Cracking the LUTS Code: A Pre-Urodynamic Tool for DU vs. BOO Diagnosis in Female Patients with Non-Neurogenic LUTS
Karolina Garbas, Łukasz Zapała, Aleksander Ślusarczyk, Tomasz Piecha, Piotr Radziszewski

TL;DR
This study creates a non-invasive tool to help doctors tell the difference between two bladder conditions in women without using invasive tests.
Contribution
A novel clinical prediction model is developed to distinguish detrusor underactivity from bladder outlet obstruction in women with lower urinary tract symptoms.
Findings
The model achieved a C-index of 0.779, indicating moderate predictive accuracy.
Key predictors included hesitancy, incomplete emptying, POP-Q staging, and UFL time to Qmax.
At a probability cutoff of 0.3, the model had 86.8% sensitivity and 82.1% negative predictive value.
Abstract
Background: Detrusor underactivity (DU) and bladder outlet obstruction (BOO) are common causes of voiding dysfunction in women with lower urinary tract symptoms (LUTS). However, differentiating between them remains challenging due to overlapping clinical presentations and a reliance on invasive urodynamic studies (UDS). This study aimed to develop a non-invasive, office-based clinical prediction model to distinguish DU from BOO in women with non-neurogenic LUTS. Methods: We conducted a retrospective analysis of 88 women who underwent pressure-flow studies at two outpatient clinics between 2012 and 2022. DU was defined using a projected isovolumetric pressure 1 (PIP1) < 30 cm H2O, and BOO was defined by a Female-Specific Bladder Outlet Obstruction Index (BOOIf) > 18. Clinical symptoms, uroflowmetry (UFL) parameters, and pelvic organ prolapse staging (POP-Q) were evaluated. A multivariate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
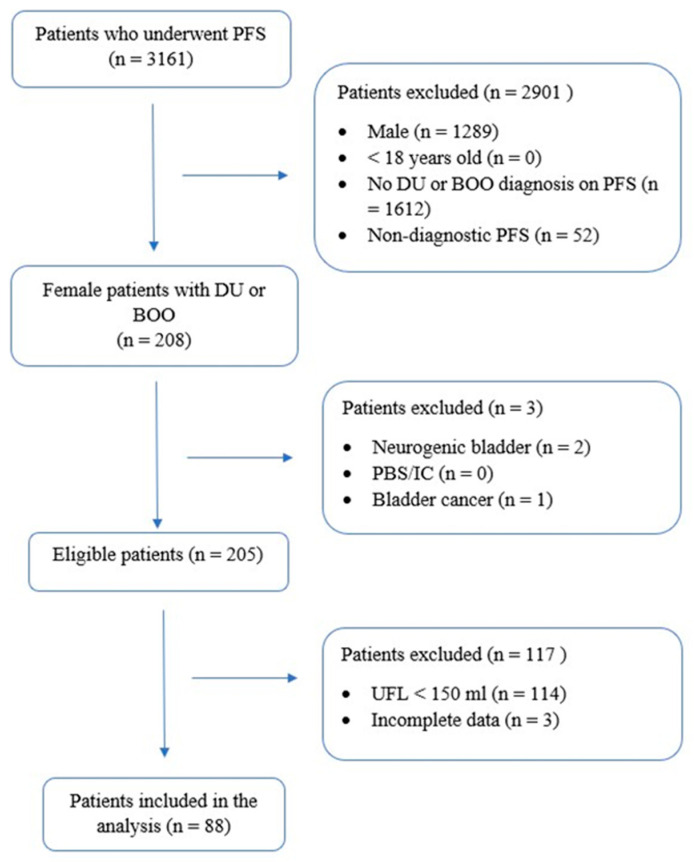 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic floor disorders treatments · Urinary Bladder and Prostate Research · Urinary Tract Infections Management
1. Introduction
Detrusor underactivity (DU) is increasingly recognized as a significant cause of voiding dysfunction (VD) in both men and women. However, data on female DU remain limited and, in some cases, contradictory. The reported prevalence rates of DU vary depending on the study population. Among women with lower urinary tract symptoms (LUTS) without cystocele, DU has been diagnosed in approximately 10% [1] to 17% [2] of cases. Furthermore, evidence suggests that the prevalence of DU increases with age [2]. Accurately determining its true prevalence is challenging due to the long-standing absence of standardized diagnostic criteria. In women attending pelvic floor clinics, DU prevalence varied substantially depending on the applied definition: 33.7% according to Schäfer’s detrusor factor, 37.0% using Abrams’ Bladder Contractility Index (BCI), and 4.1% based on Jeong’s criteria [3].
The International Continence Society (ICS) defines DU as a “detrusor contraction of reduced strength and/or duration, resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span” [4]. Bladder outlet obstruction, which can present with similar clinical symptoms, is defined as “the obstruction during voiding, (…) a reduced urinary flow rate and/or presence of a raised post-void residual and an increased detrusor pressure. (…) A urethral stricture or obstruction due to higher degrees of uterovaginal prolapse or obstructed voiding after stress incontinence procedures are among possible causes” [4].
Distinguishing DU from BOO remains diagnostically challenging, as the symptom overlap is considerable. Currently, urodynamic studies (UDS) are considered the gold standard for evaluating female VD, including DU and BOO [5]. However, until recently, the urodynamic criteria for diagnosing DU in women lacked precision and consistency.
Recent recommendations from the ICS and the Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU) strongly advise against using the BCI and its updated version—the ICS-Detrusor Contractility Index (ICS-DCI)—as a standard metric for female VD due to insufficient validation, particularly for diagnosing DU in individual women. While an ICS-DCI value greater than 100 is generally accepted as indicative of adequate detrusor voiding contraction (DVC), the clinical significance of ICS-DCI values below 100 remains unclear [6]. A study assessing isovolumetric contraction pressures found that the Detrusor/Bladder Contractility Index (D[B]CI) significantly overestimates isovolumetric (“stop-test”) detrusor pressures in women. In contrast, projected isovolumetric pressure 1 (PIP1 = PdetQmax + Qmax) has been shown to provide a more reliable estimate [7]. A PIP1 value below 30 cm H_2_O has been proposed as the lower limit for normal DVC [6]. For the diagnosis of BOO in females, a Female-Specific Bladder Outlet Obstruction Index (BOOIf) has been introduced, calculated as PdetQmax—2.2Qmax. A BOOIf value exceeding 18 has been identified as a strong predictor of BOO [8] and has been incorporated into the provisional ICS pressure-flow study (ICS-PFS) nomogram for women [6].
Despite these advancements in invasive diagnostics, no widely accepted non-invasive predictive model currently exists to differentiate DU from BOO in women. Therefore, the objective of this pilot study was to develop a first-stage, non-invasive, office-based model to support the diagnosis of DU in women with non-neurogenic LUTS and to differentiate it from BOO. This approach is intended to assist clinicians in making more efficient, evidence-informed decisions in the diagnostic workup of voiding dysfunction.
2. Materials and Methods
2.1. Patient Selection and Data Collection
We conducted a retrospective analysis of clinical records from 3161 patients who underwent pressure-flow assessments between 2012 and 2022 at two outpatient facilities. Individuals were referred for urodynamic testing due to new or persistent LUTS, unsuccessful conservative management, preoperative evaluation for urological or gynecological procedures, failure of previous invasive interventions, or preparation for kidney transplantation. Prior to undergoing pressure-flow studies (PFS), all patients had presented negative urine cultures confirming the absence of urinary tract infections. Each patient underwent a standard clinical evaluation, which included a thorough medical history covering comorbidities and current medications, completion of the Core Lower Urinary Tract Symptoms (CLSS) questionnaire [9], and a basic neurological examination [10], as previously described [11]. A urogenital examination was performed on every woman, and pelvic organ prolapse was staged according to the Pelvic Organ Prolapse Quantification (POP-Q) system [12]. Following these assessments, both a free-flow test and a PFS were performed.
The inclusion criteria for the study required participants to be adult females experiencing LUTS and diagnosed with either DU or BOO based on pressure-flow findings. Additionally, participants had to provide informed consent, undergo UFL with a voided volume exceeding 150 mL, and then subsequently undergo PFS. Patients were excluded from the study if they had a history of neurogenic bladder, painful bladder syndrome/interstitial cystitis (PBS/IC), bladder cancer, or if their PFS results were inconclusive (e.g., patient-interrupted tests, low voided volume, or displacement of bladder or rectal catheter during examination). Incomplete medical records also led to exclusion. Ultimately, 88 women met all criteria and were included in the final analysis (Figure 1). The study received approval from the Bioethics Committee of the Medical University of Warsaw (approval no. AKBE/335/2023).
The evaluated UFL parameters included maximum flow rate (Qmax), average flow rate (Qav), voided volume, time to reach Qmax, post-void residual urine (PVR), and flow-curve shape. Flow curves were categorized into predefined patterns, including bell-shaped, fluctuating, intermittent, fluctuating-intermittent, plateau, or atypical (not conforming to the aforementioned categories). Post-void residual urine was quantified via abdominal ultrasound following UFL, and the post-void residual ratio (PVR-R) was determined as the proportion of the PVR to total bladder volume (sum of voided volume and PVR). The PFS was conducted after UFL by urodynamic-trained experts in adherence to the ICS Good Urodynamics Practices protocol [13]. DU was identified based on a Projected Isovolumetric Pressure 1 (PIP1) calculation, using the formula: PIP1 = PdetQmax + Qmax [6]. BOO was diagnosed if the Female BOO Index (BOOIf), calculated using the equation BOOI = PdetQmax − 2.2Qmax, exceeded 18 [6]. The assessments were performed using Medtronic equipment (Duet Logic G/2, model: 9032A0173, Medtronic, Lublin, Poland). All recorded data were stored within the Medtronic software version 1.2 system and analyzed in accordance with ICS guidelines [4]. Each PFS underwent rigorous manual verification to identify and eliminate potential artifacts, ensuring data integrity. All validated findings were manually entered into the study database.
2.2. Statistical Analysis
Baseline demographic and clinical characteristics were summarized using medians with interquartile ranges for continuous variables, while categorical variables were reported as numbers with corresponding percentages. Comparisons of continuous variables were conducted using the Mann–Whitney U test, whereas categorical data were analyzed using Fisher’s exact test. To assess associations between variables, logistic regression was employed for both univariate and multivariate analyses. A multivariable analysis was carried out using a stepwise selection approach, where variables identified as relevant in univariate analyses were systematically introduced into the model. The stepwise selection process involved adding variables to the model based on an inclusion threshold of 0.2. Once incorporated, each variable was reassessed at every stage, and those with a p-value exceeding 0.2 were removed, ensuring that only predictors contributing to model optimization remained. This process continued iteratively until no further refinement was possible, and only statistically significant predictors were retained in the final model. Odds ratios with 95% confidence intervals were estimated through logistic regression. To evaluate the model’s performance, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. The model’s diagnostic accuracy was assessed using a probability cutoff of 0.3. Statistical significance was determined using two-sided p-values, with a threshold of <0.05. All statistical analyses were conducted using SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA). Given the limited sample size and preliminary scope, this study should be considered a pilot investigation aimed at generating hypotheses and informing the design of future validation studies.
3. Results
3.1. Baseline Characteristics
Eighty-eight women were included in the final analysis, of which 38 (43.19%) were diagnosed with DU and 50 (56.81%) with BOO. The median age of the patients with BOO was 56 (42–64) and of those with DU 59.5 (44–69). The main presenting symptom in 27 (30.68%) patients with DU was urgency, while among patients with BOO it was both urgency and nocturia, in 37 (42.05%) cases. In the CLSS questionnaire, the DU group recorded the highest median scores for frequency (2 points; range 0–2), nocturia (2 points; range 1–2), and urgency. In contrast, the BOO group’s highest score was for slow stream, with a mean of 3 points (range 0–3). The detailed symptoms and CLSS questionnaire scores are presented in Table 1.
Regarding chronic diseases, within the BOO group, diabetes mellitus (DM) was present in four (4.55%) patients and hypothyroidism in six (6.82%) patients. However, in the DU group, these comorbidities were present in three (3.41%) and six (6.82%) patients, respectively. Moreover, only two patients (2.27%) in the DU group used cholinolytics and none used alpha-blockers. In the BOO group, six patients (6.82%) were administered cholinolytics and three (3.41%) alpha-blockers. The drugs were continued until the urodynamic study. The continuation of baseline characteristics, including comorbidities and medications used, is presented in Supplementary Table S1.
On UFL, patients with DU had a median Qmax of 15.5 mL/s (10.9–20.1), a median voided volume of 274.5 (207–446), and a median time to Qmax of 15 s (6–26). Patients diagnosed with BOO demonstrated a similar median Qmax of 16.6 mL/s (11.6–20.5), similar median voided volume of 279 mL (IQR 202–406), and a shorter median time to Qmax of 9 s (6–13). The predominant UFL curve shapes observed in DU patients were fluctuating in 18 (20.45%) cases and fluctuating-intermittent in 13 (14.77%), mirroring the prevailing shapes in the BOO group (n = 21, 23.86%, n = 17, 19.32%, respectively). The median PIP1 in the DU group was 14.25 (7.4–21.9) and in the BOO group, 62.9 (49.7–89.7), while BOOIf measured 3.2 (0–7) in the DU patients and 34.8 (20.4–60) in the BOO women. Detailed urodynamic findings including the patterns of urine flow and detrusor voiding pressure curves are presented in Table 2.
3.2. Uni- and Multivariate Logistic Regression Analyses
In the univariate logistic regression analysis, only the time to Qmax on UFL (OR = 1.03, 95% CI 1.00–1.06, p = 0.04) and POP-Q < 3 on physical examination prior to UDS (OR = 4.10, 95% CI 1.08–15.62, p = 0.04) were statistically significant predictors of DU (p < 0.05). Complete univariate analyses for the prediction of DU are demonstrated in Table 3.
For the multivariate analysis, variables that demonstrated statistical significance or were on the threshold of significance in the univariate analyses (p < 0.2) were selected. Those parameters included hesitancy, incomplete emptying, straining points in CLSS, time to Qmax on UFL, and POP-Q < 3 in the clinical assessment. The final predictive model comprised three key factors: clinical symptoms, a UFL parameter, and the POP-Q assessment (Table 4).
The model indicated that the occurrences of hesitancy (OR = 2.06, 95% CI 0.71–5.98, p = 0.18) and incomplete emptying (OR = 3.52, 95% CI 1.27–9.79, p = 0.016), POP-Q < 3 (OR = 0.15, 95% CI 0.03–0.75, p = 0.02), and longer time to Qmax on UFL (OR = 1.05, 95% CI 1.02–1.09, p = 0.004) were significant predictors of DU diagnosis. The risk model incorporating these predictive factors for DU diagnosis in female patients with non-neurogenic LUTS due to DU or BOO achieved a Harrell’s Concordance Index (C-index) of 0.78. To assess the model’s diagnostic accuracy, a probability cutoff of 0.3 was applied. The resulting clinical diagnostic criteria for urodynamically confirmed DU exhibited a sensitivity of 86.8%, specificity of 46%, positive predictive value (PPV) of 55%, and negative predictive value (NPV) of 82.1%.
4. Discussion
The present study promotes the hypothesis that the evaluation of clinical symptoms, UFL analysis, and pelvic organ prolapse assessment using the POP-Q scale can serve as a non-invasive method for differentiating DU from BOO in female patients with LUTS. Our analysis led to the development of a predictive model indicating that hesitancy, incomplete emptying, prolonged time to Qmax on UFL, and POP-Q stage < 3 are significant predictors of DU, rather than BOO, in women with non-neurogenic LUTS. To our knowledge, this study is the first to employ PIP1 < 30, as currently recommended by ICS-SUFU [5], as a diagnostic criterion for DU in females. Additionally, it is the first to integrate a POP-Q assessment into a non-invasive model to distinguish between BOO and DU.
The proposed model incorporates clinically accessible parameters that do not require advanced diagnostic tools, beyond standard UFL, and can be assessed without catheterization. This is particularly relevant for elderly patients or those with comorbidities, who may be unable or unwilling to undergo UDS, or who may have difficulty cooperating during the procedure, potentially leading to biased or inconclusive results. Here, the rather young cohort tested had a median age of 56 years. Yet, a non-invasive approach improves patient accessibility and compliance, while also reducing the time and costs associated with diagnosis in all age groups. Early and accurate differentiation between DU and BOO is critical, as timely intervention can prevent complications such as chronic urinary retention, recurrent infections, and upper urinary tract damage. By offering a practical, efficient, and cost-effective diagnostic tool, this model has the potential to assist clinical decision-making, guide the need for invasive UDS, and optimize healthcare resource utilization.
Due to similarities between the symptoms of DU and BOO, both in men and women, it remains impossible to reliably differentiate between these two disorders based solely on the voiding or storage symptoms [14,15]. A study by D’Alessandro et al. demonstrated that in women attending a urogynecology clinic, among others, voiding/bulging symptoms and anterior and central prolapse were correlated positively with DU, whereas stress urinary incontinence showed an inverse relationship. However, the final diagnostic models exhibited poor accuracy across all evaluated definitions of DU, with the area under the curve (AUC) ranging between 0.64 and 0.72 [16]. Contrary to these findings, our study indicates that clinical symptoms, specifically hesitancy and incomplete emptying, can become valuable predictive factors once integrated into a broader diagnostic model. Although, to our knowledge, no previous studies specifically investigated a symptom-based model differentiating between DU and BOO in females, research in males by Gammie et al. observed incomplete emptying significantly more frequently in DU patients [17], supporting our findings. Nevertheless, it is important to acknowledge that self-reported symptoms are inherently subjective and may introduce variability between patients.
Interestingly, and in alignment with previous observations by Rubilotta et al. our analysis identified a POP-Q stage lower than 3 as a significant predictor of DU. Existing research has demonstrated a high prevalence (40.9%) of DU among patients with pelvic organ prolapse (POP), especially highlighting more severe cystocele in those with DU [18]. Moreover, another study reported that DU was present in approximately half of women undergoing urodynamic evaluation for symptomatic POP, with the likelihood of DU diagnosis increasing substantially at advanced POP stages (stage 4) [18]. Our findings demonstrated that rather mild-to-moderate prolapse (POP-Q < 3) might indicate impaired detrusor function rather than BOO.
UFL has also been extensively studied as a non-invasive diagnostic method to distinguish different types of VD among patients with LUTS. Cheng et al. identified key UFL parameters—Qmax, flow time, and voiding efficiency—as independent risk factors for female BOO in women undergoing UDS; however, they did not explicitly evaluate DU patients [19]. Another study specifically examining DU predictors highlighted prolonged time to Qmax (greater than 13.5 s), altered mean flow ratios, and extended overall flow times as indicators of detrusor impairment, which align closely with our findings, though in a different patient population [20]. Furthermore, one study showed that among free-flow parameters, lower Qmax and higher bladder voiding efficiency were more predictive of BOO compared to DU in a multivariate regression analysis [21]. Our results complement these observations, reinforcing the concept that certain UFL-derived metrics, specifically the prolonged time to Qmax, can reliably support the differentiation between DU and BOO, particularly when interpreted within a structured diagnostic framework.
The diagnostic utility of flow-curve morphology remains more controversial. A recent 2020 study found that bell-shaped flow patterns effectively excluded BOO, whereas prolonged curves primarily indicated obstruction rather than DU. Fluctuating and intermittent curves were associated equally with both conditions, thereby limiting their diagnostic utility for clearly distinguishing between DU and BOO [22]. Another analysis indicated that prolonged or tailed curves were independent predictors for BOO when differentiating from DU or undetermined urodynamic findings (unclassified PFS) [23]. In contrast, in our current study, flow-curve shape did not emerge as a significant differentiating predictor, possibly due to the relatively limited sample size. Surprisingly, and in contrast with previous studies [2,19,24], patient age was not found to be a significant predictor of DU in our cohort. While age-related decline in detrusor function is well documented, the relatively young median age of our population (median 56 years; IQR 42–64) may explain this discrepancy.
Our study has several limitations that must be acknowledged. First, as a retrospective study, it is inherently subject to selection bias. Second, the relatively small sample size (n = 88) may limit statistical power and increase the risk of model overfitting, particularly in the context of a multivariate model with four predictors. While the variables were selected based on both statistical thresholds and clinical plausibility, the robustness of the model remains uncertain due to the limited sample size. Third, the absence of external validation further restricts the generalizability of our findings. The model has not yet been tested in an independent cohort, which is essential to establish its clinical utility. We therefore consider this study to be a pilot investigation aimed at generating hypotheses and informing the design of future validation studies. Another limitation is the lack of data on menopausal status and hormonal therapy, both of which are known to influence detrusor function and LUTS in women. Although medication use (e.g., anticholinergics, alpha-blockers) was recorded, it was not adjusted for in the regression analysis due to heterogeneity and limited subgroup sizes. These unaccounted confounders may have affected the observed associations. Finally, the study population consisted entirely of patients from a single geographic region and ethnic background, which may limit the applicability of our findings to more diverse populations. Future research should focus on prospective validation in larger, multi-center cohorts with broader demographic representation and the incorporation of additional clinical variables to enhance diagnostic accuracy.
5. Conclusions
In summary, we developed a non-invasive prediction model that integrates easily available clinical parameters—hesitancy, incomplete emptying, POP-Q assessment, and time to Qmax on UFL—to assist in differentiating DU from BOO in female patients with LUTS. While many prior attempts at symptom-based or single-parameter differentiation proved insufficient, our combined approach shows promise in terms of diagnostic value and clinical applicability and may serve as a supportive diagnostic aid in selected patients. Future studies in larger and more diverse populations are warranted to prospectively validate and refine the model.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu C.J. Hsiao S.M. Wu P.C. Chang T.C. Chen C.H. Sheu B.C. Lin H.H. Prevalence and predictors of detrusor underactivity and bladder outlet obstruction in women with lower urinary tract symptoms Sci. Rep.2024142514110.1038/s 41598-024-76242-y 39448651 PMC 11502903 · doi ↗ · pubmed ↗
- 2Wu P. Hsiao S. Lin H. Age-specific prevalence, clinical and urodynamic findings of detrusor underactivity and bladder outlet obstruction in female voiding dysfunction Int. J. Gynecol. Obstet.202416779780310.1002/ijgo.1570538800864 · doi ↗ · pubmed ↗
- 3Kitta T. Wada N. Shinohara S. Hayashi N. Yamamura H. Yamamoto T. Takagi H. Hatakeyama T. Nagabuchi M. Morishita S. Validation of the area under the Watts factor curve during the voiding cycle as a novel parameter for diagnosing detrusor underactivity in females Int. J. Urol.2024311121112710.1111/iju.1553138969345 · doi ↗ · pubmed ↗
- 4ICS Standards 2024 Available online: https://www.ics.org/Publications/ICS%20Standards%202024.pdf(accessed on 20 October 2024)
- 5Rosier P.F.W.M. Valdevenito J.P. Smith P. Sinha S. Speich J. Gammie A. Members of the ICS Working Group PFS 23 ICS-SUFU standard: Theory, terms, and recommendations for pressure-flow studies performance, analysis, and reporting. Part 1: Background theory and practice Neurourol. Urodyn.2023421590160210.1002/nau.2519237096828 · doi ↗ · pubmed ↗
- 6Rosier P.F.W.M. Gammie A. Valdevenito J.P. Speich J. Smith P. Sinha S. ICS-SUFU standard: Theory, terms, and recommendations for pressure-flow studies performance, analysis, and reporting, Part 2: Analysis of PFS, reporting, and diagnosis Continence 2023710070910.1016/j.cont.2023.10070937139677 · doi ↗ · pubmed ↗
- 7Valentini F.A. Marti B.G. Robain G. Zimern P.E. Nelson P.P. Comparison of indices allowing an evaluation of detrusor contractility in women Progrès Urol.20203039640110.1016/j.purol.2019.11.00431866143 · doi ↗ · pubmed ↗
- 8Lindsay J. Solomon E. Nadeem M. Pakzad M. Hamid R. Ockrim J. Greenwell T. Treatment validation of the Solomon-Greenwell nomogram for female bladder outlet obstruction Neurourol. Urodyn.2020391371137710.1002/nau.2434732249980 · doi ↗ · pubmed ↗