Persistent Asymptomatic Pneumoperitoneum With Spontaneously Resolving Idiopathic Pneumatosis Intestinalis: A Case Report
John P. Ratanawong, Tzu Han Huang, Torben H. Urdahl, Katherine Weir, Anthony T. Rezcallah

TL;DR
A patient with asymptomatic pneumoperitoneum and intestinal gas was managed without surgery over 8 months.
Contribution
This case highlights nonoperative management of massive free air without underlying disease.
Findings
The patient had no symptoms despite significant free air under the diaphragm.
Longitudinal observation avoided unnecessary surgery in a stable patient.
No underlying systemic disease was identified after thorough evaluation.
Abstract
We present our experience with a patient with acute-on-chronic asymptomatic pneumoperitoneum with spontaneously resolving idiopathic pneumatosis intestinalis that was solely managed on close observation alone. This case is unique in that it details the approach to nonoperative management of massive free air under the diaphragm identified incidentally on routine preventative health screening and longitudinal follow-up over an 8-month period. In the absence of known and underlying systemic disease, efficient and coordinated clinical work-up and evaluation for comorbid diagnoses associated with pneumoperitoneum can serve to guide management and avoid unnecessary surgery for stable and asymptomatic patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
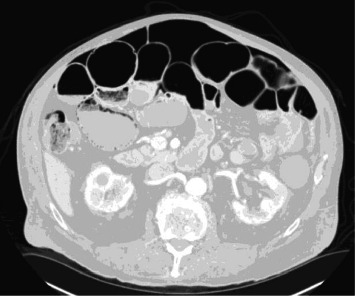 Figure 1
Figure 1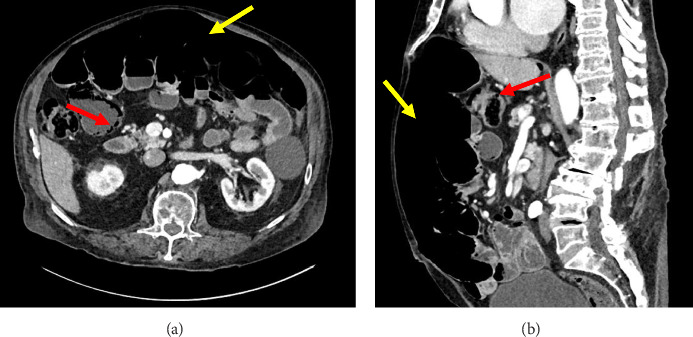 Figure 2
Figure 2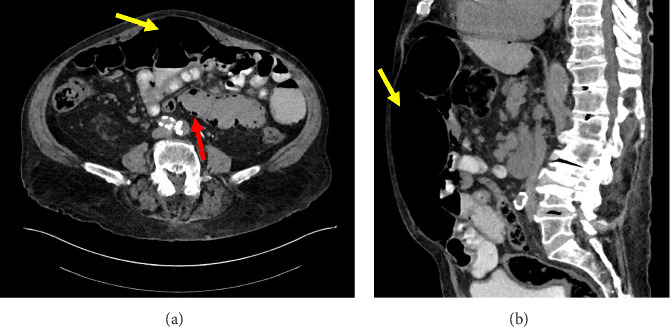 Figure 3
Figure 3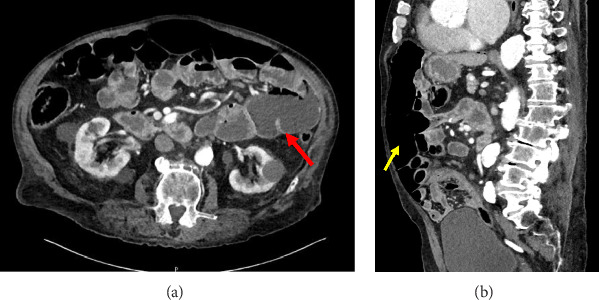 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Abdominal Surgery and Complications · Pneumothorax, Barotrauma, Emphysema
1. Introduction
Massive free air in the abdomen or pneumoperitoneum is an acute radiographic finding that can be associated with life-threatening diagnoses, often requiring immediate operative management. Very seldom is spontaneous pneumoperitoneum found to have a benign etiology, as most symptomatic cases are attributable to infectious, iatrogenic, inflammatory, and other causes that ultimately lead to an acute abdomen [1]. Cases of asymptomatic, idiopathic pneumoperitoneum due to pneumatosis intestinalis or intramural gas found within the bowel wall are even more rare. To date, there have been only a handful of cases of pneumoperitoneum secondary to underlying pneumatosis intestinalis in the published literature. Here, we describe a patient who presented with asymptomatic pneumoperitoneum incidentally found on radiographic imaging and also idiopathic small bowel pneumatosis that spontaneously resolved with observation alone.
2. Case Presentation
An 84-year-old man with a history of heart failure with preserved ejection fraction, chronic kidney disease, and chronic obstructive pulmonary disease presented to the radiology outpatient department for low-dose CT imaging for routine lung nodule surveillance. After the patient was sent home, the reviewed images demonstrated incidental massive free air within the upper abdomen, resulting in the staff radiologist calling the patient informing him that he needed to return to the emergency department (Figure 1). He did not report any recent episodes of acute abdominal pain, nausea, vomiting, shortness of breath, chest pain, or changes in bowel or bladder habits. Table 1 provides a brief summary of his medical history, surgical history, and medications.
In the emergency department, he was afebrile with vital signs within normal limits and benign findings on examination. In particular, mild abdominal distension and diastasis recti were noted on abdominal examination that was otherwise unremarkable for any acute changes concerning for peritonitis and small bowel obstruction in the setting of volvulus, appendicitis, or hernias. Likewise, his laboratory testing, which included a comprehensive metabolic panel and complete blood count, was also nonconcerning. The patient reported his last bowel movement was earlier that morning. At that time, he was given prophylactic intravenous piperacillin/tazobactam in case of a possible bowel perforation. Following this, a CT abdomen/pelvis was obtained which identified significant free air within the anterior abdomen and pneumatosis intestinalis of several dilated loops of small bowel in the right mid-abdomen. Other findings included a mild twisting of the mesentery, redundant distal small bowel loops, and a normal appearing colon (Figure 2). Given his clinically asymptomatic status and negative history of prior abdominal or endoscopic surgeries, he was subsequently admitted for observation with possible exploratory laparotomy if the patient demonstrated signs of decompensation. He was later discharged after an uneventful 2-day hospital stay, where he tolerated a regular diet, independent ambulation, and spontaneous voiding. He was then scheduled for monthly outpatient follow-up with general surgery.
One month after his initial encounter, the patient presented back to the emergency department to ask questions about the etiology of his unexplained pneumoperitoneum. He denied any changes in his clinical status since his last outpatient follow-up and continued to be clinically asymptomatic with benign laboratory testing and a nonsurgical abdomen on exam. Repeat CT imaging redemonstrated the existing pneumoperitoneum, pneumatosis, and dilated loops of small bowel with intact mesenteric vasculature (Figure 3). After discussing the findings with no clear underlying cause for his presentation, we recommended further in-patient observation. The patient declined to be admitted, but he was cautioned to return if experiencing new onset bowel symptoms. He had regular follow-ups afterward at 1-month and 6-month intervals, with no change in his asymptomatic condition.
Eight months after his initial presentation, he returned to the hospital with acute onset epigastric “spasm-like” abdominal pain that worsened after a bowel movement. On CT imaging, he still had free air within the upper abdomen, although less than 8 months prior. There was also complete resolution of the LUQ small bowel loop pneumatosis, but with new fluid-filled small bowel dilations, as well as areas concerning for possible stricture (Figure 4). His benign physical examination was reassuring for no acute surgical emergency and improving benign pneumoperitoneum. He was discharged after 3 days of observation for concomitant generalized weakness and continued to follow-up with his primary care provider. His abdomen remains nonsurgical and he continues to have asymptomatic pneumoperitoneum without known recurrence of his pneumatosis on conservative management only.
3. Discussion
Spontaneous idiopathic pneumoperitoneum in the setting of benign pneumatosis intestinalis has shown to be a difficult clinical problem to investigate, as the majority of the literature consists of case reports with few robust studies. This is mainly due to the extreme rarity of encountering both extraluminal free air that is spontaneous as well as pneumatosis intestinalis in a benign abdomen. Notably, there has only been one published report that closely matches the presented case. However, in that report, the patient's persisting pneumoperitoneum with resolved pneumatosis was linked to chronic systemic sclerosis, a known cause of both of these phenomena [2]. A study by Adachi et al. [3] observed similar cases, but with pneumatosis resolving within 7 days on follow-up CT and persistent extraluminal free air linked to bowel perforation, not idiopathic causes. Thus, to the best of our knowledge, we believe this is the first reported case of completely asymptomatic longstanding pneumoperitoneum in the setting of benign idiopathic pneumatosis intestinalis that spontaneously resolved with observation.
Table 2 outlines the known etiologies of both pneumatosis intestinalis and pneumoperitoneum [1, 4–8]. The pathogenesis of pneumatosis intestinalis is unclear, although there have been several theories devised, including mechanical, bacterial, pulmonary, and chemical [6, 7]. The mechanical theory states that increased intraluminal pressure from mechanical disturbances (e.g., trauma, gastrointestinal procedures, and bowel obstruction) can lead to gas intrusion into the intestinal wall. The bacterial theory suggests that gas-producing gut microbes can translocate into intestinal wall and produce excessive hydrogen gas causing pneumatosis intestinalis. The pulmonary theory hypothesizes that pulmonary diseases (e.g., asthma and COPD) can result in alveoli rupture and air entering the mediastinum that then dissects along the aorta, into the mesenteric vessels, and ultimately end up in the intestinal walls. Last, the chemical theory proposes that malnutrition can lead to decrease in carbohydrate breakdown and increased bacterial fermentation in the bowel, producing excessive gas byproducts [9]. With respect to our patient, the pulmonary theory is the most applicable to understand the driving forces behind his unique presentation, given that his medical history is notable for COPD and no other systemic disease. However, it remains unclear how much of his presentation can be explained by his pulmonary disease alone, since this is the first documented case of spontaneous pneumoperitoneum with benign pneumatosis intestinalis in the absence of any systemic disease or identifiable cause.
Despite an exceptionally unique presentation, timely recognition of massive free air by the radiologists allowed our patient to be quickly recalled back for urgent evaluation from the outpatient setting and community. This decision resulted in efficient coordination of care between radiology, emergency medicine, and surgery to both stabilize and monitor the patient for signs of acute decompensation and the need for emergent intervention. While the patient never reached acute status, this enabled the care team to establish a baseline and readily follow his case over the course of 8 months from his initial presentation on medical management alone. This patient's asymptomatic presentation in the absence of an acute abdomen and its chronicity documented over several months provide a helpful framework to inform clinical decision-making in determining the appropriateness for urgent or emergent surgical intervention versus careful observation with close follow-up and routine monitoring. This is especially useful when encountering such an exceedingly rare combination of both asymptomatic pneumoperitoneum and benign pneumatosis intestinalis without any known underlying risk factors.
4. Conclusions
Chronic asymptomatic massive pneumoperitoneum with eventual spontaneous resolution of pneumatosis intestinalis in a patient with a nonsurgical abdomen is rare. When incidentally found and the chronicity is not yet appreciated, this condition requires timely and coordinated evaluation and workup in the urgent setting given the possible surgical causes. In the absence of an acute surgical abdomen and known, underlying systemic disease, massive pneumoperitoneum can be successfully approached with expectant management and the flexibility to shift to operative management, should the patient's course mandate it.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Scoglio D. Pozzobon M. Battistioli M. Asymptomatic Pneumoperitoneum or Pneumatosis Cystoides Intestinalis? Easy to Make a Mistake Journal of Surgical Case Reports 20212021410.1093/jscr/rjab 138rjab 138PMC 806846533927871 · doi ↗ · pubmed ↗
- 2Vischio J. Matlyuk-Urman Z. Lakshminarayanan S. Benign Spontaneous Pneumoperitoneum in Systemic Sclerosis JCR: Journal of Clinical Rheumatology 201016837938110.1097/RHU.0b 013e 3181 ffeb 492-s 2.0-7865041458321085017 · doi ↗ · pubmed ↗
- 3Adachi W. Matsushita T. Yashiro Y. Imura J. Shiozawa H. Kishimoto K. Clinical Characteristics of Pneumoperitoneum With Pneumatosis Intestinalis Detected Using Computed Tomography: A Descriptive Study Medicine 2020994010.1097/MD.0000000000022461 e 22461 PMC 753575833019436 · doi ↗ · pubmed ↗
- 4Hannan E. Saad E. Hoashi S. Toomey D. The Clinical Dilemma of the Persistent Idiopathic Pneumoperitoneum: A Case Report International Journal of Surgery Case Reports 201963101210.1016/j.ijscr.2019.08.0152-s 2.0-8507185241531499325 PMC 6734534 · doi ↗ · pubmed ↗
- 5Sooby P. Harshen R. Joarder R. An Unusual Triad of Pneumatosis Intestinalis, Portal Venous Gas and Pneumoperitoneum in an Asymptomatic Patient Journal of Surgical Case Reports 20152015410.1093/jscr/rjv 035rjv 035PMC 439099225858266 · doi ↗ · pubmed ↗
- 6Zaki-Metias K. M. Zarour C. C. Mian A. Asymptomatic Pneumoperitoneum in the Setting of Pneumatosis Intestinalis: A Benign Entity or Surgical Emergency? Clinical Imaging 20217610410810.1016/j.clinimag.2021.02.01133582616 · doi ↗ · pubmed ↗
- 7Ho L. M. Paulson E. K. Thompson W. M. Pneumatosis Intestinalis in the Adult: Benign to Life-Threatening Causes American Journal of Roentgenology 200718861604161310.2214/AJR.06.13092-s 2.0-3424988331617515383 · doi ↗ · pubmed ↗
- 8Mularski R. A. Ciccolo M. L. Rappaport W. D. Nonsurgical Causes of Pneumoperitoneum The Western Journal of Medicine 1999170141469926735 PMC 1305434 · pubmed ↗