The International TrifectaTM and EpicTM Valve‐in‐Valve Registry: Insights Into Clinical & Hemodynamic Outcomes
Matthias Raschpichler, Mohamed Abdel‐Wahab, Nick Curzen, Manuel Wilbring, Christoph Dubois, Kayan Lam, Gloria Faerber, Jana Nagel, Holger Thiele, Michael A. Borger

TL;DR
This study compares the outcomes of valve-in-valve TAVR in two types of failed aortic valves, finding that Trifecta valves have lower risks of complications and better patient outcomes.
Contribution
The study provides the first international comparison of clinical and hemodynamic outcomes for ViV-TAVR in Trifecta versus Epic valves.
Findings
ViV-TAVR into Trifecta valves showed a lower rate of the primary composite outcome (6.1% vs. 20%) compared to Epic valves.
Trifecta patients had a lower risk of patient-prosthesis mismatch compared to Epic patients.
Survival rates were similar between the two groups at a median follow-up of 365 days.
Abstract
Little is known about the clinical and hemodynamic outcome of valve‐in‐valve transcatheter aortic valve replacement (ViV‐TAVR) for failed Trifecta surgical aortic bioprotheses. We aimed to compare outcomes of valve‐in‐valve transcatheter aortic valve replacement (ViV‐TAVR into failed TrifectaTM vs. ViV‐TAVR into a standard aortic bioprosthetic valve with internally mounted leaflets (EpicTM, Abbott, Minneapolis, MN). Data of consecutive patients who underwent ViV‐TAVR into either failed TrifectaTM or EpicTM bioprostheses between October 2015 and June 2020 were retrospectively collected within the International Trifecta and Epic Valve‐in‐Valve Registry, and analyzed for a primary composite outcome of 30‐day mortality and/or coronary obstruction (CO), defined as: (1) CO resulting in myocardial infarction and/or cardiogenic shock, or (2) CO requiring emergent coronary intervention. A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
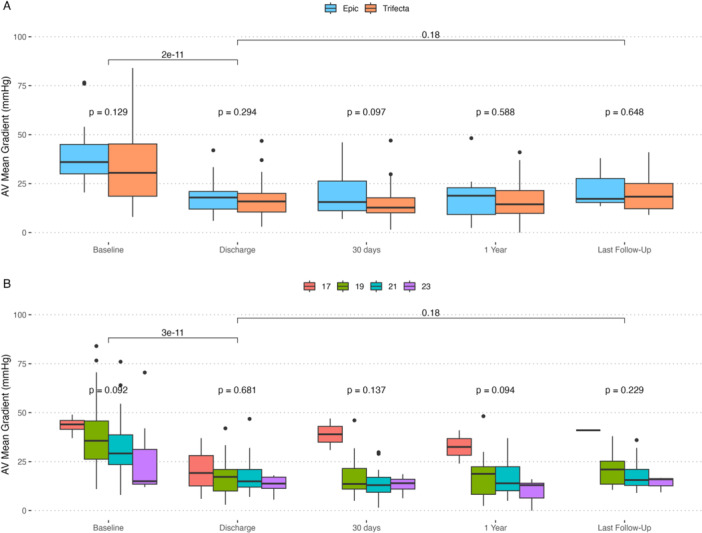 Figure 1
Figure 1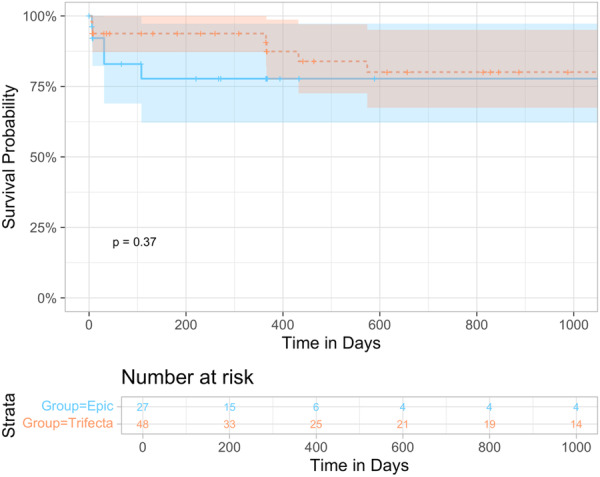 Figure 2
Figure 2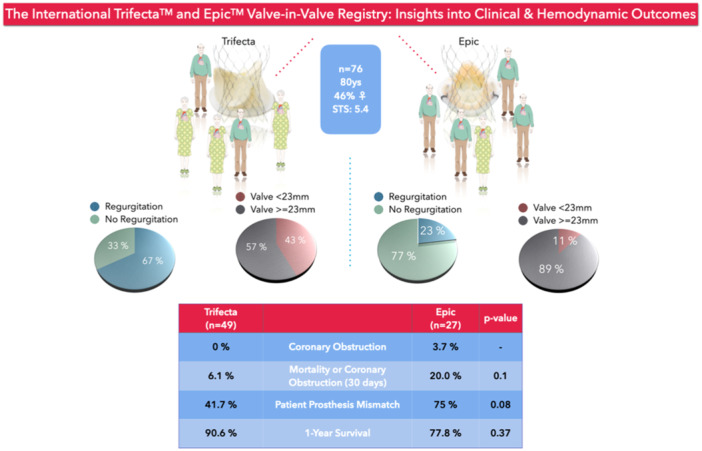 Central Figure 1
Central Figure 1| Epic ( | Trifecta ( |
| |
|---|---|---|---|
| Age (years) | 80.0 [78.0; 84.5] | 79.0 [75.0; 82.0] | 0.184 |
| Female | 4 (14.8%) | 31 (63.3%) | < 0.001 |
| BSA (m2) | 1.87 [1.78; 1.95] | 1.82 [1.71; 1.91] | 0.385 |
| STS PROM Score | 7.73 [4.12; 10.3] | 5.00 [4.02; 8.53] | 0.300 |
| NYHA > I | 25 (92.6%) | 46 (97.9%) | 0.550 |
| Prior Stroke | 2 (7.41%) | 3 (6.12%) | 1.000 |
| Prior MI | 4 (14.8%) | 1 (2.04%) | 0.051 |
| Arterial Hypertension | 23 (85.2%) | 45 (91.8%) | 0.444 |
| Insulin‐Dependent Diabetes Mellitus | 3 (11.1%) | 10 (20.4%) | 0.359 |
| Chronic Renal Failure | 9 (33.3%) | 18 (36.7%) | 0.963 |
| PCI Within 3 Months Prior | 2 (7.41%) | 6 (13.3%) | 0.701 |
| Prior CABG | 13 (48.1%) | 17 (34.7%) | 0.366 |
| Permanent Pacemaker | 5 (18.5%) | 13 (26.5%) | 0.614 |
| LVEF (%) | 55.5 [42.8; 65.0] | 57.6 [44.2; 62.2] | 0.794 |
| Aortic Stenosis > mild | 21 (100%) | 28 (68.3%) | 0.003 |
| EOA | 0.80 [0.55; 0.90] | 0.95 [0.62; 1.30] | 0.055 |
| AV Mean Pressure Gradient | 36.0 [30.0; 45.0] | 30.5 [18.6; 45.2] | 0.129 |
| AV Peak Pressure Gradient | 65.0 [51.2; 77.8] | 54.9 [32.5; 77.5] | 0.161 |
| Aortic Regurgitation > mild | 5 (22.7%) | 30 (66.7%) | 0.002 |
| Mode of Failure: Predominant AS | 17 (77.3%) | 15 (33.3%) | 0.002 |
| Mode of Failure: Predominant AR | 0 (0.00%) | 13 (31.7%) | 0.003 |
| Mode of Failure: Mixed | 3 (15.0%) | 12 (30.0%) | 0.343 |
| Epic ( | Trifecta ( |
| |
|---|---|---|---|
| Time between Interventions (years) | 5.39 [4.08; 10.4] | 6.55 [4.65; 7.74] | 0.978 |
| Surgical Valve Diameter < 23 mm | 3 (11.1%) | 21 (42.9%) | 0.010 |
| Annulus Maximal Diameter (mm) | 24.0 [22.2; 26.0] | 22.0 [20.0; 24.1] | 0.088 |
| Annulus Mean Area (mm2) | 383 [347; 415] | 344 [285; 380] | 0.046 |
| Left Coronary Artery Height (mm) | 10.0 [9.50; 12.0] | 8.00 [6.00; 11.0] | 0.113 |
| Right Coronary Artery Height (mm) | 13.0 [9.50; 16.5] | 10.0 [6.95; 14.0] | 0.071 |
| SoV Width (mm) | 33.0 [31.0; 36.5] | 32.0 [30.0; 35.0] | 0.291 |
| STJ Width (mm) | 29.8 [29.0; 32.0] | 28.0 [26.0; 30.4] | 0.250 |
| Predilatation | 12 (44.4%) | 11 (22.9%) | 0.093 |
| Any Coronary Protection Maneuver | 0 (0.00%) | 8 (29.6%) | 0.006 |
| Leaflet Laceration (BASILICA) | 0 (0.00%) | 4 (14.3%) | 0.117 |
| Self‐expandable ViV Prosthesis | 14 (51.9%) | 30 (61.2%) | 0.583 |
| ViV Size: | 0.074 | ||
| 20 | 1 (3.70%) | 0 (0.00%) | |
| 23 | 13 (48.1%) | 35 (71.4%) | |
| 26 | 12 (44.4%) | 11 (22.4%) | |
| 29 | 1 (3.70%) | 3 (6.12%) |
| Epic ( | Trifecta ( |
| |
|---|---|---|---|
|
| |||
| Mortality | 2 (8.00%) | 3 (6.1%) | 1.000 |
| Coronary Obstruction | 1 (3.70%) | 0 (0.00%) | ‐‐‐ |
| Stroke | 2 (7.41%) | 2 (4.08%) | 0.612 |
| Minor Vascular Complication | 5 (18.5%) | 7 (14.3%) | 0.745 |
| Early Safety | 18 (78.3%) | 38 (90.5%) | 0.260 |
| Mean AV Gradient [mm Hg] | 17.9 [12.0; 21.0] | 15.9 [10.5; 20.0] | 0.294 |
| Peak AV Gradient [mm Hg] | 25.5 [21.5; 34.5] | 26.1 [18.1; 34.5] | 0.488 |
| AV Residual Gradient (≥20 mmHg) | 10 (43.5%) | 11 (25.6%) | 0.226 |
| iEOA | 0.73 [0.60; 0.83] | 0.81 [0.74; 1.01] | 0.087 |
| Moderate or Severe PPM | 12 (75.0%) | 10 (41.7%) | 0.080 |
|
| |||
| Primary Outcome (Mortality or CO) | 5 (20.0%) | 3 (6.1%) | 0.116 |
| LVEF [%] | 57.0 [45.0; 65.0] | 59.0 [55.0; 62.0] | 0.530 |
| Mean AV Gradient [mm Hg] | 15.6 [11.2; 26.3] | 12.8 [10.1; 17.8] | 0.097 |
| Peak AV Gradient [mm Hg] | 32.0 [22.9; 41.8] | 22.4 [15.8; 29.9] | 0.057 |
- —Financial support was provided by the Abbott Structural Heart.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
Introduction
1
Valve‐in‐Valve transcatheter aortic valve replacement (ViV‐TAVR) has become the treatment of choice for many patients presenting with deteriorated surgical aortic bioprostheses at higher surgical risk [1, 2]. Most observational studies have demonstrated superior short‐term clinical outcome of ViV‐TAVR compared to redo surgical aortic valve replacement (rSAVR), while the benefits regarding long‐term outcome remain unclear [3, 4, 5, 6]. Downsides of ViV‐TAVR include inferior hemodynamic performance compared to rSAVR, increased risk of thrombogenicity of ViV‐TAVR prostheses, and greater difficulty to access coronary arteries postprocedure [7, 8, 9]. Although rare, periprocedural coronary obstruction (CO) is a feared, and often lethal, complication. Risk factors associated with CO following ViV‐TAVR include narrow sinotubular dimensions relative to the ViV‐TAVR prostheses and stentless surgical prostheses or those with externally mounted leaflets [10].
In patients at risk of CO, preventive measures such as coronary wiring, pre‐emptive stenting, or bioprosthesis leaflet laceration (e.g., the BASILICA procedure), can reduce both occurrence and consequences of CO [11, 12]. These techniques are particularly relevant for stented bioprostheses with externally mounted leaflets designed to provide the largest possible opening area, such as the Mitroflow (LivaNova, London, UK) or the Trifecta (Abbott, Minneapolis, MN) prostheses. The Trifecta valve is a tri‐leaflet supra‐annular bovine pericardial prosthesis with leaflets mounted on the outside of a polyester‐covered titanium stent to maximize valve opening [13]. The titanium stent cannot be fractured with a valvuloplasty balloon, but it is possible to deform the stent posts outwardly [14, 15]. Unfortunately, several reports have demonstrated limited durability compared to other stented prostheses [16, 17, 18, 19, 20]. Although many patients require re‐intervention when rSAVR is considered high risk, data on ViV‐TAVR for failed Trifecta prostheses remains limited. In comparison, the Epic Supra valve (Abbott, Minneapolis, USA) is a supra‐annular valve from the same manufacturer but designed with leaflets mounted internally. It therefore allows the comparison to a potentially problematic valve.
The current study compares the clinical and hemodynamic outcome of patients undergoing ViV‐TAVR for deteriorated Trifecta and Epic^T^ aortic bioprostheses from a multicenter European registry.
Methods
2
Data Availability Statement
2.1
Data and statistical analysis underlying this article can be shared upon reasonable request.
Study Population
2.2
We retrospectively collected baseline, procedural, hemodynamic, and clinical data of consecutive patients that underwent ViV‐TAVR for deteriorated Trifecta or Epic aortic bioprostheses at six European centers between October 2015 and June 2020 within The International Trifecta and Epic Valve‐in‐Valve Registry (NCT05389631). Exclusion criteria included (1) ViV‐TAVR of an aortic valve bioprosthesis other than the Trifecta or Epic valve, and (2) patients undergoing combined multiple transcatheter valve procedures in addition to ViV‐TAVR. This retrospective study was approved by the ethics committees of each participating center (Supporting Information S1: Table 1). Funding was provided by Abbott Structural Heart.
The Trifecta GT valve is a second‐generation valve that was introduced in 2016 and has additional features intended to make the valve easier to implant. The Epic Supra valve (Abbott, Minneapolis, USA) is a supra‐annular triple composite porcine valve with leaflets mounted internally onto a low profile FlexFit polyester‐covered polymer stent [21]. The stent frame can be fractured with a valvuloplasty balloon at 8 atmospheres [14].
Outcomes of Interest
2.3
The primary outcome of interest was a composite of 30‐day all‐cause mortality and/or clinically significant CO defined as: (1) CO resulting in myocardial infarction and/or cardiogenic shock, or (2) CO requiring emergent coronary intervention. Secondary outcomes of interest included selected Valve Academic Research Consortium (VARC)3‐based outcomes including cardiac structural complications and early safety [22]. All variables were collected locally. Median follow‐up was 365 days.
Statistical Analysis
2.4
Normality of data was tested using Shapiro‐Wilk test. Continuous variables of normal distribution were compared using student t‐test and are shown as mean ±standard deviation (SD). Continuous variables without normal distribution were compared using Wilcoxon rank‐sum or Kruskall‐Wallis test and are shown as median ± interquartile range (IQR). Categorical variables were compared using Chi^2^ and are shown as frequencies and percentages. Missing variables were tested both numerically and graphically for patterns of missingness and subsequently treated as missing at random. Using the difference of the surgical prosthesis as well as baseline and CT‐based parameters that differed at a level of p < 0.1 as independent variables, and the primary composite outcome as the dependent variable within uni‐variable binomial regression, we tested all variables with a p‐value of less than 0.1 as well as clinically relevant variables using the Wald‐test as well as Pseudo‐R^2^ measures as criteria within multivariable analysis. Midterm clinical outcome was analyzed using the Kaplan‐Meier curve and the log‐rank test. Statistical analysis was performed using base R functions (R version 4.2.1) within RStudio (version 1.4.1103), as well as the following R packages: tidyverse, compareGroups, ggthemes, ggsci, ggpubr, aod, pscl, janitor, reshape2, survival, and survminer. The manuscript was written using R Markdown and Knitr in adherence to principles of reproducible research.
Results
3
Study Population & Baseline Characteristics
3.1
Seventy‐six patients (median age 80 years, interquartile range [IQR] 75; 82]; 46.1% females) with a median Society of Thoracic Surgeons‐score of 5.4 [4; 9.8] were identified (Table 1). The 76 implanted surgical prostheses included Epic standard valve (N = 23), Epic Supra valve (N = 4), Trifecta valve (N = 47), and Trifecta GT valve (N = 2). Trifecta patients were more frequently female (63.3% vs. 14.8%, p < 0.001) and had lower rates of previous myocardial infarction (2.0% vs. 14.8%, p = 0.05). All Epic prostheses showed relevant stenosis (63.8% vs. 100% for Trifecta vs. Epic, respectively, p = 0.003), while approximately 2/3 of Trifecta valves had relevant prosthesis regurgitation (66.7% vs. 22.7%, p = 0.002), with greater valve effective orifice areas compared to Epic prostheses (0.95 vs. 0.80 cm^2^, p = 0.06). Small surgical valves (i.e., labeled valve diameter < 23 mm) were more frequent in the Trifecta group (42.9% vs. 11.1%, p = 0.01).
Computed Tomography Measures & Procedural Characteristics
3.2
Median time between surgery and ViV‐TAVR was 6.4 years (4.5; 8.0; Table 2). Selected CT‐based and procedural characteristics of the two ViV sizes predominantly utilized (i.e., 23 mm and 26 mm valve size) are shown in Supplemental Table 2. Access for ViV‐TAVR was transfemoral in all but one Trifecta case. Smaller aortic annulus and surgical prosthesis diameters were present in patients undergoing valve‐in‐Trifecta. Coronary protection was performed in eight Trifecta cases (29.6%; four leaflet laceration procedures; three protective wiring; one preventive stenting) versus 0 Epic cases (p = 0.006). Coronary obstruction occurred in one case following valve‐in‐Epic. The obstructed left main coronary artery was stented and the patient was discharged uneventfully. Supporting Information S1: Table 4 shows selected variables of cases of coronary protection or coronary obstruction.
Clinical and Hemodynamic Outcome
3.3
The primary composite outcome of all‐cause mortality or CO was observed in 8 cases, three times more frequently in patients undergoing valve‐in‐Epic (20.0% vs. 6.4%, p = 0.1, Table 3). Adverse clinical events included two cases of VARC3‐based cardiac structural or other/technical complications in Trifecta patients, and one Trifecta case of valve malpositioning, resulting in comparable rates of VARC3‐based early safety. Multivariable logistic regression including prosthesis type and STS‐score as independent variables revealed that prosthesis regurgitation was independently and inversely associated with the primary composite outcome (Supporting Information S1: Table 3).
Hemodynamic performance improved significantly following ViV‐TAVR and remained improved through last follow‐up (Figure 1; Supporting Information S1: Table 5). Although overall comparable between groups, valve‐in‐Trifecta resulted in lower mean and peak gradients at 30 days (12.8 vs. 15.6 mmHg and 22.4 vs. 32 mmHg; p = 0.1 and 0.06, respectively); larger aortic valve area at both discharge and 1 year postprocedure (1.9 vs. 1.3 cm^2^ and 1.7 vs. 1.1 cm^2^, respectively, p = 0.02); and lower rates of PPM and thus VARC3‐based nonstructural valve dysfunction (41.7% vs. 75.0%, p = 0.08; Supporting Information S1: Figure 1). Survival at a median of 365 days did not differ between groups (log‐rank p = 0.37; Figure 2).
Graphs depicting mean valve gradient by (A) prosthesis type (blue = Epic, orange = Trifecta, and (B) true internal diameter of the surgical prosthesis. Gradients improved significantly by discharge and improvements were maintained until follow up. [Color figure can be viewed at wileyonlinelibrary.com]
Curves depict Kaplan‐Meier time‐to‐event rates for all‐cause mortality by prosthesis type (blue = Epic, orange = Trifecta). [Color figure can be viewed at wileyonlinelibrary.com]
Discussion
4
The International Trifecta and Epic Valve‐in‐Valve Registry assessed the clinical and hemodynamic outcome of ViV‐TAVR, comparing surgical aortic bioprostheses with and without increased risk of CO based on the mounting of the leaflets. We found that: (1) ViV‐TAVR for deteriorated Trifecta‐valves was performed without major complications in more than 90% of the cases using measures to prevent CO, in 29.6% of the Trifecta patients; (2) hemodynamic outcome post‐Trifecta ViV‐TAVR is acceptable and appears to be comparable to other ViV‐cohorts; (3) midterm survival may be comparable to other failed prostheses treated in similar patient populations [2].
Although our cohort was comparable to most previous reports on ViV‐TAVR, some aspects are worth highlighting. First, the Trifecta patients represent a subgroup of individuals at increased risk for PPM post ViV‐TAVR due to small annular dimensions relative to body surface area (BSA). Approximately 2/3 of Trifecta patients were female, with annulus diameters unsuitable for prosthesis larger than 22 mm in diameter on average, while BSA did not differ between groups. At ViV‐TAVR, this did not result in lower baseline effective orifice areas (EOA) in Trifecta patients, likely due to the mode of failure which included prosthesis regurgitation in 2/3 of the cases. Nevertheless, small surgical valves (i.e., labeled valve diameter < 23 mm) were more frequent in the Trifecta group, accounting for 87.5% of all cases of small valves, of which in turn 83.3% were female. Conversely, 57.1% of all female patients received surgical prostheses smaller than 23 mm at the index SAVR procedure. Although the EOA and short‐term hemodynamic outcome may be superior in prostheses with externally compared to internally mounted leaflets, the titanium stent ring ultimately limits the size of the ViV‐TAVR prosthesis, since the Trifecta valve cannot be fractured [14, 15, 23]. This may result in PPM after ViV‐TAVR, which is known to be associated with worse long‐term clinical outcomes [24]. Reporting on the outcome of ViV‐TAVR for these prostheses, therefore, highlights the life‐time consequences of avoiding root enlargement techniques in small aortic roots at the initial SAVR procedure (Central Figure 1).
Figure illustrating the two groups undergoing ViV‐TAVR for failed Trifecta (left) and Epic (right column) valves. [Color figure can be viewed at wileyonlinelibrary.com]
Coronary obstruction is a rare, but often lethal, complication following ViV‐TAVR [10]. With a single case of CO in our series managed successfully with coronary stenting, our data confirm that CO is infrequent, even when including prostheses at higher risk of this complication. It should be noted, however, that preventive measures such as leaflet laceration or coronary wiring were utilized exclusively in Trifecta cases. We did not have access to the number of patients screened for a ViV‐TAVR and were therefore unable to assess how many patients with an indication for repeat intervention were indeed referred for intervention. Thus, the degree of selection bias cannot be evaluated, and it remains unclear whether our results can be generalized to other prostheses with externally mounted leaflets. Nevertheless, recent data on coronary protection and CO in 250 cases of aortic ViV‐TAVR including 28% with externally mounted leaflets demonstrated higher rates of CO or stent deployment compared to those with internally mounted leaflets, with no difference in mortality after 2 years [12]. Notably, coronary protection was performed in 79% of the cases with externally mounted leaflets (vs. 6% for other prostheses), indicating the importance of patient selection and pre‐procedure planning with a low threshold to utilize coronary protection [12, 25].
Finally, hemodynamic outcome in our data demonstrate that although valve‐in‐Trifecta may be technically challenging, it can also lead to better valve opening area compared to prostheses without externally mounted leaflets. At least moderate PPM was found more frequently following valve‐in‐Epic, resulting in 75% of patients meeting the VARC3‐based endpoint of stage‐1 nonstructural valve dysfunction [22]. This is an interesting finding, because neither choice of TAVR prosthesis (balloon‐ vs. self‐expandable) nor procedural characteristics such as pre‐ or post‐dilatation and bioprosthetic valve fracture differed between groups. In fact, the latter were used numerically less frequently in Trifecta patients. A possible explanation for this finding includes the differences in failure mode as well as pre‐existing PPM in the Epic group [9]. Compared to other surgical aortic bioprostheses, the deterioration of Trifecta prostheses includes an increased rate of cusp tear and subsequent prosthesis regurgitation [26, 27, 28, 29]. Although reduced EOA postprocedure did not translate into statistically worse hemodynamic performance in terms of mean or peak valve gradient in our study, valve‐in‐Epic resulted in mild prosthesis stenosis based on mean gradient and valve opening area, a finding that is in line with other reports on aortic ViV‐TAVR [9, 29, 30]. It is known that PPM is associated with impaired long‐term survival following valve replacement [24]. In our sample, more than half of the patients discharged with at least moderate PPM were not high‐risk based on the STS‐score. For these patients, elective rSAVR may be considered as it could lead to improved hemodynamics and therefore better long‐term clinical outcomes [3, 31, 32].
Limitations
4.1
The current study has several limitations. First, we focused on the Trifecta prostheses representing a valve design with externally mounted leaflets and our results are therefore limited to this particular heart valve. Second, sample size was limited which may explain why we could not detect statistical significance for the primary outcome of interest. Third, some hemodynamic measures were incomplete during follow‐up and hence should be interpreted with caution. Forth, relevant CT‐based measurements such as the valve‐to‐aorta or valve‐to‐coronary distances were available in three cases only and could therefore not be studied for this analysis. Finally, screening processes were not documented for patients presenting with Trifecta or Epic valve failure who were not referred for intervention, and our data therefore carries a risk of selection bias.
Conclusions
5
In comparison to a standard surgical aortic bioprosthesis without increased risk of CO based on mounting of leaflets, Trifecta aortic bioprostheses with an indication for repeat intervention can be treated safely using ViV‐TAVR in the majority of cases, when techniques to limit the risk of CO are appropriately utilized. One year mortality is acceptable post‐ViV TAVR, but a significant proportion of patients have post‐intervention PPM which may affect longer term outcomes.
Conflicts of Interest
Dr. Borger declares that his hospital receives speakers' honoraria and/or consulting fees on his behalf from Edwards Lifesciences, Medtronic, Abbott, and Artivion. Dr. Abdel‐Wahab declares that his hospital receives speaker's honoraria and/or consultancy fees on his behalf from Medtronic, Boston Scientific and Edwards Lifesciences. Prof Curzen declares receipt of grants from Boston Scientific, HeartFlow, Beckman Coulter, Haemonetics and honoraria from Abbott, Shockwave & Boston. Dr. Dubois declares that he is transcatheter heart valve proctor for Edwards Lifesciences.
Supporting information
Supporting information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. Dvir , J. Webb , S. Brecker , et al., “Transcatheter Aortic Valve Replacement for Degenerative Bioprosthetic Surgical Valves,” Circulation 126 (2012): 2335–2344.23052028 10.1161/CIRCULATIONAHA.112.104505 · doi ↗ · pubmed ↗
- 2J. G. Webb , D. J. Murdoch , M. C. Alu , et al., “3‐Year Outcomes After Valve‐in‐Valve Transcatheter Aortic Valve Replacement for Degenerated Bioprostheses,” Journal of the American College of Cardiology 73 (2019): 2647–2655.31146808 10.1016/j.jacc.2019.03.483 · doi ↗ · pubmed ↗
- 3P. Deharo , A. Bisson , J. Herbert , et al., “Transcatheter Valve‐in‐Valve Aortic Valve Replacement as an Alternative to Surgical Re‐Replacement,” Journal of the American College of Cardiology 76 (2020): 489–499.32731926 10.1016/j.jacc.2020.06.010 · doi ↗ · pubmed ↗
- 4M. Majmundar , R. Doshi , A. Kumar , et al., “Valve‐in‐Valve Transcatheter Aortic Valve Implantation Versus Repeat Surgical Aortic Valve Replacement in Patients With a Failed Aortic Bioprosthesis,” Euro Intervention 17 (2022): 1227–1237.34521614 10.4244/EIJ-D-21-00472 PMC 9724873 · doi ↗ · pubmed ↗
- 5M. Raschpichler , S. de Waha , D. Holzhey , et al., “Valve‐in‐Valve Transcatheter Aortic Valve Replacement Versus Redo Surgical Aortic Valve Replacement for Failed Surgical Aortic Bioprostheses: A Systematic Review and Meta‐Analysis,” Journal of the American Heart Association 11 (2022): e 7965.36533610 10.1161/JAHA.121.024848 PMC 9798815 · doi ↗ · pubmed ↗
- 6T. Nagasaka , O. Koren , V. Patel , et al., “Two‐Year Outcomes of Valve‐in‐Valve Using New‐Generation Transcatheter Devices Compared With Redo‐SAVR,” The American Journal of Cardiology 207 (2023): 380–389.37778227 10.1016/j.amjcard.2023.08.147 · doi ↗ · pubmed ↗
- 7M. Abdel‐Wahab , M. Simonato , A. Latib , et al., “Clinical Valve Thrombosis After Transcatheter Aortic Valve‐in‐Valve Implantation,” Circulation. Cardiovascular Interventions 11 (2018): 006730.10.1161/CIRCINTERVENTIONS.118.00673030571208 · doi ↗ · pubmed ↗
- 8F. D'Ascenzo , S. Salizzoni , A. Saglietto , et al., “Incidence, Predictors and Cerebrovascular Consequences of Leaflet Thrombosis After Transcatheter Aortic Valve Implantation: A Systematic Review and Meta‐Analysis,” European Journal of Cardio‐Thoracic Surgery 56 (2019): 488–494.31321408 10.1093/ejcts/ezz 099 · doi ↗ · pubmed ↗