Miller Fisher Syndrome With Syndrome of Inappropriate Antidiuretic Hormone Secretion: A Case Report
Khaing Zin That, Kai Xiong Lim, Marc Hai Liang Wong

TL;DR
A 70-year-old man with a rare neurological condition also had a hormone disorder, which was successfully managed with supportive care.
Contribution
This case report highlights the rare co-occurrence of Miller Fisher syndrome and SIADH, emphasizing the importance of early diagnosis and management.
Findings
The patient presented with incomplete Miller Fisher syndrome and syndrome of inappropriate antidiuretic hormone secretion.
Supportive treatment with fluid restriction and oral sodium chloride resolved symptoms within eight weeks.
Anti-GQ1b IgG antibodies confirmed the diagnosis of Miller Fisher syndrome.
Abstract
We report the case of a 70-year-old man with an incomplete form of Miller Fisher syndrome (MFS) complicated by syndrome of inappropriate secretion of antidiuretic hormone (SIADH). He presented with diplopia two weeks after a respiratory infection. Neurological examination showed bilateral pupil-sparing third nerve palsy, with normal reflexes, gait, coordination, power, and sensation. Serum sodium was markedly low (112 mmol/L) at presentation, with low serum osmolality, high urine sodium, and elevated urine osmolality. Anti-GQ1b IgG antibodies were positive, confirming the diagnosis of MFS. He was managed supportively with fluid restriction and oral sodium chloride tablets. He did not receive intravenous immunoglobulin. Symptoms resolved completely after eight weeks. This case underscores the importance of recognizing incomplete presentations of MFS and highlights the rare but clinically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
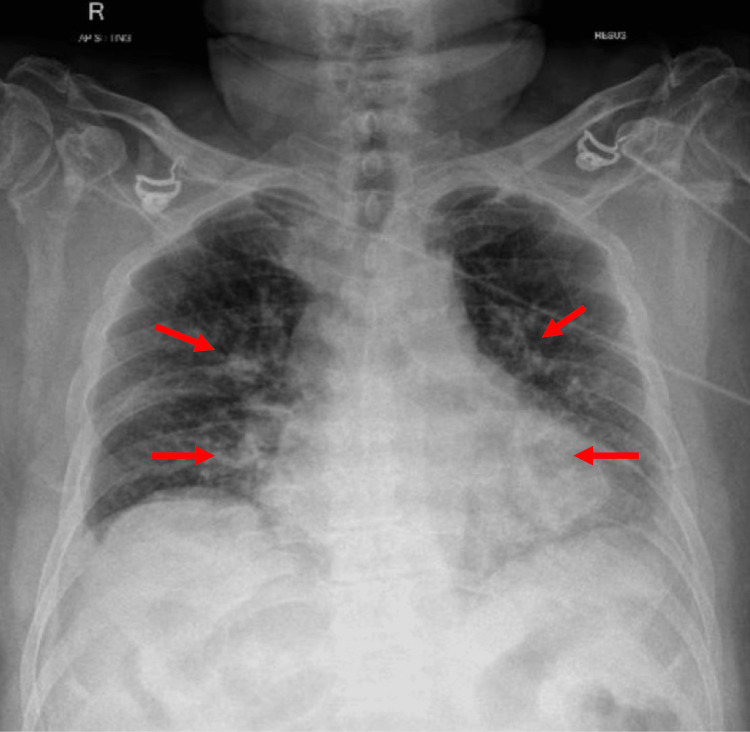 Figure 1
Figure 1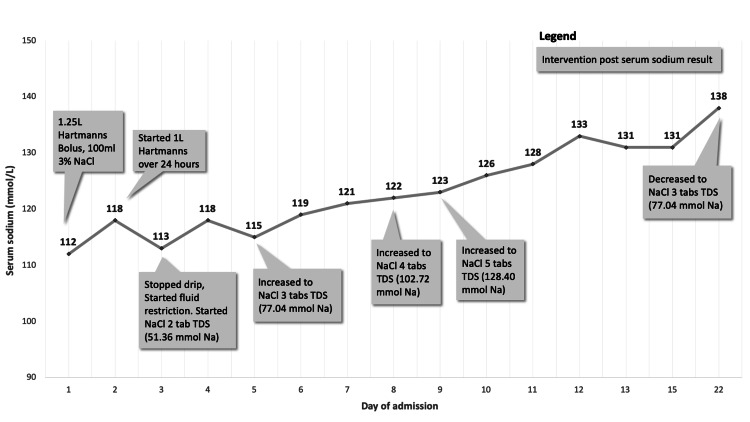 Figure 2
Figure 2| Investigations | Value | Normal values | |
| Complete blood count | Hemoglobin (g/dL) | 15.3 | 12.0–16.0 |
| White blood cell count (×109/L) | 13.77 | 4.00–10.00 | |
| Platelets (×109/L) | 305 | 140–440 | |
| Neutrophil absolute (×109/L) | 9.92 | 2.00–7.50 | |
| Renal panel | Urea (mmol/L) | 3.5 | 2.5–7.8 |
| Sodium (mmol/L) | 112 | 136–145 | |
| Potassium (mmol/L) | 4.3 | 3.5–5.1 | |
| Chloride (mmol/L) | 80 | 98–107 | |
| Bicarbonate (mmol/L) | 18.2 | 22–29 | |
| Creatinine (µmol/L) | 57 | 45–84 | |
| Other investigations | Protein total, serum (g/L) | 73 | 68–85 |
| Albumin, serum (g/L) | 43 | 35–50 | |
| Bilirubin, total (µmol/L) | 27 | ≤21 | |
| Alkaline phosphatase, serum (U/L) | 63 | 40–129 | |
| Alanine transaminase, serum (U/L) | 18 | ≤50 | |
| Aspartate transaminase, serum (U/L) | 21.6 | 11.9–21.6 | |
| C-reactive protein, serum (mg/L) | 17.7 | 0.2–9.1 | |
| Investigation | Value | Normal values |
| Serum sodium (mmol/L) | 113 | 136–145 |
| Serum osmolality (mOsm/kg H2O) | 247 | 275–301 |
| Urine osmolality (mOsm/kg H2O) | 720 | 50–1,200 |
| Urine sodium (mmol/L) | 131 | - |
| Serum cortisol (8 AM) (nmol/L) | 488 | 133–537 |
| Thyroid-stimulating hormone, serum (mIU/L) | 1.780 | 0.270–4.200 |
| Thyroxine (T4), free, serum (pmol/L) | 21.6 | 11.9–21.6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Hereditary Neurological Disorders · Autoimmune Neurological Disorders and Treatments
Introduction
Miller Fisher syndrome (MFS) was first described in 1956 as a variant of Guillain-Barré syndrome (GBS) [1], characterized by acute neuropathy from inflammation mediated by antibodies against neuronal membrane gangliosides. MFS is strongly associated with anti-GQ1b IgG antibodies, where GQ1b ganglioside is abundantly present in cranial nerves III, IV, and VI and the dorsal root ganglia [2,3]. The classical presentation of MFS is a triad of ophthalmoplegia, ataxia, and areflexia. However, the syndrome may not always manifest fully, resulting in diagnostic confusion. Incomplete forms, such as isolated ophthalmoplegia without ataxia or areflexia, can lead to delayed or missed diagnoses [4,5]. While hyponatremia secondary to the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) is well-documented in GBS, its occurrence in MFS is considerably less common and infrequently reported.
Case presentation
A 70-year-old male with a history of hypertension was brought to the emergency department following a fall due to acute-onset diplopia. He reported a one-day history of shortness of breath, two weeks of purulent cough and rhinorrhea, and three days of diarrhea and vomiting.
On admission, vital signs showed blood pressure of 160/119 mmHg, pulse rate of 76 beats/minute, respiratory rate of 16 breaths/minute, and oxygen saturation of 86% on room air, which improved to 100% with supplemental oxygen. There were bilateral lower-zone lung crepitations, normal abdominal findings, and no pedal edema. Examination of the eyes showed limited bilateral adduction and supraduction with normal pupillary reflexes, suggestive of bilateral pupil-sparing third nerve palsy. He had normal power, sensation, balance, coordination, and gait. Bilateral knee and ankle reflexes were normal.
Laboratory tests revealed severe hyponatremia (112 mmol/L), normal renal function, and elevated serum lactate (2.8 mmol/L). Chest radiography showed patchy airspace opacities in bilateral lower zones and perihilar regions consistent with pneumonia (Figure 1).
Chest radiograph showing bilateral pneumonia, with arrows indicating patchy opacities in the bilateral lower zones and perihilar regions.
Initial investigations are shown in Table 1. Cerebrospinal fluid analysis was not done as the patient declined a lumbar puncture.
He was treated for community-acquired pneumonia with IV ceftazidime and levofloxacin, which were later switched to oral Augmentin for a total duration of 10 days. Serum C-reactive protein levels downtrended quickly from 17.7 mg/L to 4.4 mg/L by the fifth day of antibiotic treatment.
MRI of the brain was normal. Anti-GQ1b ganglioside IgG antibodies were strongly positive, confirming MFS, while acetylcholine receptor antibodies were negative. Intravenous immunoglobulin was not administered due to ongoing improvement in symptoms.
Hyponatremia was initially thought to be due to hypovolemia from gastrointestinal losses. As the patient was symptomatic, he was given a 100 mL bolus of 3% NaCl, 1,250 mL bolus of Hartmann’s solution, and subsequently started on 1 L of Hartmann’s solution over 24 hours. After an initial response, serum sodium levels dropped again on day three of admission while he was on fluid replacement. By then, the patient was euvolemic and work-up demonstrated SIADH, as illustrated in Table 2.
He required high-dose oral sodium chloride tablets due to persistent SIADH. Figure 2 shows a graph of the serum sodium levels during admission and the corresponding treatment.
Graph illustrating serum sodium levels and corresponding treatment.
SIADH eventually resolved eight weeks after the initial presentation, concurrently with the resolution of bilateral third nerve palsy.
Discussion
This case illustrates the pertinent and lesser-known aspects of MFS. First, MFS can present in incomplete forms, which pose a diagnostic challenge. Additionally, SIADH can be a significant but rare complication of MFS.
Diagnostic challenges of incomplete forms of MFS
MFS is rare, with an estimated incidence of 1-2 cases per 1,000,000 people [5], and incomplete forms of MFS are underrecognized in clinical practice. Incomplete forms of MFS include acute ophthalmoplegia without ataxia and acute ataxic neuropathy without ophthalmoplegia [6]. Our patient’s presentation with isolated bilateral pupil-sparing third nerve palsy, without ataxia or areflexia, exemplifies this diagnostic challenge. Important differentials to consider for unexplained diplopia are ocular myasthenia gravis and brainstem stroke.
Retrospectively, the acuity of symptoms, presence of antecedent respiratory illness [7], and positive anti-GQ1b IgG antibodies clarify the diagnosis of incomplete MFS. Serum anti-GQ1b IgG antibodies are useful in diagnosing MFS given their high specificity and sensitivity [8]. Clinicians should thus remain vigilant to incomplete presentations of MFS and consider anti-GQ1b antibody testing early, especially in cases with ophthalmoplegia following recent infection.
Association between MFS and SIADH
Only a few cases of MFS complicated by SIADH have been documented in the literature [9-11]. The pathophysiology is presumably similar to GBS, involving autoimmune-mediated dysfunction of autonomic fibers or central regulation pathways of antidiuretic hormone [12-14].
In our patient, hypothyroidism and adrenal insufficiency were first excluded in the evaluation of euvolemic hyponatremia before a diagnosis of SIADH was made. Other common causes of SIADH were reasonably excluded, as there were no central nervous system lesions or causative medications. Although the patient had pneumonia, he promptly recovered from the infection, as evidenced by the normalization of serum C-reactive protein levels by day five of admission. The persistence of severe hyponatremia despite the resolution of pneumonia suggests that MFS is the cause of SIADH instead. Furthermore, the temporal correlation between neurological symptom resolution and normalization of sodium levels supports the relationship between MFS and SIADH. Severe hyponatremia from SIADH may cause life-threatening complications [9]. It is crucial to detect and manage SIADH promptly in patients with MFS to prevent poor patient outcomes.
Conclusions
This case underscores several key learning points. Clinicians should remain vigilant for incomplete presentations of MFS, such as isolated ophthalmoplegia. In such cases, early testing for anti-GQ1b IgG antibodies can accurately distinguish MFS from other disorders. While SIADH is uncommon in MFS, it should be actively looked for and managed due to the potential for severe complications. Prompt recognition of SIADH in patients with MFS is essential, as targeted management including fluid restriction and sodium supplementation can significantly impact patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An unusual variant of acute idiopathic polyneuritis (syndrome of ophthalmoplegia, ataxia and areflexia)N Engl J Med Fisher M 576525519561333479710.1056/NEJM 195607122550201 · doi ↗ · pubmed ↗
- 2Miller Fisher's syndrome Semin Neurol Teener JW 5125163220122367765910.1055/s-0033-1334470 · doi ↗ · pubmed ↗
- 3Ganglioside composition of the human cranial nerves, with special reference to pathophysiology of Miller Fisher syndrome Brain Res Chiba A Kusunoki S Obata H Machinami R Kanazawa I 32367451997903739110.1016/s 0006-8993(96)01123-7 · doi ↗ · pubmed ↗
- 4Acute ophthalmoparesis (without ataxia) associated with anti-GQ 1b Ig G antibody: clinical features Ophthalmology Yuki N Odaka M Hirata K 19620010820011115028910.1016/s 0161-6420(00)00420-6 · doi ↗ · pubmed ↗
- 5Miller-Fisher syndrome after first dose of Oxford/Astra Zeneca coronavirus disease 2019 vaccine: a case report J Med Case Rep Pirola FJ Santos BA Sapienza GF Cetrangolo LY Geranutti CH de Aguiar PH 4371620223638458410.1186/s 13256-022-03592-4PMC 9667853 · doi ↗ · pubmed ↗
- 6Guillain-Barré syndrome Lancet Willison HJ Jacobs BC van Doorn PA 71772738820162694843510.1016/S 0140-6736(16)00339-1 · doi ↗ · pubmed ↗
- 7Antecedent infections in Fisher syndrome: a common pathogenesis of molecular mimicry Neurology Koga M Gilbert M Li J 160516116420051588332410.1212/01.WNL.0000160399.08456.7C · doi ↗ · pubmed ↗
- 8Serum and CSF GQ 1b antibodies in isolated ophthalmologic syndromes Neurology Spatola M Du Pasquier R Schluep M Regeniter A 178017848620162698494710.1212/WNL.0000000000002558 · doi ↗ · pubmed ↗