Thyroid cancer surgical indication during pregnancy: Systematic literature review and series of illustrative cases
Lucas Albuquerque Chinelatto, Flávio Carneiro Hojaij, Dorival de Carlucci, Claudio Roberto Cernea

TL;DR
This paper reviews when to perform thyroid cancer surgery during pregnancy, suggesting second-trimester surgery for severe cases and post-delivery for less severe ones.
Contribution
The study provides clinical guidance on thyroidectomy timing during pregnancy based on tumor severity and patient safety.
Findings
Surgery during the second trimester is suitable for aggressive thyroid cancers with lymph node metastasis.
Postpartum surgery is safer for less severe cases to reduce risks to the fetus and mother.
Recent studies support flexibility in performing thyroidectomy during the second trimester.
Abstract
•There is no literature consensus about the better time to perform thyroidectomy in pregnant patients with thyroid cancer.•Surgery in the second trimester should be considered for the most severe cases, such as those that present lymph node metastasis or effective nodule growth within the first weeks of pregnancy.•In less severe cases, it is safer to perform thyroidectomy after delivery, decreasing the risks related to surgery to the patient and the fetus. There is no literature consensus about the better time to perform thyroidectomy in pregnant patients with thyroid cancer. Surgery in the second trimester should be considered for the most severe cases, such as those that present lymph node metastasis or effective nodule growth within the first weeks of pregnancy. In less severe cases, it is safer to perform thyroidectomy after delivery, decreasing the risks related to surgery to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
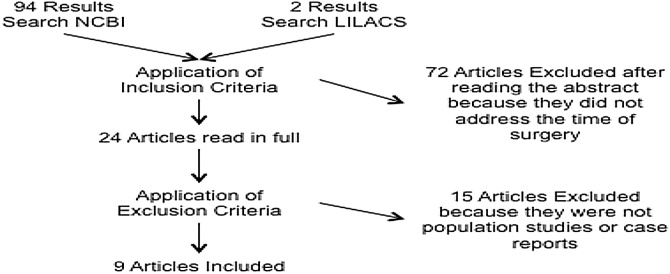 Figure 1
Figure 1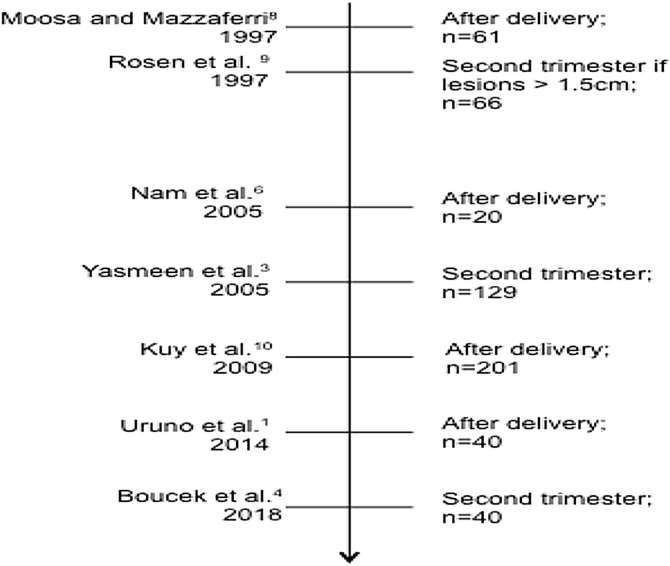 Figure 2
Figure 2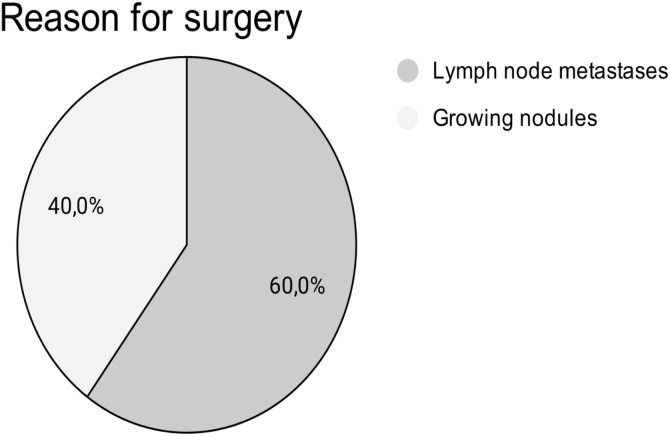 Figure 3
Figure 3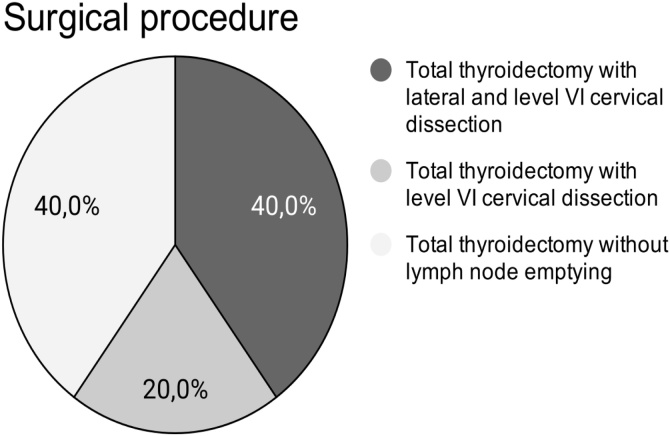 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Cancer Risks and Factors · Radiation Dose and Imaging
Introduction
Thyroid cancer is the second most frequently found type of cancer during pregnancy.1, 2 Its estimated incidence is 14 cases per 100,000 deliveries, with peak incidence in the 25‒30-year age group.3, 4 Papillary carcinoma is the main histology in this type of cancer.3, 4 Diagnosis is performed by Fine Needle Aspiration Biopsy (FNAB), which is indicated after finding altered values in routine prenatal examinations, such as those of TSH and free T4, and the manifestation of symptoms is uncommon.5
Diagnosis of thyroid cancer during pregnancy brings insecurity and fear to patients,4, 6, 7 which makes updated medical knowledge on the subject fundamental for a correct surgical clinical approach.
The present study reports five cases of surgical approach to thyroid cancer in the second trimester of pregnancy and their respective outcomes. In order to better support the discussion, a systematic literary review was carried out on a chronological perspective. The objective of this study is to evaluate whether there is consensus on the correct time to approach papillary thyroid carcinoma in pregnant patients and discuss the accepted approaches according to the literature.
Methods
The systematic review used the following descriptors in the title or abstract of the publications as a search criterion: “Thyroid” “Surgery” and “Pregnant” [((Thyroid[Title/Abstract]) AND Surgery[Title/Abstract]) AND Pregnant [Title/Abstract]]. An online search was conducted at the Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS) and the National Center for Biotechnology Information (NCBI) databases because they are the main databases used in the medical literature. The search was carried out on March 22, 2019 and the abstracts were analyzed for the selection of articles. Inclusion criteria comprised optimal timing to perform thyroidectomy in pregnant patients and outcome evaluation. The following exclusion criteria were adopted: publications other than in English, Portuguese or Spanish; articles not available online; articles other than population studies or case reports. A total of nine articles were analyzed, according to the flowchart in Fig. 1.Fig. 1. Flowchart of the inclusion and exclusion processes of the studies. Ninety-eight abstracts were analyzed, with final inclusion of nine articles.Fig. 1
A retrospective analysis of thyroidectomies was performed in patients in the second trimester of pregnancy between 1999 and 2019. The series includes cases selected by surgical indication due to the presence of a growing nodule or lymph node metastasis. Intravenous anesthesia with propofol and remifentanil was used in all cases. The option for neck dissection was guided by lymph node involvement. All cases are from the authors’ private practice. Data were processed using Microsoft® Excel® for Mac 2011 14.7.7.
Results
Of the 25 articles read, nine were case reports or population studies. Table 1 shows these articles and their main outcomes. Fig. 2 presents a timeline of the population studies analyzed based on the publication date. It shows that the possibility of indicating surgery in the second trimester of pregnancy, regardless of case severity, is more recent. Even so, there has been no complete change in the indication pattern, as observed in the studies by Kuy et al.10 and Uruno et al.1 Table 2 presents the studies separated according to their conclusions on the time to indicate surgery, evidencing that constant divergence still exists regarding this topic.Table 1. Systematic review results. Characteristics of the selected studies in chronological order of publication.Table 1. AuthorsMethodologyStudy sampleTime of thyroidectomy: number of patientsMorbidities and deathsConclusionMoosa and Mazzaferri8Cohort of patients treated at the United States Air Force or the Ohio State University Hospitals61 patients with thyroid cancer during pregnancy1^st^ trimester: 1There was no statistical difference between groupsSurgery can be performed after delivery, not delaying it for more than 1-year after delivery2^nd^ trimester: 123^rd^ trimester: 1After delivery: 47Rosen et al9Retrospective study: 1982‒199766 patients with thyroid cancer during pregnancy20^nd^ trimester: 14There was no statistical difference between groupsPerform total thyroidectomy in the 22-weeks when nodule > 1.5 cm.After delivery: 37Nam et al6Retrospective case study: 1991‒200420 patients with thyroid cancer during pregnancy2^nd^ trimester: 6There was no statistical difference between groupsSurgery after delivery can generate anxiety, affecting breastfeeding and quality of careAfter delivery: 9Abortions: 5 (non-pathology-related)Yasmeen et al3Retrospective cohort study: 1991 and 1999595, cases of thyroid cancer. 129 cases during pregnancy2^nd^ trimester: 96There was no statistical difference between groupsPerform surgery after delivery, not delaying it for more than 1-year as it may increase mortalityDuring delivery: 1After delivery: 26Kux et al10Retrospective cross-sectional study: 1999‒2005201 pregnant women compared to 31,155 non-pregnant womenNot specifiedThere was no statistical difference between groupsOperate cases in the 2^nd^ trimesterGietka- Czernel et al11Case report ‒ Department of Endocrinology of a hospital in Warsaw, Poland1 patient at the 21 week of gestationEmergency thyroidectomy performed in the 2^nd^ trimesterThere was no statistical difference between groupsDue to higher costs and longer hospital stay, it is better to operate after deliveryUruno et al1Retrospective review 1989‒201145 patients with thyroid cancer during pregnancy20^nd^ trimester: 24There was no statistical difference between groupsSurgery after deliveryAfter delivery: 21Ismi et al12Case report1 patient at 23-week of gestation with a neck mass of 3 cm, growingTotal thyroidectomy in the 2^nd^ trimester + Total lymphadenectomyThere was no statistical difference between groupsOperate after delivery. In cases of rapid nodule growth, compressive symptoms, spinal cord or affected lymph node metastases, thyroidectomy should be performed in the 2^nd^ trimesterBoucek et al4International observational cohort. Patients registered between June 2004 and October 201640 patients with thyroid cancer during pregnancy 5 excluded for cancer not being well-differentiated20^nd^ trimester: 293 abortions: 1 due to fetal malformation and 2 by maternal desireOperate in the 2^nd^ trimester. Waiting tox childbirth can increase maternal psychological stress during pregnancyAfter delivery: 6Fig. 2Flowchart with chronological order of publication of the population studies on thyroid cancer in pregnancy. On the right, study conclusion about the time to perform surgery and the study sample (n).Fig. 2. Table 2Classification of the articles analyzed in the systematic review according to their conclusions regarding best time for surgery.Table 2. Second TrimesterAfter deliveryAny caseOnly cases considered serious according to author discretionYasmeen et al3Rosen et al9Moosa and Mazzaferri8Boucek et al4Gietka-Czernel et al11Nam et al6Ismi et al12Kuy et al10Uruno et al 1
In our experience, we present five case reports surgically addressed during the second trimester of pregnancy, referring to all cases performed by our team at this time of pregnancy (Table 3). As it can be observed in Fig. 3, Fig. 4, surgeries were indicated because of lymph node metastasis or growing nodule. In one of the five cases, the recorded growth was from 1 to 2.5 cm in two months. The decision for surgery in the second trimester was agreed between patient, obstetrician, endocrinologist, and surgeon. No cases presented fetal, anesthetic, or surgical complications. Hypoparathyroidism was observed in all of the cases, being transient in three of them. In order to ensure fetal safety, the fetus was monitored preoperatively, in the immediate postoperative period, in an anesthetic recovery room, as well as twice a day until hospital discharge.Table 3. Case series. Description of surgical cases performed by the authors.Table 3. Number of patients5Age (years)25‒38Follow-upMinimum of 3 yearsSurgery15‒25 weeks (2^nd^ trimester)ReasonGrowing nodules2Lymph node metastasis3Type of SurgeryTotal thyroidectomy with lateral level VI cervical dissection2Total thyroidectomy with level VI cervical dissection1Total thyroidectomy without lymph node dissection2DeliveryCesarean section without intercurrencesObstetric examinationsNormal, pre- and post-surgical interventionAnesthesiaIntravenous (propofol + remifentanil)lodine therapyStarting 3-months after deliveryEvolutionWithout intercurrencesFig. 3Surgical indication of the series of cases in which the decision was, together with the clinical team, to address cancer during the second semester of pregnancy.Fig. 3. Fig. 4Surgical procedures performed by the authors in their series of cases divided according to the type of cervical dissection performed.Fig. 4
The length of hospital staying of the patients ranged from 2 to 4 days, and there were no postoperative complications.
Discussion
During prenatal care, it is customary to perform thyroid investigation by dosing TSH and free T4 levels, and it is important to analyze them carefully, since normal values are different in pregnancy.13, 14 If there are changes in these tests or a nodule is found on physical examination, further investigation by Ultrasound (US) and Fine Needle Aspiration Puncture (FNAP) should be conducted.13 However, we believe that thyroid nodule investigation should be performed in the pre-gestational period when possible. During the gestational period, the use of scintigraphy with radioactive iodine should be excluded, given the risks for fetal development.11, 13 Surgical resection is the usual conduct in confirmed cases of papillary thyroid carcinoma; however, the most appropriate time to perform surgery is controversial.1, 6
Surgery timing can be divided into pregnancy and postpartum. When approached during pregnancy, the optimal indication for surgery is the second trimester, since there is a teratogenic risk in the first trimester and a risk of early delivery in the third trimester.6, 15 The decision to operate during pregnancy is associated with the effects of human Chorionic Gonadotropin (hCG) on nodule growth due to reactivity of hCG with the TSH receptor.14, 16 More recent studies have also indicated that most of thyroid cancers in pregnancy present Estrogen Receptors alpha (ER-α), and their growth is therefore stimulated by high estrogen levels.17
More recent studies and reviews have shown that there is no difference in mortality and complications, whether maternal or fetal, between operating in the second trimester or after delivery.18 Nevertheless, some studies insist on the need to always perform surgery after delivery.1, 6, 8, 10
Many studies have reported the option to operate during pregnancy due to the anxiety caused by cases of more aggressive tumors,2, 8, 12, 13^,^19 as it occurred in the cases herein reported. Aggressive, or locally advanced histology, cervical metastases, compressive symptoms, and rapid nodule growth13, 14, 15, 18, 20 are the main aggressiveness criteria adopted to indicate surgery in the second trimester, as it occurred in the case of the present study, showing excellent results. However, other authors have used tumor size criteria, ranging from 1.0 to 1.5 cm, as suggestive of greater aggressiveness and surgical indication of patients in the second trimester of pregnancy.9, 21, 22
Another group of authors has always choosen to indicate surgery in the second trimester.3, 4, 9, 11 Such decision aims to reduce maternal anxiety23 and promote better maternal care and breastfeeding after delivery.9, 20 In any case, it should be considered that surgical intervention in the second trimester of pregnancy has higher costs (approximately USD 300 extra) in addition to a one-day increase in length of hospital stay.10
When a choice is made for surgical intervention in the second trimester of pregnancy, there is consensus that some extra care should be taken. Choosing a high-volume surgeon, for example, means a better prognosis.3, 4, 9, 11 Anesthesia should also be considered, and some groups have suggested the use of local anesthesia with cervical plexus block associated with the use of benzodiazepines and short-term opiates.7, 19 In our experience, the use of intravenous anesthesia with propofol and remifentanil did not present maternal or fetal complications in any of the cases.
Conclusion
There is no consensus on the correct time to perform thyroidectomy in pregnant patients with thyroid cancer. Although the review does not bring innovations, it provided collection of clearer data for the definition of conducts.
Operating the most severe cases in the second trimester is an option, as shown in our case series and described in the literature. We understand that more severe cases are those that present lymph node metastasis or effective nodule growth in the first weeks of pregnancy. In less severe cases, it is safer to perform thyroidectomy after delivery, and the risks to the patient and the fetus, patient anxiety, and costs of hospital stay should also be considered.
Financial support
None.
Declaration of competing interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Uruno T.Shibuya H.Kitagawa W.Nagahama M.Sugino K.Ito K.Optimal timing of surgery for differentiated thyroid cancer in pregnant women World J Surg 3820147047082424842910.1007/s 00268-013-2334-9 · doi ↗ · pubmed ↗
- 2Mazzaferri E.L.Approach to the pregnant patient with thyroid cancer J Clin Endocrinol Metab 9620112652722129699010.1210/jc.2010-1624 · doi ↗ · pubmed ↗
- 3Yasmeen S.Cress R.Romano P.S.Thyroid cancer in pregnancy Int J Gynaecol Obstet 91200515201608506110.1016/j.ijgo.2005.06.022 · doi ↗ · pubmed ↗
- 4Boucek J.de Haan J.Halaska M.J.Maternal and obstetrical outcome in 35 cases of well-differentiated thyroid carcinoma during pregnancy Laryngoscope 1282018149315002898843410.1002/lary.26936 · doi ↗ · pubmed ↗
- 5Andersen S.L.Olsen J.Laurberg P.Maternal thyroid disease in the Danish National Birth Cohort: prevalence and risk factors Eur J Endocrinol 17420162032122658248410.1530/EJE-15-0816 · doi ↗ · pubmed ↗
- 6Nam K.-H.Yoon J.H.Chang H.-S.Park C.S.Optimal timing of surgery in well- differentiated thyroid carcinoma detected during pregnancy J Surg Oncol 9120051992031611877510.1002/jso.20327 · doi ↗ · pubmed ↗
- 7Modesti C.Aceto P.Masini L.Lombardi C.P.Bellantone R.Sollazzi L.Approach to thyroid carcinoma in pregnancy Updates Surg 6920172612652863924010.1007/s 13304-017-0476-2 · doi ↗ · pubmed ↗
- 8Moosa M.Mazzaferri E.L.Outcome of differentiated thyroid cancer diagnosed in pregnant women J Clin Endocrinol Metab 82199728622866928471110.1210/jcem.82.9.4247 · doi ↗ · pubmed ↗