Assessing mutation-clinical correlations and treatment outcomes in Vietnamese non-small cell lung cancer patients
Hoang-Bac Nguyen, Bang-Suong Nguyen-Thi, Huu-Huy Nguyen, Minh-Khoi Le, Quoc-Trung Lam, Tuan-Anh Nguyen

TL;DR
This study analyzes genetic mutations and treatment outcomes in Vietnamese non-small cell lung cancer patients to guide personalized therapies.
Contribution
The study identifies mutation patterns and their clinical correlations in a Vietnamese NSCLC cohort, emphasizing EGFR and KRAS mutations.
Findings
EGFR mutations are more common in female non-smokers, while KRAS mutations are more common in male smokers.
EGFR-mutated patients treated with TKIs had significantly longer survival compared to others.
Co-mutations are rare and may indicate resistance to treatment.
Abstract
This study examines the genetic and clinical profiles of Vietnamese patients with non-small cell lung cancer (NSCLC), focusing on mutations in seven driver genes: EGFR, KRAS, NRAS, BRAF, ALK, ROS1, and PIK3CA. The goal is to identify mutation patterns and their correlations with clinical factors, thereby informing personalized treatment strategies. A cross-sectional study of 299 NSCLC patients at the University Medical Center, Ho Chi Minh City (2019–2022) recorded demographics, smoking history, and tumor stage. Pre-treatment samples were analyzed via massively parallel sequencing, and survival analysis assessed the impact of EGFR/KRAS mutations on survival and TKI response. Most patients (88.6 %) were diagnosed at stage IV. EGFR mutations were found in 43.5 % of cases, predominantly in female non-smokers, while KRAS mutations (15.4 %) were more common in male smokers. EGFR exon 19…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
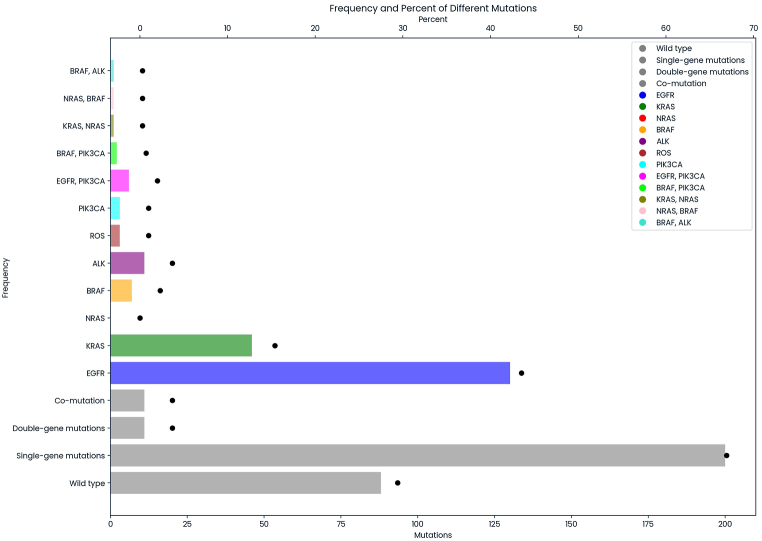 Figure 1
Figure 1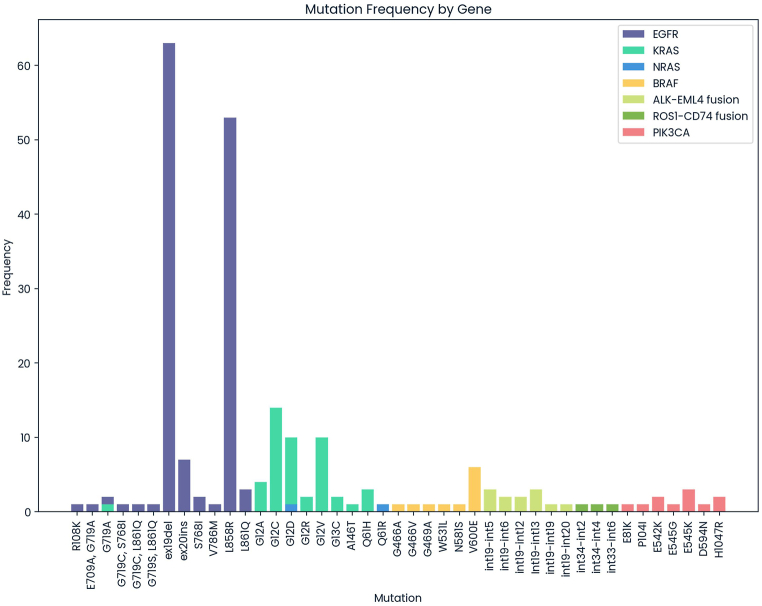 Figure 2
Figure 2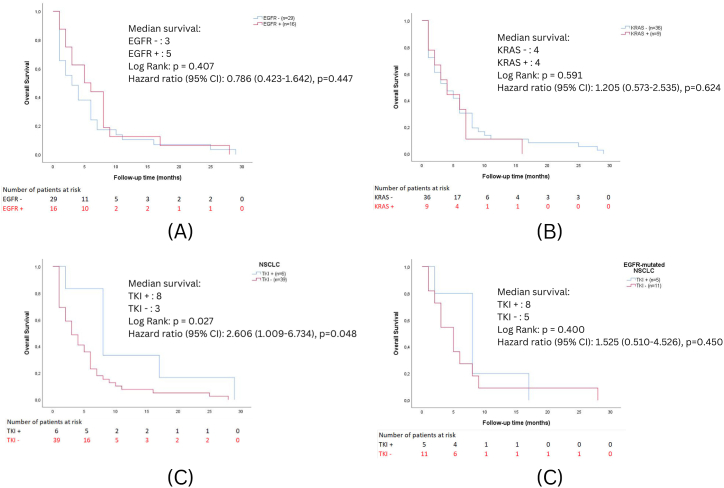 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Cancer Genomics and Diagnostics · Genetic factors in colorectal cancer
Introduction
1
Lung cancer remains the leading cause of mortality, accounting for an estimated 1.8 million deaths, which constituted 18 % of all cancer-related deaths [1]. In Vietnam, approximately 26,000 cases of lung cancer are reported annually, and sadly, around 24,000 of these cases result in fatalities [2]. Consequently, lung cancer stands as the second deadliest disease in the nation, demanding urgent medical attention. The two most common subtypes of lung cancer are small-cell lung carcinoma (SCLC), comprising 20 % of cases, and non-small-cell lung carcinoma (NSCLC), accounting for 80 % of cases [3]. NSCLC has been further categorized into three distinct subtypes: squamous-cell carcinoma, adenocarcinoma, and large-cell carcinoma [4].
Overall, patients with late-stage NSCLC are typically treated with systemic or palliative therapies, such as chemotherapy, radiation therapy, or a combination of both. The 5-year overall survival rates for NSCLC vary based on the stage of the cancer: 26 % for stage IIIb, 10 % for stage IVa, and 1 % for stage IVb [5]. Roughly 80 % of lung cancer patients are diagnosed at an advanced stage, where surgery offers little significant benefit [6]. Previously, patients with advanced stages of NSCLC were often considered less responsive to effective treatments due to poor prognoses. However, advancements in science and technology have enabled the identification of specific gene mutations and the use of targeted medications for treatment. Targeted therapy, which focuses on specific molecular pathways, has emerged as a promising approach. However, its effectiveness hinges on accurately identifying lung cancer cells, with oncogenic driver genes playing a pivotal role [7]. According to the National Comprehensive Cancer Network Guidelines for NSCLC (version 4.2020), it is recommended that all patients with advanced non-squamous NSCLC undergo testing for crucial driver genes, including EGFR, ALK, BRAF, and ROS1, regardless of clinical variables [8].
Most data available in publicly accessible databases, such as The Cancer Genome Atlas, come from prospective studies conducted in Caucasian cohorts. As a result, there is a high likelihood of underestimating the impact of NSCLC variations across different nations. GLOBOCAN statistics indicate that despite similar mortality rates, the incidence of lung cancer is significantly higher in Vietnam (14.5 %) compared to the global average (11 %) [9].
In our recent research, conducted at the prestigious University Medical Center in Southern Vietnam, we successfully utilized the "next generation sequencing" technique to identify genetic alterations in seven essential driver genes - EGFR, KRAS, NRAS, BRAF, ALK, ROS1, and PIK3CA - in tumor tissues from 299 cases of NSCLC. To our knowledge, this is one of the largest cohorts of NSCLC patients in Vietnam analyzed for seven major driver gene mutations. Moreover, Southeast Asian populations are underrepresented in global mutation profiling studies; our study helps fill this gap. Our analysis also revealed strong correlations between the occurrence of these mutations and various clinical characteristics within the Vietnamese cohort. Furthermore, we thoroughly evaluated current treatment methods for NSCLC. Additionally, we have been monitoring the survival rates of lung cancer patients who have received specialized therapy for one year, and our statistics have revealed some significant findings.
Materials and methods
2
Study design
2.1
Throughout every procedure, we meticulously adhered to applicable instructions and proper regulations. A total of 299 formalin-fixed paraffin-embedded tumor samples from NSCLC patients under the care of the University Medical Center were comprehensively examined. Hematoxylin and eosin staining were employed to identify tissue regions containing at least 20 % tumor cells. Before participation, each research participant provided their full consent. Testing for gene mutations was carried out only with explicit permission from the patient or their family, and all data collected was encrypted to safeguard patient privacy.
Treatment history of patients
2.2
Establishing a baseline genomic profile before treatment is crucial to accurately assess mutation patterns without interference from therapy-induced resistance. Genetic profiling before treatment was administered to the patients, ranging from first-line chemotherapy and radiation to advanced targeted therapies, such as osimertinib (n = 42), ceritinib (n = 5), pembrolizumab (n = 1), and bevacizumab-afatinib (n = 2). At the time of genomic analysis, patients had not received any therapy. Treatment regimens were later documented based on patient medical records from the University Medical Center in Ho Chi Minh City.
DNA isolation
2.3
We employed two different techniques to extract DNA from formalin-fixed paraffin-embedded specimens and quantify them: the QIAamp DNA FFPE Tissue Kit (Qiagen, USA) and the QuantiFluor dsDNA system (Promega, USA).
Massively parallel sequencing
2.4
We utilized NEBNext® UltraTM II kits from New England Biolabs, USA, to generate high-quality libraries from various input quantities and fragmentize DNA. We employed the QuantiFluor dsDNA system from Promega, USA, to measure DNA library concentrations. The seven driver genes EGFR (ID: 1956), KRAS (ID: 3845), NRAS (ID: 4893), BRAF (ID: 673), ALK (ID: 238), ROS1 (ID: 238), and PIK3CA (ID: 5290) were hybridized with xGen Lockdown probes obtained from IDT DNA, USA, with an equal amount of 150 ng for each sample library. Customized probes for intron regions of ALK and ROS1 were created and combined with exon region probes at an equal concentration. Sequencing was performed using the NextSeq system from Illumina, explicitly utilizing the 500/550 High Output kits Version 2 (150 cycles). Illumina's 550 system was used, aiming for a minimum target coverage of 100x. In cases where the mean coverage in the targeted areas fell below 100x, additional sequencing was conducted to raise the mean coverage to the anticipated range. Across all samples, the average coverage in the target regions was approximately 129x.
Variant calling using Mutect2 and Factera
2.5
Dual indicators in the P7 and P5 primers were used to barcode each FFPE specimen. The Bcl2fastq package from Illumina was employed to generate paired-end (PE) reads, which were subsequently aligned to the hg38 reference genome using the BWA package [10]. Duplicate reads were identified and labeled using the MarkDuplicates tool from the Picard program (http://broadinstitute.github.io/picard/) or the Mutect2 package [11]. Furthermore, a custom pipeline incorporating the BWA, Picard, and Samtools programs was developed to facilitate these analytical stages [12]. Factera v1.4.4 was utilized with standard settings to detect fusion variants to identify ALK and ROS1 rearrangements [13]. Our targeted capture sequencing method accurately identified mutations in FFPE tissue samples with a variant allele frequency (VAF) greater than 4 % [14]. Each gene investigates different types of mutations, including point mutations, deletions, and short insertions (under 20 nucleotides) in the coding region and adjacent areas near the intron (−20/+10 nucleotides from the exon) as follows: L858 (R, Q)/L861 (P, Q, R)/G719 (A, D, S, C, R, X)/S768I/L747S/A750P/Exon 19 deletion/Exon 20 insertion/T790M for EGFR, G12 (A, D, V) or G12 (S, R, C)/G13 (A, D, V) or G13 (S, R, C)/Q61 (K, E, P, L, R, H) or KRAS, G12 (A, D, V) or G12 (S, R, C)/G13 (A, D, V) or G13 (S, R, C)/Q61 (K, E, P, L, R, H) for NRAS, V600E for BRAF, ALK-EML4 fusion, ALK-HIP1, PHACTR1 fusion, G1202R for ALK, CD74, SLC34A2, SDC4, EZR, TPM3, Fig. 1, LRIG3, CCDC6, KDELR2, LRIG3, TPD52L1 fusions for ROS1, H1047 (R, L) and E545K for PIK3CA.Fig. 1. The genetic variation within seven crucial driver genes among 299 Vietnamese NSCLC patients. The bars represent frequencies. The dots represent the percent.Fig. 1
Statistical analysis
2.6
Descriptive statistics were used for categorical variables (frequencies and percentages). Statistical analysis using either the Chi-squared test (for sample sizes >5) or Fisher's exact test (for sample sizes ≤5) was employed to determine the p-value. The Monte Carlo simulation for larger tables with minor frequencies. Univariate and multivariate analyses assessed the association between clinical characteristics and the frequency of mutations in NSCLC driver genes, especially EGFR and KRAS mutations. The survival analysis includes three main aspects. First, the Kaplan-Meier analysis assessed survival outcomes of EGFR and KRAS mutation status and tyrosine kinase inhibitor treatment. Second, the log-rank test was conducted to determine whether survival distributions differed between groups. Finally, the Cox proportional hazards model was used to identify factors influencing survival time. A p-value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS 26 software.
Results
3
Patient characteristics
3.1
Our study involves a larger cohort with 299 patients compared to previous local studies, such as those by Dang et al. [14]. This provides a more robust data set for analyzing mutation patterns and their implications for treatment outcomes. Moreover, our research utilizes massively parallel sequencing to identify mutations, offering detailed and extensive genetic profiling compared to Vu et al. [15], which employed Sanger sequencing, a less comprehensive method in mutation detection.
The study cohort includes slightly more males (54.8 %) than females (45.2 %). The population is relatively evenly distributed across age groups, with fewer individuals over 61 (55.9 %) than those aged 61 or younger (44.1 %). A significant portion of the population has unknown smoking (21.4 %) and drinking habits (46.1 %). Adenocarcinoma (AC) is the most common histological type (93.3 %), followed by Squamous Cell Carcinoma (SCC) at 5.0 %. The majority of patients are diagnosed at stage IV (88.6 %). A total of 52.5 % of patients are treatment-naïve (Table 1).Table 1. Key clinical and pathological characteristics observed in 299 Vietnamese patients with NSCLC.Table 1. Clinical characteristicsN%GenderFemale13545.2Male16454.8Age≤6113244.1>6116755.9Smoking statusYes8127.1No15451.5Unknown6421.4Drinking habitsYes3712.4No12441.5Unknown13846.1HistologyAC27993.3SCC155.0Others or unknown51.7Tumor StageII144.7III206.7IV26588.6Treatment informationChemotherapy4113.7Naïve to treatment15752.5Palliative care3712.4Radiation41.3Resection103.3TKI5016.7N: number of cases; AC: adenocarcinoma; SCC: squamous cell carcinoma.
Mutation frequencies and co-mutations in NSCLC driver genes
3.2
The analysis of the occurrence of wild-type and mutated genes within the studied population presents the frequency of mutations across the seven primary driver genes and the specific mutation frequency in cases where co-mutations are observed.
Most patients exhibit mutations, with 66.9 % having mutations in a single gene and 3.7 % showing co-occurring mutations. Only 29.4 % of patients are wild-type. EGFR mutation is the most prevalent in 43.5 % of patients, while KRAS is detected in 15.4 %. In a minority of cases, concurrent mutations, where patients have mutations in more than one gene, were detected in various gene combinations. Specifically, EGFR and PIK3CA co-mutations were observed in 2.0 % of cases, while co-mutations involving BRAF and PIK3CA occurred in 0.7 % of cases. Moreover, KRAS and NRAS co-mutations were identified in 0.3 % of cases, with NRAS and BRAF co-mutations occurring at the same frequency. Co-mutations involving BRAF and ALK were also observed in 0.3 % of cases (Fig. 1).
The study population exhibited a variety of EGFR mutations, ranging from point mutations to insertions and deletions. Exon 19 deletions (46.3 %) and the L858R mutation (39.0 %) were the most prevalent. Less common mutations included exon 20 insertions (5.1 %) and co-mutations. The frequency and distribution of KRAS mutations in the study population revealed a diverse array of mutations across various codons, with G12C (29.8 %), G12D (21.3 %), and G12V (21.3 %) being the most frequent. Rarer mutations, such as G12A, G12R, G13C, A146T, G719A, and Q61H, contributed to the molecular diversity of KRAS-mutant cancers. Two NRAS mutations, G12D and Q61R, accounted for 50 % of observed mutations. The predominant BRAF mutation was V600E, accounting for 54.5 % of BRAF mutations, while other mutations, including G466A, G466V, G469A, W531L, and N581S, each represented 9.1 %. The most common ALK-EML4 fusion variants were int19-int5 and int19-int13, each at 25.0 %, followed by int19-int6 and int19-int12, at 16.7 % each. Int19-int19 and int19-int20 were less frequent, at 8.3 % each. ROS1-CD74 fusion variants included int34-int2, int34-int4, and int33-int6, each representing 33.3 % of mutations. PIK3CA mutations encompassed variants like E81K, P104I, E542K, E545G, E545K, D594N, and H1047R. E545K (27.3 %) and H1047R (18.2 %) were the most common mutations, followed by E542K (18.2 %), and less frequent mutations, such as E81K, P104I, E545G, and D594N, each at 9.1 % (Fig. 2).Fig. 2. The distribution of mutation subtypes across seven driver genes, namely EGFR, KRAS, BRAF, NRAS, ALK, ROS1, and PIK3CA, was analyzed in Vietnamese NSCLC. The mutation frequencies (%) within specific subtypes of these genes were determined as the percentage of mutant cases among the total number of cases with mutations. The bars represent frequencies.Fig. 2
Associations between clinical characteristics and NSCLC driver gene mutations
3.3
Table 2 presents the distribution of clinical characteristics by mutation status for seven genes (EGFR, KRAS, NRAS, BRAF, ALK, ROS1, and PIK3CA), with p-values indicating statistical significance. For EGFR, mutations are significantly more common in females (60.7 % vs. 32.9 % in males; p < 0.001) and non-smokers (72.1 % vs. 29.6 % in smokers; p < 0.001). Moreover, non-drinkers tend to exhibit a higher prevalence of EGFR mutations (53.2 %) compared to drinkers (35.1 %), although this difference is marginally significant (p = 0.053). In contrast, KRAS mutations are significantly more prevalent in males (23.8 % vs. 5.9 % in females; p < 0.001) and smokers (44.4 % vs. 7.1 % in non-smokers; p < 0.001), with a significant association also observed with alcohol consumption (p = 0.001). ALK mutations are notably linked with female gender (6.7 % vs. 0.6 % in males; p = 0.041) and with younger patients (7.6 % in individuals ≤61 years vs. 1.2 % in those >61 years; p = 0.007), while differences by smoking and alcohol status are not significant. In addition, the prevalence of ROS1 mutations does not differ significantly by gender, age, smoking, or alcohol consumption. Similarly, mutations in NRAS, BRAF, and PIK3CA show no significant associations with these clinical parameters. Analyses by histologic subtype and tumor stage also reveal no significant correlations with mutation status across the examined genes, except for treatment groups, where significant differences were observed for EGFR and KRAS (p < 0.001). Collectively, these results underscore that while specific clinical factors such as gender, age, smoking, and alcohol consumption are robustly associated with the prevalence of mutations in EGFR, KRAS, and ALK, they do not appear to influence the mutation status of NRAS, BRAF, ROS1, or PIK3CA.Table 2. The correlation between clinical variables and the occurrence rates of mutations in NSCLC driver genes.Table 2. Clinical characteristicsEGFRKRASNRASBRAFALKROS1PIK3CAYesNopYesNopYesNopYesNopYesNopYesNopYesNopGenderFemale8253<0.0018127<0.00101350.50341310.75991260.04121330.59151300.984Male541103912521637157316111636158Age≤6163690.489221100.68911311.00041280.760101220.00721300.58541280.760>6173942514211667160216511667160Smoking statusYes2457<0.0013645<0.0012790.1181800.6621800.1690811.0003781.000No111431114301544150814611537147Unknown163064064658361262163Alcohol drinkingYes13240.05314230.0012350.0521361.0000370.1200371.0002351.000No66581710701244120911511237117Unknown57811612201386132313521362136HistologyACC1301490.315442350.48212780.10092700.413122671.00032761.000102690.444SCC510114114114015015114Unknown14230514050505Tumor stageII1040.0562120.9250141.0000140.5010140.5050141.0000140.238III614416020020020020218IV120145412242263112541225332629256Treatment16790<0.00121136<0.00111560.10281490.28861510.45411560.35221550.16327341724041338041140338314235320370373341361364132204040404045462819010010010196437050050050347050446The abbreviations ACC and SCC represent adenocarcinoma and squamous carcinoma, respectively. Tumor stage: II, III, IV. Treatment: 1, 2, 3, 4, 5, and 6 are naïve to treatment, chemotherapy, palliative care, radiation, resection, and TKI, respectively.
To assess the potential influence of prior treatments on genomic alterations, we performed subgroup analyses stratifying patients by their treatment histories. This analysis aimed to identify any significant patterns of mutations associated with specific therapies, with a primary focus on secondary resistance mutations in the EGFR and KRAS genes (Table 3) (see Table 4).Table 3. The frequency of specific mutations stratified by treatment type.Table 3. Treatment informationChemotherapyNaïve to treatmentPalliative careRadiationResectionTKINone125414134EGFR ex19del12781221EGFR L858R3273–216KRAS G12C581–––KRAS G12D3511––EGFR Exon20ins14–––1BRAF V600E–4––––KRAS G12A–4––––KRAS g12v523–––KRAS Q61H12––––ALK-EML4 (int19-int6)–2––––ALK-EML4 fusion (int19-int13)–2––––EGFR S768I–2––––EGFR G719A–1–––1PIK3CA D594N–1––––ROS1-CD74 fusion (int34-int4)–1––––ALK-EML4 fusion (int19-int20)–1––––BRAF G466V–1––––BRAF N581S–1––––BRAF W531L, ALK-EML4 fusion (int19-int13)–1––––NRAS G12D, BRAF G469A–1––––EGFR Exon20ins, PIK3CA E545G–1––––EGFR G719A, E709A–1––––EGFR G719C, S768I–1––––EGFR G719S; L861Q–1––––EGFR L861Q, G719C–1––––EGFR R108K–1––––ALK-EML4 fusion (int19-int5)––2––1ALK-EML4 fusion (int19-int12)––1––1ALK-EML4 fusion (int19-int19)–––––1EGFR ex19del, PIK3CA E545K–––––1EGFR ex19del, PIK3CA H1047R–––––1EGFR L858R, PIK3CA H1047R–––––1EGFR L858R, PIK3CA p104l–––––1KRAS g12r–––11–PIK3CA E542K––––1–KRAS G13C, NRAS Q61R––––1–EGFR L861Q1–2–––ROS1-CD74 (int33-int6)––1–––EGFR ex19del, PIK3CA E81K––1–––PIK3CA E545K1–––––ROS1-CD74 (int34-int2)1–––––BRAF G466A1–––––BRAF V600E, PIK3CA E542K1–––––BRAF V600E, PIK3CA E545K1–––––KRAS A146t1–––––KRAS G13C1–––––KRAS G719A1–––––EGFR V786M1–––––None: No mutation in the penal was detected. Int: insertion. (−) no mutation exists. The number represents the frequency of specific mutations.Table 4. Logistic regression analysis of clinical factors associated with EGFR and KRAS mutation status.Table 4. Clinical characteristicsEGFRKRASpOR95 % CIpOR95 % CIGender0.6070.7650.276–2.1250.0753.7970.875–16.47Age0.8350.9170.406–2.0710.2731.9000.603–5.987Smoking status0.1280.3990.122–1.3040.0844.0200.830–19.47Alcohol drinking0.8951.0870.314–3.7680.8920.8920.190–4.180Histology0.2990.4230.083–2.146–––Tumor stage III0.02111.071.443–84.860.1010.1060.007–1.543Tumor stage IV0.6011.5360.308–7.6550.1910.2810.042–1.881Chemotherapy0.0040.1630.048–0.5590.0048.5362.003–36.38Palliative care0.2130.4980.166–1.4920.4961.6910.372–7.681Radiation0.5570.4480.031–6.5380.02943.771.466–1307Resection0.6320.6510.113–3.7600.7240.6180.043–8.949Tyrosine Kinase Inhibitor0.0017.3003.378–22.40–––OR: Odds ratio; Reference categories: Tumor stage II, Naïve to treatment.
Patients with different genetic mutations received varying treatments, which included chemotherapy, naive to treatment, palliative care, radiation, resection, and targeted kinase inhibitors (TKIs). Patients whose testing panel detects no mutation may undergo various interventions, likely based on other clinical factors outside the detected gene mutations.
EGFR mutations, such as ex19del and L858R, are associated with a higher proportion of patients receiving TKI treatments (21 % and 16 %, respectively), which aligns with the finding that EGFR mutations often respond well to TKIs. These mutations are also notable in patients receiving chemotherapy and those considered naive to treatment, indicating the prevalence and importance of these mutations in treatment decisions. KRAS mutations, such as G12C and G12D, exhibit lower rates of receiving TKIs, consistent with KRAS mutations typically associated with poorer outcomes and reduced responsiveness to TKIs. Many patients with various mutations are treatment-naive, which could reflect newly diagnosed cases or those waiting to begin a treatment regimen. Some mutations with complex or multiple genetic alterations, such as EGFR Exon20ins and PIK3CA E545G, are found in very few patients, often only one or two, suggesting that these are rare or less commonly targeted for specific treatments. Palliative care numbers are generally low, which might indicate either a lower rate of end-stage patients in this dataset or a focus on more aggressive treatment strategies in this particular clinical setting.
Logistic regression analysis of clinical factors influencing EGFR and KRAS mutations
3.4
In this study on EGFR mutation status, significant findings include that Stage III patients are significantly more likely to exhibit positive EGFR mutations with an odds ratio (OR) of 11.07 (p = 0.021), suggesting advanced cancers are more mutation-prone. There is a notable negative correlation between chemotherapy and EGFR mutations (OR = 0.163, p = 0.004), indicating that chemotherapy is more often prescribed to patients without these mutations. This is likely because patients with mutations are prioritized for other treatments, such as tyrosine kinase inhibitors (TKIs). TKIs exhibit a strong positive association with EGFR mutations (OR = 7.3, p = 0.001), confirming that patients with these mutations are significantly more likely to receive TKI treatment. Other clinical factors like gender, age, smoking, and alcohol consumption did not demonstrate a significant relationship with EGFR mutation status (p > 0.05), highlighting that the most important predictors of mutation status are cancer stage and treatment type.
In the analysis of KRAS mutation status, the results demonstrate statistically significant associations for patients undergoing chemotherapy (p = 0.004, OR = 8.536), indicating that they are approximately 8.5 times more likely to have a positive KRAS mutation than the naive-to-treatment group. This pattern suggests that KRAS mutation carriers, who typically respond poorly to TKI intended for EGFR/ALK-positive cancers, often receive chemotherapy or radiation. Radiation treatment also shows a strong positive correlation with KRAS mutations (p = 0.029, OR = 43.77), though the wide confidence interval suggests a small or unevenly distributed sample. This indicates that patients with KRAS mutations are significantly more likely to require radiation, either as a supplementary treatment or for symptom relief. Other variables such as gender, age, smoking, and tumor stage did not show significant results (p > 0.05), although trends indicate that KRAS mutations are more prevalent among males and smokers. The negligible response of KRAS mutation-positive patients to TKIs is also highlighted, suggesting a minimal use of TKIs in this group. Overall, the significant links between chemotherapy, radiation, and KRAS mutations align with the biological behavior of KRAS-mutant lung cancer, underlining the necessity for alternative treatments like chemotherapy and radiation in these patients.
Survival analysis by EGFR and KRAS mutation status and TKI treatment
3.5
In the analysis stratified by EGFR status (n = 45), the median survival was 3 months for the EGFR‐negative group and 5 months for the EGFR‐positive group. Still, this difference was not statistically significant (p = 0.407) by either the log-rank test or Cox regression (HR = 0.786, p = 0.447). A similar pattern was observed when stratifying by KRAS status: 45 patients were included, and both the KRAS‐negative and KRAS‐positive groups had a median survival of four months, with no significant difference in survival (p = 0.591) and an HR of 1.205 (p = 0.624). In contrast, when comparing TKI recipients (n = 6) with non‐TKI recipients (n = 39), the Kaplan-Meier analysis showed a significantly longer median survival for the TKI group (8 vs. 3 months, p = 0.027). However, the Cox model yielded a hazard ratio of 2.606 (p = 0.048), which may be attributed to confounding factors such as disease severity or the small sample size. Focusing specifically on the 16 EGFR‐mutated NSCLC patients, the Cox regression indicated a hazard ratio of 1.525 (p = 0.450) for TKI use, a finding that was not statistically significant. The wide confidence interval (0.510–4.562) and small sample underscore the limited power of this subgroup analysis. Overall, the unadjusted Kaplan–Meier results for TKI use in the entire 45-patient cohort suggest a survival benefit. In contrast, the hazard ratio and smaller subgroup analysis raise questions that require cautious interpretation (Fig. 3).Fig. 3. Overall survival varies according to EGFR (5A) and KRAS (5B) mutation status and EGFR tyrosine kinase inhibitors (TKI) treatment in NSCLC (5C) and EGFR-mutated NSCLC (5D) patients.Fig. 3
Discussion
4
Establishing a solid genetic predisposition to lung cancer could be clinically valuable for stratifying populations for effective treatment and primary prevention. Our study provides detailed insights into the prevalence and types of mutations across various demographic groups, including age, smoking status, and gender, offering valuable data for personalized medicine in the treatment of NSCLC. We identified significant correlations between the presence of EGFR, KRAS, and ALK mutations and clinical characteristics such as gender, age, smoking habits, and alcohol consumption in the Vietnamese cohort. Additionally, we assessed the effectiveness of current NSCLC treatments and monitored the survival rates of lung cancer patients after one year of specialized therapy. To the best of our knowledge, this represents one of the most extensive Vietnamese NSCLC cohorts examined for seven primary driver mutations. Furthermore, given the limited representation of Southeast Asian populations in global genomic studies, our research provides important insights to help bridge this disparity.
Among 299 Vietnamese NSCLC patients, the majority (88.6 %) presented with advanced disease at the time of diagnosis. Adenocarcinoma was the most common histological type, accounting for 93.3 % of cases. Additionally, more than 50 % of patients reported not receiving specific therapy for their condition. However, some patients with stage II NSCLC were enrolled and received targeted therapy if they had gene mutations. This is a common scenario in our hospital's clinical setting, as physicians often recommend TKIs as adjuvant therapy following complete surgical resection for stage II patients, mainly when specific genetic mutations are present. This approach is generally considered when patients have the financial resources to afford TKI therapy, given that healthcare reimbursement for these treatments is often limited.
Furthermore, as mentioned in our study, the decision to forgo targeted therapy for some patients often arises from financial constraints or deteriorating health. In such cases, palliative care may be deemed a more suitable option. These factors significantly impact clinical decision-making, highlighting the need for a personalized approach. These data provide valuable insights into the demographics, disease characteristics, and treatment landscape of the study population.
Actionable genomic insights in Vietnamese NSCLC
4.1
We employed targeted next-generation sequencing to analyze seven actionable driver genes - EGFR, KRAS, NRAS, BRAF, ALK, ROS1, and PIK3CA - in formalin-fixed, paraffin-embedded tumor specimens from Vietnamese NSCLC patients. This approach is more comprehensive than earlier studies, which focused primarily on EGFR [15,16]. Our findings confirmed EGFR as the most prevalent mutation, aligning with previous research [14,[17], [18], [19], [20]], while KRAS emerged as the second most frequent [14,19,21]. These results underscore the global impact of racial, genetic, and environmental factors on mutation variability [17,18].
Recent investigations into the mutation spectrum of NSCLC have highlighted notable ethnic and regional variations, particularly in the incidence of EGFR and KRAS mutations. In our cohort, the EGFR mutation rate reached 43.5 %, aligning with findings in other East Asian populations - such as China (30–50 %) [22] and Japan (around 43.6 %) [23] - but substantially exceeding the figures reported in Caucasian (9.8–17.5 %) [24,25] and African-American groups (4.8–19 %) [26,27] (Table 5). These higher EGFR frequencies among Vietnamese and other East Asians suggest a strong influence from genetic predisposition, lifestyle, and environmental factors unique to these regions. Smoking habits may play an additional role, as reduced smoking prevalence or patterns could partially explain the relatively high occurrence of EGFR mutations in these populations.Table 5EGFR and KRAS mutation frequencies in NSCLC by ethnicity and region.Table 5. Study populationEGFR mutation (%)KRAS mutation (%)SourceVietnamese43.515.4This studyOther Vietnamese35.0–35.422.6–23.0[2,14]Chinese30.0–50.08.3[22,52]Japanese43.69.3[23]Korean17.4–51.35.2–5.8[[53], [54], [55]]Caucasian9.8–17.523.0–35.0[24,25,28]African-American4.8–19.017.0–25.0[26,27]
In contrast, KRAS mutations were observed in 15.4 % of our study cohort, which is significantly lower than the 23–35 % (Table 5) found in Western cohorts [24,28]. This trend reflects an inverse relationship between EGFR and KRAS mutations. While patients in East Asian countries generally exhibit elevated EGFR mutation rates, they tend to have fewer KRAS mutations compared to Western populations. Nonetheless, some variation exists even within Vietnam itself. Compared to two prior studies in the same country [2,14], EGFR mutation rates in this cohort were higher, whereas KRAS frequencies were lower (Table 5). Such discrepancies suggest that factors such as local environment, healthcare infrastructure, and genetic diversity within an ethnic group may substantially influence the prevalence and detection of specific mutations.
These findings underscore the importance of establishing ethnic-specific genomic databases and treatment guidelines, which are vital for ensuring equitable access to precision medicine. Routine molecular profiling of NSCLC tumors helps clinicians identify actionable mutations, thereby informing targeted therapies. Asian patients, who often have higher EGFR mutation rates, frequently benefit from EGFR tyrosine kinase inhibitors, a mainstay treatment in regions such as Vietnam, China, Japan, and Korea. Conversely, Western patients who show an elevated incidence of KRAS mutations may require alternative therapeutic approaches. Novel agents targeting KRAS G12C, for example, offer promising avenues for patients harboring KRAS mutations; however, they remain under investigation and are not as commonly indicated for East Asian populations.
Recognizing these molecular distinctions is crucial for optimizing care in NSCLC, highlighting the need for personalized screening, prevention, and therapeutic strategies. By accounting for genetic, environmental, and lifestyle factors, clinicians can better identify which treatments are most likely to be effective for specific patient populations. In an era where personalized medicine is increasingly driving oncology research, documenting ethnic and regional differences offers a roadmap to expand the benefits of targeted therapies worldwide.
Further analysis revealed that EGFR mutations were notably higher in female non-smokers, consistent with established correlations between EGFR, gender, and smoking status [14,18,19,29]. Meanwhile, KRAS mutations were more common among smokers, reflecting the strong link between cigarette smoking and KRAS alterations [14,24,30,31]. These observations advance our understanding of the molecular landscape of Vietnamese NSCLC, emphasizing the importance of actionable genomic profiling in guiding personalized therapies and informing future targeted research.
Comprehensive analysis of key oncogenic mutations in NSCLC
4.2
Identifying diverse oncogenic drivers underscores the complexity of NSCLC and highlights the need for comprehensive genomic profiling to guide personalized treatment [32]. Common EGFR mutations (e.g., ex19del and L858R) correlate strongly with favorable responses to inhibitors like gefitinib and erlotinib [15]. By contrast, KRAS mutations (particularly G12C, G12D, and G12V) often predict poor prognosis and resistance to EGFR inhibitors, emphasizing the importance of alternative therapeutic strategies [33]. Notably, the emergence of KRAS G12C inhibitors - such as sotorasib and adagrasib - offers significant therapeutic potential; these agents are now approved for second-line use in advanced or metastatic NSCLC and highlight the importance of comprehensive molecular testing to guide therapy selection [34].
Although less frequent, NRAS mutations (∼1 %) share signaling pathways with KRAS, potentially conferring sensitivity to MEK inhibitors like selumetinib and trametinib [35]. BRAF mutations, including the well-characterized V600E variant, can be targeted with combined BRAF/MEK inhibition (dabrafenib plus trametinib), thereby improving treatment efficacy [36]. ALK-EML4 and ROS1-CD74 fusions also play critical roles in tumorigenesis, with established targeted options (e.g., crizotinib and newer ALK inhibitors) that significantly enhance patient outcomes [[37], [38], [39]]. Finally, PIK3CA mutations, such as E542K, E545K, and H1047R, underscore the relevance of the PI3K/AKT/mTOR pathway in NSCLC and hold promise for future targeted therapies [40,41]. Overall, these findings underscore the importance of routine biomarker testing, preferably via next-generation sequencing, and the integration of emerging treatments to address the molecular heterogeneity of NSCLC.
Distribution of driver mutations across lung cancer histological types
4.3
Lung cancers are primarily classified as non-small cell lung cancer (NSCLC, ∼80 %) and small cell lung cancer (SCLC, ∼20 %) [3]. Our histological assessment identified EGFR and KRAS as predominant driver genes, consistent with a report showing at least eight pathological subtypes in lung adenocarcinoma [18]. Variations in smoking habits and racial backgrounds may explain the genetic disparities observed across histological groups [37], and most research indicates EGFR and KRAS mutations rarely coexist [38].
In this study, adenocarcinoma showed a higher frequency of mutations than squamous cell carcinoma or cancers of unknown histology [39]. The predominance of EGFR mutations in adenocarcinoma highlights its potential as a therapeutic target for EGFR inhibitors [40]. The absence of ALK and ROS1 rearrangements in squamous cell carcinoma suggests a lesser role for these fusions in that subtype. However, a rare case of lung squamous cell carcinoma with a ROS1 rearrangement showed marked sensitivity to crizotinib [41]. These findings underscore the need for comprehensive genomic profiling to guide personalized therapy.
Few mutations were observed in the unknown histology group, indicating a need for further classification to determine their clinical implications. Less common mutations, such as NRAS and PIK3CA, also warrant additional investigation in adenocarcinoma and squamous cell carcinoma, potentially through targeted clinical trials [42]. Ultimately, understanding the mutation landscape across different histological types can foster more effective, patient-specific treatment strategies [43].
Co-mutation profiles and the impact of targeted treatment
4.4
Co-mutation profiling is critical for designing targeted therapies that may address multiple mutations simultaneously. Our study observed a lower co-mutation rate (3.7 %) than another study reporting 12.3 % in stage IV disease [39]. Notably, co-mutations in EGFR and PIK3CA could reflect crosstalk between the EGFR and PI3K-AKT-mTOR pathways, potentially indicating poor prognosis in advanced EGFR-mutant lung adenocarcinomas [40,41]. Co-mutations in BRAF and PIK3CA may signify an aggressive phenotype, as both mutations correlate with poor outcomes in colorectal cancer [42,43]. Similarly, KRAS and NRAS co-mutations may activate overlapping downstream signaling pathways (e.g., RAF-MEK-ERK and MEK-ERK, respectively) [44,45], though their exact clinical impact remains unclear.
BRAF mutations are relatively rare in NSCLC (2.3 % of lung adenocarcinoma) and often appear in never-smokers [46]. Thus, NRAS-BRAF co-mutations are even rarer and may indicate complex tumor heterogeneity [47]. Some studies have reported co-mutations in BRAF and ALK [48], suggesting possible cross-regulation between the MAPK and ALK pathways. Although KRAS-EGFR co-mutations have been reported elsewhere, their incidence is less than 1 %, and none were identified in our cohort [49]. Overall, these patterns highlight the disease's molecular diversity and complexity. Further research is needed to clarify the clinical significance of these co-mutations and guide personalized treatment strategies.
Additionally, interpreting genomic data in patients with diverse treatment histories poses challenges, as prior therapies can induce secondary mutations like EGFR T790M. This study acknowledges that variability in treatment backgrounds limits the generalizability of findings. Future research with more uniform cohorts or statistical controls for prior treatments could better isolate the effects of specific genomic alterations on treatment response and disease progression. Notably, resistance mutations (e.g., secondary EGFR mutations) were more common in patients previously exposed to TKIs, underscoring the selective pressure exerted by targeted therapies [50,51].
Overall survival to EGFR and KRAS mutation status and tyrosine kinase inhibitor treatment
4.5
Unlike many studies [15,16], our approach extends beyond simple mutation detection to examine relationships with progression-free survival and overall outcomes in advanced-stage III and IV NSCLC. By correlating specific mutations with survival and treatment responses, we provide practical insights for personalized therapy - particularly relevant in Vietnam, where such detailed data have been scarce.
Our findings reveal that EGFR and KRAS mutations are correlated with declining cumulative survival (Fig. 3A and B). Although KRAS-mutant patients generally have lower survival rates than non-mutants, this difference is less pronounced than in EGFR-mutant cases. Consistent with previous observations, EGFR mutations are more common in older patients with worse survival [47]. Moreover, EGFR and KRAS independently affect outcomes in advanced NSCLC treated with EGFR-TKIs, with EGFR status influencing progression-free and overall survival. In contrast, KRAS status primarily affects overall survival [48].
Among all NSCLC patients in our study, those receiving TKI therapy showed higher mean and median survival times (Fig. 3C). However, in the EGFR-mutant subgroup, the TKI and non-TKI groups had similar survival curves (Fig. 3D), suggesting that EGFR mutations do not always predict TKI benefits [38]. This discrepancy could be attributed to geography, ethnicity, treatment practices [49], sample size, or patient demographics.
Despite these nuances, our results illuminate the impact of TKI therapy on Vietnamese patients with advanced NSCLC and lay the groundwork for future clinical trials of targeted therapies. Additional research is needed to clarify the efficacy of TKIs in EGFR-mutant patients, as evidenced by a recent study in China, which demonstrated significantly better survival among EGFR-TKI-treated patients [50]. Our analysis highlights the importance of genomic profiling and its correlation with survival in informing treatment decisions and enhancing cancer care in Vietnam.
Conclusion
5
The study reveals a high prevalence of advanced-stage adenocarcinoma in Vietnamese NSCLC patients. It identifies strong links between EGFR and KRAS mutations with factors such as gender and smoking status. EGFR mutations are predominantly found in female non-smokers, whereas KRAS mutations are more common among male smokers. The use of EGFR inhibitors as targeted therapies has demonstrated significant survival benefits, emphasizing the need for personalized treatment plans based on detailed genomic profiling. Additionally, the research highlights the intricate relationship between a patient's treatment history and genomic alterations, stressing the importance of careful analysis in determining the impact of previous treatments. This necessitates further studies to understand these interactions better and enhance personalized treatment approaches in NSCLC.
CRediT authorship contribution statement
Hoang-Bac Nguyen: Writing – review & editing, Supervision, Resources, Project administration, Investigation, Funding acquisition, Conceptualization. Bang-Suong Nguyen-Thi: Writing – original draft, Supervision, Resources, Project administration, Investigation, Funding acquisition, Conceptualization. Huu-Huy Nguyen: Visualization, Validation, Formal analysis. Minh-Khoi Le: Software, Methodology, Data curation. Quoc-Trung Lam: Software, Methodology, Formal analysis. Tuan-Anh Nguyen: Writing – review & editing, Writing – original draft, Visualization, Validation, Investigation, Formal analysis, Data curation.
Ethics approval and consent to participate
The University Medical Center Ho Chi Minh City ethics committees reviewed and approved this study protocol (reference number: 88/GCN-HĐĐĐ, signed on 29/09/2022). All procedures were conducted following relevant guidelines and regulations. Before the investigations, written informed consent was obtained from all participants and/or their legal guardians. This study adhered to the World Medical Association's Code of Ethics (Declaration of Helsinki) for human experiments.
Consent for publication
Not applicable.
Availability of data and materials
The detailed data and materials are available upon reasonable request ([email protected]).
Funding
The University Medical Center Ho Chi Minh City supported this work under Grant 92/2022/HĐ-ĐHYD. The funding agency had no role in the study's design, data collection, analysis, interpretation, or manuscript writing.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests:The authors declare no conflict of interest, financial or otherwise.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H.Ferlay J.Siegel R.L.Laversanne M.Soerjomataram I.Jemal A.Bray F.Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.713202120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Tran H.T.T.Nguyen S.Nguyen K.K.Pham D.X.Nguyen U.H.Le A.T.Nguyen G.H.Tran D.V.Phung S.D.H.Do H.M.Lung cancer in Vietnam J. Thorac. Oncol.16920211443144810.1016/j.jtho.2021.06.00234425998 · doi ↗ · pubmed ↗
- 3Nicholson A.G.Tsao M.S.Beasley M.B.Borczuk A.C.Brambilla E.Cooper W.A.Dacic S.Jain D.Kerr K.M.Lantuejoul S.The 2021 WHO classification of lung tumors: impact of advances since 2015 J. Thorac. Oncol.173202236238710.1016/j.jtho.2021.11.00334808341 · doi ↗ · pubmed ↗
- 4Pathological diagnosis and classification of lung cancer in small biopsies and cytology: strategic management of tissue for molecular testing Travis W.D.Rekhtman N.Seminars in Respiratory and Critical Care Medicine 2011© Thieme Medical Publishers 10.1055/s-0031-127286621500121 · doi ↗ · pubmed ↗
- 5Goldstraw P.Chansky K.Crowley J.Rami-Porta R.Asamura H.Eberhardt W.E.Nicholson A.G.Groome P.Mitchell A.Bolejack V.The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer J. Thorac. Oncol.111201639512676273810.1016/j.jtho.2015.09.009 · doi ↗ · pubmed ↗
- 6Rivera M.P.Mehta A.C.Wahidi M.M.Establishing the diagnosis of lung cancer: diagnosis and management of lung cancer: American College of Chest Physicians evidence-based clinical practice guidelines Chest (Am. Coll. Chest Physicians)14352013 e 142S-e 65S 10.1378/chest.12-235323649436 · doi ↗ · pubmed ↗
- 7Juan O.Popat S.Ablative therapy for oligometastatic non–small cell lung cancer Clin. Lung Cancer 18620175956062837720610.1016/j.cllc.2017.03.002 · doi ↗ · pubmed ↗
- 8N.C.C.N. [NCCN]Non-small cell lung cancer Version 3.2022 NCCN Clinical Practice Guidelines in Oncology J. Natl. Compr. Canc. Netw.20520224975303554517610.6004/jnccn.2022.0025 · doi ↗ · pubmed ↗