing survival outcomes across different regimens, patients treated with chemotherapy plus an anti-EGFR antibody exhibited a trend toward better hazard ratios for overall survival, PFS, and postprogression survival compared with patients treated with chemotherapy plus bevacizumab or chemotherapy alone. This finding suggests a potential relationship between early tumor shrinkage and improved survival outcomes (Figure 3).
The correlations between early tumor shrinkage and survival in left-sided tumors. This figure demonstrates the correlation between early tumor shrinkage and survival outcomes (overall survival, progression-free survival [PFS], and postprogression survival) in left-sided RAS wild-type tumors. Early tumor shrinkage–positive patients showed improved overall survival, PFS, and postprogression survival across all treatment groups (anti–epidermal growth factor receptor [EGFR] antibody, bevacizumab, and chemotherapy alone), with hazard ratios (HRs) favoring early tumor shrinkage positivity.
Next, we compared the significance of early tumor shrinkage between patients treated with chemotherapy plus an anti-EGFR antibody and patients treated with chemotherapy plus bevacizumab. In patients with left-sided RAS wild-type early tumor shrinkage–positive metastatic CRC, there were no statistically significant differences in overall survival, PFS, or postprogression survival between anti-EGFR–based therapy and bevacizumab-based therapy (overall survival, HR = 0.92 [95% CI = 0.80 to 1.05]; PFS, HR = 0.94 [95% CI = 0.83 to 1.08]; postprogression survival, HR = 0.86 [95% CI = 0.73 to 1.02]). In contrast, in early tumor shrinkage–negative patients on bevacizumab-based therapy showed a trend toward better overall survival, PFS, and postprogression survival outcomes compared with patients on anti-EGFR–based therapy (overall survival, HR = 1.22 [95% CI = 1.00 to 1.48]; PFS, HR = 1.27 [95% CI = 1.05 to 1.53]; postprogression survival, HR = 1.13 [95% CI = 0.90 to 1.43]). These trends were consistent with patients with right-sided RAS wild-type metastatic CRC (Figure 4, Figure S3).
Correlations between early tumor shrinkage and treatment efficacy in left-sided tumors. The figure compares the efficacy of anti-EGFR antibody and bevacizumab treatments in early tumor shrinkage–positive and early tumor shrinkage–negative patients with left-sided tumors. Early tumor shrinkage–positive patients demonstrated similar overall survival, PFS, and postprogression survival between both treatment types, whereas early tumor shrinkage–negative patients treated with bevacizumab showed better survival outcomes. EGFR = epidermal growth factor receptor; HR = hazard ratio; PFS = progression-free survival.
Correlations between depth of response and survival
To evaluate the significance of depth of response, we examined its implications in the left-sided anti-EGFR antibody group, the bevacizumab group, and chemotherapy-alone group, referencing the hazard ratio of each quantile of the maximum percentage reduction to the first quantile (q). In the anti-EGFR antibody group, the hazard ratios for overall survival were as follows: ≥q1 and <q2, 0.88 (95% CI = 0.70 to 1.11); ≥q2 and <q3, 0.58 (95% CI = 0.47 to 0.72); and ≥q3, 0.39 (95% CI = 0.32 to 0.48) compared with <q1. For PFS, the hazard ratios were 0.90 (95% CI = 0.71 to 1.14), 0.59 (95% CI = 0.48 to 0.73), and 0.43 (95% CI = 0.35 to 0.52). For postprogression survival, the hazard ratios were 0.98 (95% CI = 0.71 to 1.34), 0.69 (95% CI = 0.51 to 0.93), and 0.47 (95% CI = 0.36 to 0.62). In the bevacizumab group, the hazard ratios for overall survival were as follows: ≥q1 and <q2, 0.87 (95% CI = 0.68 to 1.11); ≥q2 and <q3, 0.73 (95% CI = 0.58 to 0.93); and ≥q4, 0.53 (95% CI = 0.40 to 0.71). The hazard ratios for PFS were 0.90 (95% CI = 0.72 to 1.13), 0.72 (95% CI = 0.58 to 0.90), and 0.63 (95% CI = 0.49 to 0.83). For postprogression survival, the hazard ratios were 0.94 (95% CI = 0.71 to 1.25), 0.81 (95% CI = 0.61 to 1.07), and 0.56 (95% CI = 0.40 to 0.79). In the chemotherapy-alone group, the hazard ratios for overall survival were as follows: ≥q1 and <q2, 0.53 (95% CI = 0.41 to 0.68); ≥q2 and <q3, 0.48 (95% CI = 0.37 to 0.63); and ≥q4, 0.24 (95% CI = 0.18 to 0.32). The hazard ratios for PFS were 0.53 (95% CI = 0.40 to 0.70), 0.42 (95% CI = 0.31 to 0.56), and 0.23 (95% CI = 0.18 to 0.31). For postprogression survival, the hazard ratios were 0.91 (95% CI = 0.53 to 1.56), 1.06 (95% CI = 0.64 to 1.74), and 0.43 (95% CI = 0.25 to 0.74). In patients with left-sided RAS wild-type metastatic CRC, depth of response was demonstrated to be a prognostic marker for overall survival, PFS, and postprogression survival, with survival curves showing clear stratification based on depth of response. These trends were consistent with patients with right-sided RAS wild-type metastatic CRC (Figure 5, Figure S4).
Correlations between depth of response and survival in left-sided tumors. This figure highlights the correlation between the depth of response and survival outcomes (overall survival, PFS, and postprogression survival) in left-sided tumors, stratified by treatment type (anti-EGFR antibody, bevacizumab, and chemotherapy alone). Patients with a greater depth of response experienced statistically significantly improved survival, with clear stratification across treatment groups. EGFR = epidermal growth factor receptor; HR = hazard ratio; PFS = progression-free survival; q = quantile.
Next, we calculated the depth of response required to achieve the median overall survival in patients treated with chemotherapy combined with an anti-EGFR antibody and patients treated with chemotherapy combined with bevacizumab. In patients with left-sided disease receiving anti-EGFR–based therapy, the receiver operating characteristic curve–derived cutoff value to reach a median overall survival of 31.9 months was 0.55 (area under the curve = 0.70, sensitivity = 0.63, specificity = 0.68). For patients receiving bevacizumab-based therapy, the cutoff value to achieve a median overall survival of 32.7 months was 0.47 (area under the curve = 0.66, sensitivity = 0.73, specificity = 0.52) (Figure S5). These cutoff values for depth of response, as identified by the receiver operating characteristic curve, effectively stratified patients with improved overall survival, PFS, and postprogression survival. Furthermore, patients treated with chemotherapy plus an anti-EGFR antibody exhibited a trend toward better hazard ratios for overall survival, PFS, and postprogression survival compared with patients treated with chemotherapy plus bevacizumab or chemotherapy alone (Figure S5).
Discussion
Although several literature-based meta-analyses have been published on the clinical efficacy of early tumor shrinkage and depth of response in patients with metastatic CRC,13^,^24 to the best of our knowledge, this study represents the largest investigation to date using individual patient data to examine the association between early tumor shrinkage and depth of response with overall survival, PFS, and postprogression survival in the context of chemotherapy combined with anti-EGFR antibodies or bevacizumab, according to tumor sidedness in patients with RAS wild-type metastatic CRC. In addition, our analysis encompasses evaluations conducted using various criteria, including World Health Organization and RECIST, versions 1.0 and 1.1, reflecting changes over time. The World Health Organization criteria allow for a maximum of 2 target lesions per organ and 5 target lesions in total, whereas RECIST, version 1.0, permits up to 5 target lesions per organ and 10 target lesions in total. RECIST, version 1.1, however, revised these criteria to allow a maximum of 2 target lesions per organ and 5 target lesions in total. In our analysis, we used the longest diameter measurements and demonstrated that early tumor shrinkage and depth of response consistently serve as reliable assessment metrics, maintaining stable values regardless of the number of tumor lesions, total tumor diameter, or the presence of liver metastases. Given the ability of early tumor shrinkage and depth of response to predict survival outcomes without incurring additional costs for data collection, we believe that these metrics should be actively used not only in clinical trials but also in routine clinical practice.
Although early tumor shrinkage and depth of response were shown to be strongly associated with survival outcomes, irrespective of the type of targeted therapy used or the primary tumor location, the findings were particularly pronounced in patients treated with chemotherapy plus an anti-EGFR antibody. These results suggest that a higher rate of early tumor shrinkage and a deeper depth of response are associated with statistically significantly better survival. Notably, in ultraselect patients with right-sided tumors characterized by specific gene alterations (RAS/BRAF/EGFR ectodomain wild type), early tumor shrinkage and depth of response may serve as prognostic markers for chemotherapy plus anti-EGFR antibody treatment. In our dataset, among patients with right-sided, RAS/BRAF wild-type disease treated chemotherapy plus anti-EGFR antibodies, the hazard ratios for early tumor shrinkage positivity and for depth of response in the highest quantile (≥Q3) were more favorable than those observed in patients treated with bevacizumab or chemotherapy alone (Table S5). Furthermore, although the current standard treatment for RAS wild-type left-sided metastatic CRC is chemotherapy plus an anti-EGFR antibody, our analysis revealed that patients who did not achieve early tumor shrinkage had worse overall survival, PFS, and postprogression survival compared with patients treated with chemotherapy plus bevacizumab. The ability to determine at the 8-week mark whether anti-EGFR antibody–based therapy may be unsuitable and potentially associated with shorter overall survival is crucial for making informed decisions regarding the continuation of treatment, independent of gene alterations. Although the present analysis alone does not allow us to conclude whether switching to bevacizumab-based therapy at the 8-week mark is appropriate, the possibility of a shorter PFS should be anticipated, and clinicians should be prepared to promptly transition to the next line of treatment, if necessary.
It was also demonstrated that depth of response, irrespective of the type of targeted therapy or the primary tumor location, serves as a robust indicator capable of effectively stratifying patient survival outcomes. Although the sensitivity and specificity of depth of response as a predictive marker may not be exceptionally high, our analysis revealed that the depth of response required to achieve the median overall survival was 55% for anti-EGFR antibody–based therapy and 47% for bevacizumab-based therapy (Figure S5). For both anti-EGFR antibody–based therapy and bevacizumab-based therapy, the area under the curve values were not particularly high, making it difficult to consider the model as ideal. However, considering the balance between sensitivity and specificity, it may serve as a useful indicator. In addition, achieving a deep response during first-line treatment can be considered a major factor influencing subsequent survival duration.
This study had several limitations. First, BRAF mutation status was unavailable in more than half the cases, and microsatellite instability status was missing in the majority of patients, precluding evaluation of their impact on survival outcomes. Second, due to the lack of information about the organs assessed as target lesions, we were unable to analyze the influence of metastatic sites on early tumor shrinkage and depth of response. Furthermore, information about second-line and later-line therapies was incomplete due to the follow-up framework of the clinical trials, limiting our ability to assess their impact on overall survival. Although this study represents the most precise meta-analysis to date using individual patient data, limitations remain in fully evaluating the impact of early tumor shrinkage and depth of response on survival. The interpretation of these results must consider recent advances in treatment that have expanded subsequent therapeutic options, and the fact that this analysis is based on a select population from prospective randomized controlled trials focusing on patients with RAS wild-type disease facilitated by improved diagnostic accuracy. Nevertheless, the ability to obtain a prognostic indicator without incurring additional costs is valuable.
In conclusion, this study is the largest to date using individual patient data to assess early tumor shrinkage and depth of response as prognostic markers in metastatic CRC. Our findings confirm that early tumor shrinkage and depth of response are robust indicators of overall survival, PFS, and postprogression survival, regardless of targeted therapy or tumor location. Notably, patients who did not achieve early tumor shrinkage had worse outcomes with anti-EGFR therapy than with bevacizumab. These results suggest that early tumor shrinkage and depth of response are valuable tools for guiding treatment strategies and should be integrated into clinical trials and routine practice to optimize patient outcomes.
Supplementary Material
pkaf042_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H , Ferlay J, Siegel RL, et al Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209-249. 10.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Cervantes A , Adam R, RosellóS, et al ESMO Guidelines Committee. Electronic address: [email protected]. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34:10-32. 10.1016/j.annonc.2022.10.00336307056 · doi ↗ · pubmed ↗
- 3Yoshino T , Arnold D, Taniguchi H, et al Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: a JSMO-ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann Oncol. 2018;29:44-70.29155929 10.1093/annonc/mdx 738 · doi ↗ · pubmed ↗
- 4Morris VK , Kennedy EB, Baxter NN, et al Treatment of metastatic colorectal cancer: ASCO guideline. J Clin Oncol. 2023;41:678-700. 10.1200/JCO.22.0169036252154 PMC 10506310 · doi ↗ · pubmed ↗
- 5Arnold D , Lueza B, Douillard JY, et al Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann Oncol. 2017;28:1713-1729. 10.1093/annonc/mdx 17528407110 PMC 6246616 · doi ↗ · pubmed ↗
- 6Watanabe J , Muro K, Shitara K, et al Panitumumab vs bevacizumab added to standard first-line chemotherapy and overall survival among patients with RAS wild-type, left-sided metastatic colorectal cancer: a randomized clinical trial. [published correction appears in JAMA. 2023 Jun 27; 329(24):2196. doi:10.1001/jama.2023.10533]. JAMA. 2023;329:1271-1282. 10.1001/jama.2023.442837071094 PMC 10114040 · doi ↗ · pubmed ↗
- 7Van Cutsem E , Cervantes A, Adam R, et al ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27:1386-1422. 10.1093/annonc/mdw 23527380959 · doi ↗ · pubmed ↗
- 8Venook AP , Niedzwiecki D, Lenz HJ, et al Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced or metastatic colorectal cancer: a randomized clinical trial. JAMA. 2017;317:2392-2401. 10.1001/jama.2017.710528632865 PMC 5545896 · doi ↗ · pubmed ↗