Effect of weight gain on blood pressure in Ugandan persons with HIV on dolutegravir/lamivudine/ tenofovir disoproxil fumarate over 48 weeks
Willington Amutuhaire, Barbara Castelnuovo, Nele Brusselaers, Martin Nabwana, Lal Muhammad, Brendan Maloney, Bridgette Nixon, Jean-Marc Schwarz, Frank Mulindwa

TL;DR
This study found that weight gain in Ugandan HIV patients taking dolutegravir-based treatment is linked to increased blood pressure over 48 weeks.
Contribution
The study provides new evidence linking dolutegravir-induced weight gain to higher blood pressure risk in HIV patients in Uganda.
Findings
A moderate positive linear relationship was found between weight gain and mean arterial pressure increase.
Each 1 kg weight gain was associated with a 0.62 mmHg increase in mean arterial pressure.
Weight gain on dolutegravir-based ART may heighten the risk of hypertension in HIV patients.
Abstract
Most people living with HIV in low and middle-income countries are taking fixed dose combination tenofovir disoproxil fumarate/lamivudine/dolutegravir (TLD). Dolutegravir use has been associated with weight gain, a known risk factor for hypertension. We aimed to determine if weight gain in Ugandan anti-retroviral therapy (ART) naïve patients on TLD correlated with increase in blood pressure. We analyzed data from the ‘Glucose metabolism changes in Ugandan persons with HIV (PLHIV) on Dolutegravir (GLUMED)’ study which was a prospective cohort study with ART naïve persons with HIV ≥ 18 years followed up on TLD over 48 weeks. A scatter plot with 95% confidence intervals and regression line illustrating the relationship between weight change and mean arterial pressure (MAP) change from baseline to 48 weeks was created. To further examine the effect of weight change on MAP, we performed a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
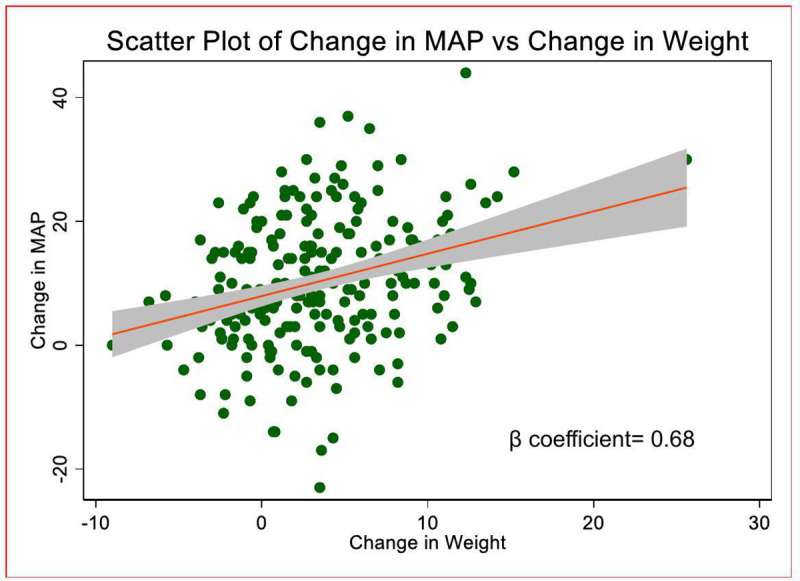 Fig 1
Fig 1- —http://dx.doi.org/10.13039/100000061Fogarty International Center
- —http://dx.doi.org/10.13039/100008673Center for AIDS Research, University of California, San Diego
- —http://dx.doi.org/10.13039/100000061Fogarty International Center
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV-related health complications and treatments · Diet and metabolism studies · Liver Disease Diagnosis and Treatment
Background
Over 80% persons living with HIV in low and middle-income countries were taking fixed dose combination tenofovir disoproxil fumarate/lamivudine/dolutegravir (TLD) by mid-2024, more so countries supported by the U.S. President’s Emergency Plan for AIDS Relief [1,2]. The widespread uptake followed WHO recommendations in 2016 and later 2018 recommending dolutegravir (DTG) anchored anti-retroviral therapy (ART) use as first line and optional second line therapy, respectively [3,4]. The recommendations followed reports of increased resistance to non-nucleoside reverse transcriptase inhibitors (NNRTIs) as well as multiple advantages of DTG including; having a high genetic barrier to resistance, a good side effect profile, high efficacy and less drug-drug interactions [5,6]. Dolutegravir use however has been associated with weight gain when compared to other anchor drugs like non-nucleoside reverse transcriptase inhibitors and protease inhibitors [7–10].
Obesity is a risk factor for dyslipidemia, glucose dysmetabolism, cardiovascular disease and hypertension [11–13]. With mortality and morbidity in persons living with HIV (PLHIV) shifting from AIDS associated opportunistic infections to non- infectious diseases like cardiovascular diseases, renal disease, liver failure and non–AIDS defining malignancies, it is pertinent to understand the risk posed by different ART regimens to inform surveillance decisions as well as ART choice decisions in primary care [14–18]. Whether the weight gain from integrase inhibitors, in particular DTG translates into dyslipidemia, glucose dysmetabolism, cardiovascular disease and hypertension is still subject to research.
There is growing evidence to demonstrate that weight gain noticed in patients on dolutegravir is associated with increased blood pressure as compared to patients on other regimens as demonstrated by two studies with both ART naïve and experienced adults [8,19,20] We sought to evaluate in a Ugandan cohort of PLHIV if weight gain over 48 weeks on TLD correlated with changes in blood pressure. Our cohort was of particular interest because it was composed of younger participants with minimal other risk factors for hypertension.
Methods
Study design and setting
The participants of the study were recruited in the ‘Glucose metabolism changes in Ugandan persons living with HIV (PLHIV) on Dolutegravir (GLUMED)’ study which was a prospective cohort study at the Kisenyi Health Center IV HIV clinic, in Uganda’s capital city, Kampala [21–23]. The primary objective of the study was to describe glucose metabolism changes in participants over 48 weeks on dolutegravir based ART.
Study participants and study processes
The GLUMED study was conducted between January/2021 and September/2023. ART naïve PLHIV aged 18 years or more were recruited excluding pregnant women and very sick patients unable to undergo a 2 hour- oral glucose tolerance test (OGTT).
Baseline demographic, clinical and social data were collected. Enrolled patients were prospectively followed up with 2 hour- oral glucose tolerance tests (OGTT), body mass index, waist circumference, blood pressure measurements, adherence counselling and assessment as well as assessment of concurrent medications at 12, 24, 36 and 48 weeks. At every visit, a protocol-based procedure was used to measure blood pressure. After a 5 minutes rest, using a Welch Allyn Vital Signs Monitor, 300 Series 53NT0®, we measured patient blood pressures with patients seated upright with their backs to the chairs, feet flat on the floor and arms supported at heart level. A full description of the study protocol is described in our earlier publications [21,24]
Outcome
The primary outcome of the study was the change in mean arterial pressure (MAP) from baseline to 48 weeks. MAP is an index of systolic and diastolic blood pressure calculated by the formular; 1/3 systolic blood pressure + 2/3 diastolic blood pressure.
Statistical analysis
This study aimed to assess the effect of weight change on MAP changes between baseline and 48 weeks among participants, with adjustment for relevant covariates (sex, age, physical activity, and baseline HIV clinical stage). We performed secondary analysis of patient data collected in the GLUMED study excluding patients who had hypertension and were on treatment at baseline. We also excluded patients who were diagnosed with hypertension and started on anti-hypertensives during follow up.
Descriptive statistics were used to summarize baseline demographic and clinical characteristics. Continuous variables were reported as median (interquartile range (IQR)) due to their skewed distribution, while categorical variables were reported as counts and percentages.
A scatter plot with a 95% confidence interval and regression line illustrating the relationship between weight change and MAP change was created. This plot provides a visual representation of the strength and direction of the association. To further examine this association, we performed a linear regression analysis, with MAP change as the dependent variable and weight change as the independent variable. Both unadjusted and adjusted β-coefficients with 95% confidence intervals were estimated. The adjusted model included covariates selected based on clinical relevance and potential confounding, including sex, age, physical activity, and baseline HIV clinical stage. All analyses were conducted using Stata software (version 17.0), with a two-tailed significance level set at p < 0.05 for all tests.
Results
Of the 243 patients that completed 48 weeks of follow up in the GLUMED study, 23 patients were diagnosed with hypertension and were on hypertension treatment hence were not included in the final analysis, leaving 220 patients.
Of the 220 patients’ data analyzed, 129 (58.6%) were female. The median age of the participants was 31 years (IQR: 27.0–38.0) with a median CD4 cell count of 319.0 cells/mm^3^ (IQR: 160.0–524.0). The majority (212 (96.4%)) of the patients were in HIV clinical stage 1 with 3 (1.4%), 4 (1.8%), 1 (0.5%) being in HIV clinical stages 2,3 and 4 respectively. Seven (3.2%) patients had an established diagnosis of active tuberculosis diagnosed at enrollment into HIV care. Overall, 138 (62.7%) had a normal BMI, 48 (21.8%) were overweight, 22 (10.0%) underweight and 12 (5.5%) obese. About half (126 (57.3)) reported not taking alcohol. Most (180 (81.8%) of the patients self-reported as meeting WHO recommendations on physical activity for health. The median serum creatine, fasting LDL, fasting HDL and fasting total cholesterol at baseline were: 0.8 mg/dl, 77 mg/dl, 31.7 mg/dl and 134 mg/dl respectively. At 24 weeks of follow up, 215 (99.5%) patients had viral suppression. (baseline characteristics are summarized in Table 1)
Table 1: Baseline clinical and demographic characteristics of the study population.
Effect of change in weight on change in mean arterial pressure
We found a moderate positive linear relationship between weight gain and MAP over 48 weeks. On linear regression to determine the effect of change in weight over 48 weeks on change in MAP, after adjustment for sex, age, physical activity, and baseline HIV clinical stage in the final model, we found a significant adjusted β co-efficient of 0.62 (0.37, 0.86) (P < 0.001). The observed change in MAP was independent of other factors known to be risk factors for hypertension including baseline BMI, baseline renal function and waist circumference [31–33]. Table 2, Fig 1.
Table 2: Linear regression evaluating the effect of net weight change from baseline to 48 weeks on change in mean arterial pressure.
Scatter plot of change in mean arterial pressure versus change in weight with 95% confidence intervals.
Fig 1 On linear regression, after adjustment for sex, age, physical activity, andbaseline HIV clinical stage in the final model, the adjusted β co-efficient was 0.62 (0.37, 0.86) (P < 0.001).
Discussion
In this study, we determined the effect of weight gain on blood pressure (expressed as mean arterial pressure) over 48 weeks on TLD. We found a moderate positive linear relationship between weight gain and MAP with an increase of 0.68mmHG for every 1 kg increase in body weight over 48 weeks with consistent findings after adjusting for baseline age, sex, physical activity and baseline clinical stage.
Currently, the most used ART is fixed dose combination TLD in more than 80% PLHIV in low-middle income countries [1,2]. Dolutegravir based ART has been shown to induce weight gain compared to other anchor drugs [7–10]. Increased adiposity one of the characteristics of obesity is known to cause hypertension via various complex interlinked mechanisms including sympathetic nervous system overactivation, stimulation of the renin-angiotensin-aldosterone system, alterations in adipose-derived cytokines, insulin resistance, and structural and functional renal changes [11–13]. Determining if the reported weight gain in patients on TLD correlates with increasing blood pressure can help guide physician choices when individualizing anti-retroviral therapy as well as HIV national programs in designing hypertension surveillance strategies in this group of patients. A positive correlation between dolutegravir- associated weight gain with hypertension has been reported in other larger studies involving both ART naïve and ART exposed PLHIV before and after starting dolutegravir. These studies have had generally older patients with more risk factors for incident hypertension [8,19,20]. One such studies including data from the RESPOND cohort which is a consortium cohort of PLWH with a median age of 43 from 37 countries in Europe and Australia demonstrated that participants receiving INSTIs have a higher incidence of hypertension than those receiving NNRTIs [27]
In our study, we replicated these findings in a relatively younger population (median age; 31 years) with generally minimal other risk factors for hypertension, i.e., at baseline, majority were HIV stage I, were physically active, had normal weight and had normal median creatine levels. With other positive attributes to dolutegravir like having a high genetic barrier to resistance, having less drug- drug interactions, being a once daily drug, good tolerability and low cost of production, DTG is likely to remain part of preferred first line ART for PLHIV. The likely association with hypertension still warrants more research, especially in sub-Saharan Africa where resources for screening as well as treatment for hypertension are still limited. However, this growing evidence to suggest a tendency towards worsening high blood pressure in these patients may warrant intensified blood pressure surveillance in programmatic settings and as well aggressively optimize blood pressure treatment in hypertensive patients on DTG based ART.
Our study had limitations. With our study design, we could not demonstrate if the blood pressure increase we demonstrated is higher than what would be expected in patients on other ART regimens with similar increments in weight given we did not have a comparator group on other ART regimens. Additionally, we also had a limited period of follow-up (48 weeks). Despite the limitations, we had different strengths. Pregnant and breastfeeding mothers who are at risk of gestational hypertension were excluded. We also excluded participants who were on hypertension treatment as well as those with poor adherence to ART as all these could be potential confounders in the hypertension trajectories we report.
Conclusion
We demonstrated a positive linear relationship between weight gain and mean arterial pressure in Ugandan persons with HIV over 48 weeks on tenofovir disoproxil/ lamivudine/ dolutegravir. We provide additional evidence to suggest that the noticed weight gain after starting dolutegravir based ART may be associated with a heightened risk of incident hypertension.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global AIDS report — The Urgency of Now: AIDS at a Crossroads | UNAIDS [Internet]. 2024. [cited 2024 Dec 21]. Available from: https://www.unaids.org/en/resources/documents/2024/global-aids-update-2024
- 2WHO recommends dolutegravir as preferred HIV treatment option in all populations [Internet]. [cited 2022 Aug 15]. Available from: https://www.who.int/news/item/22-07-2019-who-recommends-dolutegravir-as-preferred-hiv-treatment-option-in-all-populations
- 3World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. WHO. 2018. http://www.who.int/hiv/pub/arv/arv-2016/en/
- 4Kandel CE, Walmsley SL. Dolutegravir – a review of the pharmacology, efficacy, and safety in the treatment of HIV. Drug Des Devel Ther. 2015;9:3547.10.2147/DDDT.S 84850 PMC 450060426185421 · doi ↗ · pubmed ↗
- 5WHO recommends dolutegravir as preferred HIV treatment option in all populations. https://www.who.int/news/item/22-07-2019-who-recommends-dolutegravir-as-preferred-hiv-treatment-option-in-all-populations. Accessed 2025 January 4
- 6Cardoso-NetoÉC, Netto EM, Brites C. Weight gain in patients starting dolutegravir-based ART according to baseline CD 4 count after 48 weeks of follow up. Brazilian J Infect Dis. 2023;27(5):102807.10.1016/j.bjid.2023.102807 PMC 1056998737788801 · doi ↗ · pubmed ↗
- 7Brennan AT, Nattey C, Kileel EM, Rosen S, Maskew M, Stokes AC, et al. Change in body weight and risk of hypertension after switching from efavirenz to dolutegravir in adults living with HIV: evidence from routine care in Johannesburg, South Africa. E Clinical Medicine. 2023;57.10.1016/j.eclinm.2023.101836 PMC 993266036816348 · doi ↗ · pubmed ↗
- 8Hirigo AT, Yilma D, Astatkie A, Debebe Z. Effect of dolutegravir-based first-line antiretroviral therapy on weight and body mass index among adult people living with HIV on follow up at health facilities in Hawassa city administration, Southern Ethiopia: a retrospective cohort study. Ann Med. 2023;55(2):2242250.37531412 10.1080/07853890.2023.2242250 PMC 10399476 · doi ↗ · pubmed ↗