Increased implant thickness in mechanically aligned off‐the‐shelf total knee replacement compared to bone resection
Filippo Calanna, Riccardo Compagnoni, Luca Tanel, Alessandra Menon, Alessio Maione, Carlo Minoli, Paolo Ferrua, Pietro Simone Randelli

TL;DR
This study finds that in knee replacement surgery, implant thickness is generally greater than bone resection, with notable differences between knee compartments.
Contribution
The study quantifies bone-implant mismatch in mechanically aligned knee replacements and identifies compartment-specific discrepancies.
Findings
Implant thickness was 14.2% greater than bone resection overall.
Medial tibio-femoral mismatch was significantly greater than lateral (p < 0.001).
Patello-femoral implant thickness was less than bone resection by 16.0%.
Abstract
Total knee arthroplasty (TKA) with mechanical alignment (MA) aims to align the leg neutrally, optimising stability and load distribution. To achieve this, bone cuts are performed, modifying the constitutional alignment of the knee and determining a mismatch between the implant thickness and the bone resection across the various compartments of the knee (bone–implant mismatch). This study aims to quantify the bone–implant mismatch in TKA with MA using an off‐the‐shelf implant and investigate how this ratio is influenced by the preoperative coronal knee alignment phenotype. Data from 100 patients who underwent primary off‐the‐shelf TKA with MA with a medial pivot design implant from January 2021 to September 2023 were analysed. Preoperative alignment phenotype was determined via long‐leg weightbearing radiographs. During surgery, bone resections were measured with a caliper for each…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
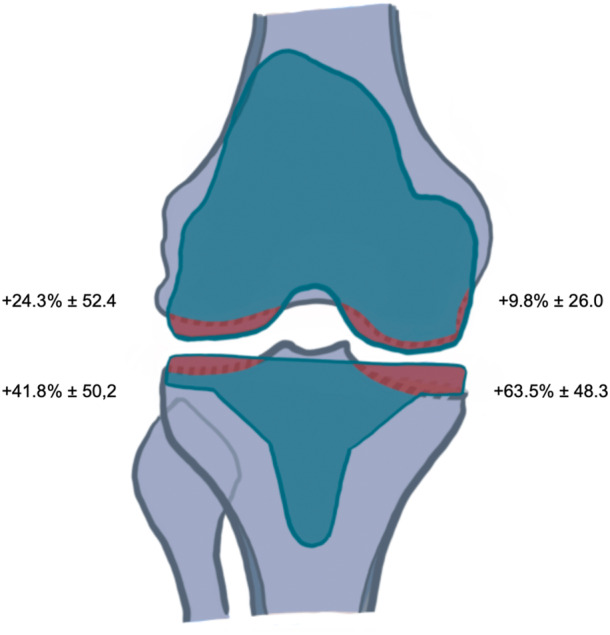 Figure 1
Figure 1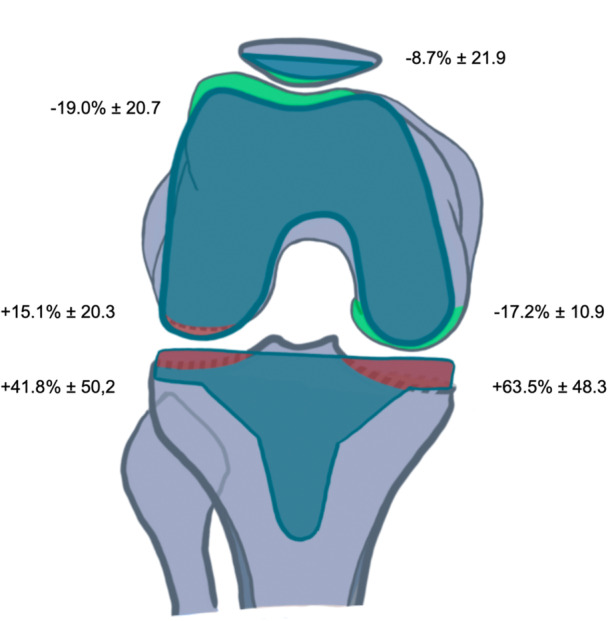 Figure 2
Figure 2| Varus HKA ≤ 177° ( | Neutral 177° < HKA > 183° ( | Valgus HKA ≥ 183° ( | Total ( |
| |
|---|---|---|---|---|---|
| %IMP medial tibia | 64.0 ± 43.6 | 71.8 ± 57.4 | 55.2 ± 49.4 | 63.5 ± 48.3 | 0.581 |
| 62.3 [37.6, 89.8] | 59.5 [27.3, 89.8] | 52.3 [23.1, 83.6] | 59.5 [27.3, 89.8] | ||
| %IMP lateral tibia | 38.0 ± 45.8 | 35.1 ± 38.8 | 55.1 ± 65.3 | 41.8 ± 50.2 | 0.471 |
| 20.9 [−2.2, 63.7] | 20.9 [17.7, 48.7] | 37.6 [11.1, 59.5] | 20.9 [7.5, 59.5] | ||
| %IMP medial posterior femur | −17.7 ± 10.8 | −18.8 ± 10.7 | −14.6 ± 11.4 | −17.2 ± 10.9 | 0.573 |
| −18.5 [−24.6, −11.3] | −18.5 [−24.6, −11.3] | −11.3 [−24.6, −11.3] | −18.5 [−24.6, −11.3] | ||
| %IMP lateral posterior femur | 12.1 ± 18.1 | 14.7 ± 19.8 | 21.0 ± 24.1 | 15.1 ± 20.3 | 0.437 |
| 7.9 [−2.6, 20.9] | 20.9 [−2.6, 20.9] | 20.9 [11.1, 20.9] | 20.9 [−2.6, 20.9] | ||
| %IMP medial distal femur | 10.7 ± 22.5 | −2.4 ± 20.5 | 19.0 ± 32.8 | 9.8 ± 26.0 |
|
| 8.8 [−2.9, 20.1] | −7.6 [−20.1, 8.8] | 8.8 [8.8, 23.8] | 8.8 [−5.3, 23.8] | ||
| %IMP lateral distal femur | 15.1 ± 41.3 | 25.6 ± 45.2 | 40.7 ± 72.4 | 24.3 ± 52.4 | 0.444 |
| 3.0 [−2.9, 23.8] | 16.3 [5.9, 43.5] | 3.0 [−12.4, 70.8] | 8.8 [−5.3, 43.5] | ||
| %IMP trochlea | −19.4 ± 17.9 | −19.9 ± 16.8 | −17.5 ± 28.5 | −19.0 ± 20.7 | 0.999 |
| −20.3 [−31.2, −5.1] | −20.3 [−31.2, −5.1] | −20.3 [−37.5, −5.1] | −20.3 [−31.2, −5.1] | ||
| %IMP patella | −16.7 ± 8.0 | −5.4 ± 18.5 | −1.4 ± 30.7 | −8.7 ± 21.9 | 0.282 |
| −13.7 [−17.5, −13.7] | −13.7 [−13.7, −13.7] | −13.7 [−13.7, −3.3] | −13.7 [−13.7, −13.7] | ||
| %IMP femoro‐patellar joint | −17.2 ± 16.7 | −17.1 ± 17.5 | −12.9 ± 24.3 | −16.0 ± 19.0 | 0.723 |
| −20.3 [−31.2, −5.1] | −16.3 [−23.9, −5.1] | −10.6 [−28.5, −6.5] | −16.3 [−31.2, −5.1] | ||
| %IMP total without femoro‐patellar joint | 18.2 ± 15.0 | 17.4 ± 11.3 | 22.3 ± 12.0 | 19.1 ± 13.4 | 0.496 |
| 13.0 [11.2, 23.5] | 17.9 [9.0, 24.5] | 21.6 [8.9, 31.4] | 14.4 [9.6, 29.7] | ||
| %IMP total | 13.5 ± 12.8 | 13.2 ± 10.1 | 16.3 ± 11.0 | 14.2 ± 11.7 | 0.422 |
| 10.0 [7.1, 15.5] | 11.6 [7.1, 21.7] | 19.5 [5.3, 23.7] | 11.6 [6.9, 21.7] |
| Comparison | Medial | Lateral |
|
|---|---|---|---|
| IMP% tibia | 63.5 ± 48.3 | 41.8 ± 50.2 |
|
| 59.5 [27.3, 89.8] | 20.9 [7.5, 59.5] | ||
| IMP% posterior femur | −17.2 ± 10.9 | 15.1 ± 20.3 |
|
| −18.5 [−24.6, −11.3] | 20.9 [−2.6, 20.9] | ||
| IMP% distal femur | 9.8 ± 26.0 | 24.3 ± 52.4 |
|
| 8.8 [−5.3, 23.8] | 8.8 [−5.3, 43.5] |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Orthopaedic implants and arthroplasty · Knee injuries and reconstruction techniques
INTRODUCTION
The primary goal of total knee arthroplasty (TKA) with mechanical alignment (MA) is to restore a neutral alignment with the prothesis perpendicular to the mechanical leg axis, aiming to improve stability, load distribution and patient outcomes at long term [5, 6, 14]. To achieve this, bone resections are performed, modifying the constitutional alignment of the knee and altering its joint line obliquity (JLO) [7, 21, 25, 29]. This process determines a mismatch between the component thickness and the bone resection across the various compartments of the knee (bone–implant mismatch) [26, 27]. Various factors, such as preoperative coronal knee alignment phenotype, knee laxity pattern (especially in case of gap balancing technique) and cartilage/bone wear determine the thickness of bone cuts, thus influencing bone–implant mismatch. Even the implant design seems to play a role: a recent meta‐analysis showed a higher bone–implant mismatch when using off‐the‐shelf (OTS) implants [1, 2], while custom TKA based on computed tomography (CT) reconstructions showed the potential to reduce this issue [3, 4].
Many studies have examined alignment phenotype changes from preoperative to postoperative in TKA with MA [7, 21, 25, 29] and how this theoretically determines a bone–implant mismatch [26, 27], however, none of these studies have specifically measured quantitatively the bone–implant mismatch in the different knee compartments.
This study aims to quantify the bone–implant mismatch (expressed as the percentage of extra implant thickness relative to the bone resection) in TKA with MA using an OTS implant and analyze how this is influenced by the preoperative coronal knee alignment phenotype.
The main hypothesis of the study was that the overall implant thickness, considering all the compartments of the knee, exceeds the thickness of the bone resection.
The second hypothesis was that there is bone–implant mismatch in each compartment of the knee with a significative difference medially compared to laterally in the tibio‐femoral compartment and that this differs significantly depending on the preoperative knee alignment phenotype.
METHODS
The study was designed based on the criteria of the Declaration of Helsinki and approved by the Institutional review board (IRB No. CTS‐P‐2024‐018‐FC).
An analysis of collected data was conducted. All patients undergoing primary TKA with MA with a medial pivot implant design (Evolution® Medial‐Pivot ‐ MicroPort, Arlington, TN) between January 2021 and September 2023 were considered for this study. All the operations were performed by a single senior knee surgeon. The following inclusion criteria were adopted: primary or post‐traumatic end‐stage tricompartmental knee osteoarthritis, co‐morbidities that do not contraindicate knee replacement, a Body Mass Index (BMI) <40 kg/m^2^.
Patients were excluded in case of inflammatory osteoarthritis, ligamentous insufficiency of the knee (JLCA > 5°), patients with active infections or altered skin conditions, patients with altered neurological conditions or neurological diseases, preoperative HKA < 160° or >200° and extra‐articular deformities suitable for knee osteotomies, revision surgery and in case of mayor ligamentous release.
Radiographic measurements
For each patient preoperative long‐leg anteroposterior weightbearing radiograph was obtained and the HKA angle calculated. Varus knee alignment was defined as an HKA angle of 177° or less, valgus knee alignment was defined as an HKA angle of 183° or more and a neutral knee alignment was defined as an HKA angle between 177° and 183° [10, 11].
Bone resection measurements
The thickness of the bone cuts in the femur, tibia and patella in each compartment of the knee was measured with a caliper during the operation. The total thickness of the bone resection was then calculated by adding the thickness of the blade used for the cuts (1.27 mm).
Surgical technique
In all procedures, MA was aimed. A medial parapatellar approach was used in all surgeries, performed by the same senior surgeon. The procedure begins by assessing the extension gap, followed by the flexion gap. We start with the distal femoral cut to open up the extension space, which facilitates subsequent steps of the procedure. The extension and flexion gaps were prepared utilising manual instrumentations and spacer blocks. A delicate partial subperiosteal release of the deep MCL bundle was performed to ensure better visibility of the joint and to prevent iatrogenic traumatic ruptures during the procedure. Such release did not alter the joint stability in any way during intra‐operative dynamic tests. No other releases were necessary or carried out. Patellar resurfacing was performed only in cases of severe patellofemoral arthritis with lateralized patella, following the selective resurfacing technique (i.e., bone‐on‐bone, especially if the patellofemoral joint surface was irregular, considering that this is a PS implant) [9].
The peri‐operative approach was standardised for all patients, including spinal anaesthesia and regional analgesic block, prophylactic antibiotics (Cefazolin 2 g pre‐operation, in the absence of allergies to this class of antibiotics Vancomycin 15 mg/kg was used as an alternative), and standard dose of ev. Tranexamic Acid (1 g) to reduce post‐operative blood loss, unless contraindicated. The surgical protocol adhered to established guidelines, including the use of a pneumatic tourniquet, meticulous haemostasis, and capsule closure followed by intra‐articular injection of 1 g of tranexamic acid. Tourniquet time (from inflation to release) and total surgical time (from incision to skin closure) were recorded.
Bone resection‐implant thickness mismatch
The bone resection‐implant thickness mismatch (bone–implant mismatch) was expressed as the percentage of extra implant thickness relative to the bone resection.
For the tibial implant thickness, we considered the tibial component + polyethylene insert and for the femoral implant thickness we considered the femoral component.
It was calculated as follows: (implant thickness − bone resection)/bone resection × 100. The following values were obtained:
- –percentage of extra implant thickness in the tibia: medially and laterally;
- –percentage of extra implant thickness in the distal femur: medially and laterally;
- –percentage of extra implant thickness in the posterior femur: medially and laterally;
- –percentage of extra implant thickness in the femoro‐patellar joint: trochlea and patella.
Statistical analysis
Statistical analyses were performed using R statistical software (Version 4.2.3; R Foundation for Statistical Computing) and GraphPad Prism (Version 6.0; GraphPad Software Inc). The Shapiro–Wilk normality test was used to evaluate the normal distribution of the sample. Continuous variables were presented as mean ± standard deviation and median [first quartile‐third quartile]. Categorical variables were expressed in numbers of cases and frequencies; their differences were tested using the chi‐square test or Fisher's exact test.
The between‐group differences for continuous variables were evaluated with the unpaired Student t‐test or Mann–Whitney test, according to the characteristics of the data distribution. The within‐group differences from baseline to post‐operative time points for continuous variables were evaluated with the Paired t‐test or Wilcoxon matched‐pairs signed rank test. according to the characteristics of the data distribution. For all analyses. the significance level was set at p‐value lower than 0.05.
In line with the recommendations by Hoenig and Heisey [12], we interpreted our results based on effect estimates and confidence intervals rather than relying on post hoc power calculations.
RESULTS
The results are reported in Table 1 and Table 2.
Among the 100 patients included in the study: 50 had a varus alignment (HKA ≤ 177°), 24 had a neutral alignment (177° < HKA < 183°) and 26 a valgus one (HKA ≥ 183°). The overall implant thickness was 14.2% greater than the bone resection.
In the tibia, the implant thickness exceeded the bone resection by 63.5% ± 48.3 medially and by 41.8% ± 50.2 laterally, showing a significant statistical difference between medial and lateral (p = 0.0014). In the posterior femur, the implant thickness was 17.2% ± 10.9 less than the bone resection medially and 15.1% ± 20.3 more laterally (p < 0.0001). In the distal femur, the implant thickness exceeded the bone resection medially by 9.8% ± 26.0 and laterally by 24.3% ± 52.4 (p = 0.016). The implant thickness was 19.0% ± 20.7 less than the bone resection in the trochlea and 8.7% ± 21.9 less in the patella, resulting in 16.0% ± 19.0 less implant thickness in the overall femoro‐patellar compartment than the bone resection (Table 2). Figures 1 and 2 show the bone–implant mismatch in the various knee compartments.
Bone implant mismatch in the tibia and in the distal femur. In red is represented a positive mismatch (more implant thickness) and in green a negative mismatch (more bone resection).
Bone implant mismatch in the tibia, posterior femur and in the patello‐femoral compartment. In red is represented a positive mismatch (more implant thickness) and in green a negative mismatch (more bone resection).
The statical analysis did not show any significant statistical difference in bone–implant mismatch between the three alignment phenotypes, except in the medial distal femur, where the implant thickness was 2.4% ± 20.5 less than the bone resection in neutral knees while in valgus knees was 19.0% ± 32.8 more (p < 0.028) (Table 1).
DISCUSSION
The main finding of this study is that the overall implant thickness, considering all compartments, is 14.2% greater than the bone resection, thus confirming our first hypothesis. Secondarily is also confirmed as there is bone–implant mismatch in each compartment of the knee with a significant difference medially compared to laterally in the tibio‐femoral joint. Finally, the consideration that the bone–implant mismatch in each compartment of the knee may differ significantly depending on the preoperative knee alignment phenotype, is refused, except considering the medial distal femur.
To the best of the author's knowledge, this is the first study to quantify and analyze the bone–implant mismatch in an OTS TKA with MA and to correlate these findings with the preoperative coronal knee alignment phenotype. As shown in the results section, there is a significant difference in bone–implant mismatch between the medial and lateral compartments in the distal femur, in the posterior femur and in the tibia. Specifically, the implant thickness exceeds the bone resection by 63.5% ± 48.3 in the medial tibia and by 41.8% ± 50.2 in the lateral tibia (p < 0.0001). In contrast, the femur showed an opposite pattern, with only 9.8% ± 26.0 extra implant thickness in the distal medial femur and 24.3% ± 52.4 extra implant thickness in the distal lateral femur (p < 0.0001). This distribution leads probably to an increase in both the medial proximal tibial angle (MPTA) and the lateral distal femoral angle (LDFA). Consequently, this may contribute to a modification of the JLO, which would tend to increase, shifting towards a neutral or proximal apex JLO phenotype, according to CPAK classification [19]. This pattern in JLO modification after TKA with MA is confirmed in literature. In their study Sappey‐Merinier et al. [25] showed that when performing TKA with MA, most of the patients had an increase in JLO, in their study they reported that preoperatively 63.5% of the patients had an apex distal JLO phenotype, 35.4% a neutral one and 1.1% an apex proximal phenotype; postoperatively only 8.5% still had an apex distal JLO while the majority, 81.9% had a neutral JLO and just a few (9.6%) an apex proximal. Cordan et al. [7] in their study also found a significant increased postop JLO in patients undergoing TKA with MA, as our study reported. Furthermore, Hirschmann et al. [26, 27] in their studies simulating bone resections using a model, demonstrated that both in varus and neutral knees phenotypes, MA tends to determine a proximalization of the joint line (JL) medially and a distalization laterally: this is in line with our results, confirming a pattern of increasing JLO (towards an apex proximal phenotype) after TKA with MA. It is also interesting to note that this pattern does not depend on the preoperative coronal alignment phenotype (varus, valgus and neutral) since, as shown in Table 1, there are no significant differences in bone–implant mismatch between the various alignments, except for a significant difference at the medial distal femur. The implant thickness in the medial distal femur was 2.4% ± 20.5 less than the bone resection in neutral knees while in valgus knees was 19.0% ± 32.8 more (p < 0.028), this means that in valgus knees there is an under‐resection of the distal medial femoral condyle compared to neutral ones. This may be attributed to the fact that valgus alignment often originates from femoral altered anatomy, typically characterised by metaphyseal deformity [31].
Considering the bone–implant mismatch in the posterior femur, the implant thickness is 17.2% ± 10.9 less than the bone resection on the medial side and 15.1% ± 20.3 more on the lateral side. According to the MA principles described by Insall [15], to achieve optimal gap balance in flexion, femoral posterior bone cuts are made in slight external rotation (using various reference parameters, such as the transepicondylar axis TEA, the posterior condylar axis PCA, or the anteroposterior AP axis). This leads to over‐resection of the medial posterior condyle and under‐resection of the lateral posterior condyle in order to achieve a balanced rectangular flexion gap. This is in accordance with our results, as 17.2% less posteromedial implant thickness and a 15.1% more posterolateral implant thickness determine a slight external rotation of the prosthetic component. Another interesting point is that in valgus knees this extra‐rotation is greater with 21.0% ± 24.1 more implant thickness (vs. 14.7% ± 19.8 in neutral knees and 12.1% ± 18.1 in varus knees) than bone resection in the lateral posterior femoral condyle. However, there was no statistically significant difference between the 3 values, probably due to a high standard deviation. The need of a greater femoral component external rotation in valgus knees to compensate the postero‐lateral cartilage worn or the lateral condyle hypoplasia, has been widely described in numerous studies in literature [18, 23].
Regarding the patellofemoral joint, our results clearly showed an important bone–implant mismatch in this compartment. The implant thickness is 19.0% ± 20.7 less than the bone resection in the trochlea and 8.7% ± 21.9 less in the patella, resulting in 16.0% ± 19.0 less implant thickness in the femoro‐patellar compartment than the bone resection. It is important to note that the patella was resurfaced in only 46 cases. This significant bone–implant mismatch is in our opinion due to different factors. First, most commercially available prostheses exhibit a degree of dysplasia in the trochlea. As reported by Saffarini et al. [24] in recent TKA designs trochlear compartments exceed radiologic signs of trochlear dysplasia by 2°–5°. Specifically, their study demonstrates that the sulcus angles remain 3°–6° greater (shallower) in prosthetic trochlear compartments. Secondly recent studies show that TKA performed with MA and using an off the shelf implant design does not restore the native trochlear groove [17, 20]. Reducing the implant thickness in PF compartment might compensate the dysplasia of the trochlea, lowering the risk of maltracking, instability, anterior pain and ROM limitation [16]. It should be noted that by resecting more bone in the trochlea compared to the implant thickness there is a risk of femoral notching [28, 30], which never occurred in our cohort of patients.
In none of the evaluated parameters (except at the distal femur) there was a significant difference in bone–implant mismatch according to knee alignment. This result suggests that, in achieving MA in TKA, the type of preoperative coronal alignment phenotype (varus, valgus or neutral) does not seem to determine our bone cuts. Instead, JLO seems to be a likely more determinant factor. Since JLO tends to decrease postoperatively moving toward a neutral value, probably the thickness of the bone cuts, at least in the coronal plane will be determined by its preoperative value.
The fact that in our study the overall implant thickness is 14.2% greater than the bone resection—and reaches 19.1% when excluding the patello‐femoral joint— likely represents in part a compensation for cartilage loss due to wear in osteoarthritic knees and meniscal removal during operation. This extra volume helps to restore the bone, cartilage and soft tissue loss. However, some of this extra implant thickness may be attributed to the type of alignment used. Kinematic alignment [13, 22] aims to preserve or restore the constitutional alignment, by aligning implants to the native condylar and tibial joint lines, and by matching component thickness of the femoral condyles and tibia to that of bone resection, plus a small additional amount to account for cartilage that has worn. This would lead probably to a smaller overall bone–implant mismatch and a smaller difference between medial and lateral bone–implant mismatch, minimally altering the natural knee spaces. However, these altered joint spaces are probably not due only to the alignment technique but also to the use of OTS prostheses. Such standardised implants may not perfectly conform to the patient's unique anatomy [1, 2]. By contrast, a custom‐made prosthesis would likely provide a more tailored fit to the patient's bone structure [3, 4]. It is likely that a custom‐made prosthesis combined with a personalised alignment [8] approach could offer the best solution to achieve optimal balance in joint spaces.
LIMITATIONS
Our study has several limitations. First, it lacks postoperative long‐leg anteroposterior weightbearing radiographs, which would allow for an assessment of postoperative HKA. Additionally, parameters such as aHKA, MPTA and LDFA were not calculated. It does not account for cartilage wear, soft tissue thickness (including meniscal structures), or the ligamentous envelope, factors which could influence compartmental balancing together with the PE insert dimension. Moreover effect size measures were not reported.
CONCLUSIONS
In mechanically aligned OTS TKA, implant thickness exceeds bone resection by an average of 14.2%, with a consistent bone–implant mismatch observed in all tibiofemoral compartments—significantly greater medially than laterally. Conversely, in the patellofemoral joint, bone resection surpasses implant thickness. Preoperative coronal alignment phenotype does not significantly influence this mismatch. These findings highlight a systematic discrepancy between bone resections and implant geometry, suggesting potential benefits from adjusted surgical techniques or implant design modifications to improve anatomical congruence and joint kinematics.
AUTHOR CONTRIBUTIONS
All authors have given final approval of the submitted manuscript and their agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have made substantial contributions to the design of the work and manuscript writing. All authors were involved in drafting the work or revising it critically for important intellectual content.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
The study was approved by the Institutional review board (IRB N° CTS‐P‐2024‐018‐FC). All patients gave valid consent to participate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Beckers L , Müller JH , Daxhelet J , Ratano S , Saffarini M , Aït‐Si‐Selmi T , et al. Considerable inter‐individual variability of tibial geometric ratios renders bone–implant mismatch unavoidable using off‐the‐shelf total knee arthroplasty: a systematic review and meta‐analysis. Knee Surg Sports Traumatol Arthrosc. 2023;31(4):1284–1298.34075491 10.1007/s 00167-021-06623-7 · doi ↗ · pubmed ↗
- 2Beckers L , Müller JH , Daxhelet J , Saffarini M , Aït‐Si‐Selmi T , Bonnin MP . Sexual dimorphism and racial diversity render bone–implant mismatch inevitable after off‐the‐shelf total knee arthroplasty: a systematic review and meta‐analysis. Knee Surg Sports Traumatol Arthrosc. 2022;30(3):809–821.33512544 10.1007/s 00167-021-06447-5 · doi ↗ · pubmed ↗
- 3Bonnin MP , Beckers L , Leon A , Chauveau J , Müller JH , Tibesku CO , et al. Correction to: Custom total knee arthroplasty facilitates restoration of constitutional coronal alignment. Knee Surg Sports Traumatol Arthrosc. 2022;30(2):476.32860522 10.1007/s 00167-020-06238-4PMC 8866254 · doi ↗ · pubmed ↗
- 4Bonnin MP , Beckers L , Leon A , Chauveau J , Müller JH , Tibesku CO , et al. Custom total knee arthroplasty facilitates restoration of constitutional coronal alignment. Knee Surg Sports Traumatol Arthrosc. 2022;30(2):464–475.32681286 10.1007/s 00167-020-06153-8PMC 8866384 · doi ↗ · pubmed ↗
- 5Callahan CM . Patient outcomes following tricompartmental total knee Replacement. JAMA. 1994;271(17):1349.8158821 · pubmed ↗
- 6Carr AJ , Robertsson O , Graves S , Price AJ , Arden NK , Judge A , et al. Knee replacement. Lancet. 2012;379(9823):1331–1340.22398175 10.1016/S 0140-6736(11)60752-6 · doi ↗ · pubmed ↗
- 7Corban LE , van de Graaf VA , Chen DB , Wood JA , Diwan AD , Mac Dessi SJ . How often do we alter constitutional limb alignment, joint line obliquity, and Coronal Plane Alignment of the Knee (CPAK) phenotype when performing mechanically aligned TKA?: a large single‐institution retrospective radiological analysis. Bone Joint Open. 2024;5(2):109–116.38325412 10.1302/2633-1462.52.BJO-2023-0122 PMC 10849801 · doi ↗ · pubmed ↗
- 8Graichen H , Avram GM , Strauch M , Kaufmann V , Hirschmann MT . Tibia‐first, gap‐balanced patient‐specific alignment restores bony phenotypes and joint line obliquity in a great majority of varus and straight knees and normalises valgus and severe varus deformities. Knee Surg Sports Traumatol Arthrosc. 2024;32(5):1287–1297.38504509 10.1002/ksa.12145 · doi ↗ · pubmed ↗