Drug-associated abdominal aortitis and retroperitoneal fibrosis after treatment with nivolumab
Naomi Wedel, Benjamin Wajda, Richard Cormack, Kenton Rommens

TL;DR
A patient treated with nivolumab developed rare side effects involving the aorta and retroperitoneal area, highlighting the need for awareness of such risks in cancer treatment.
Contribution
The paper reports a new case and reviews existing literature on immune checkpoint inhibitor-induced aortitis.
Findings
A 60-year-old man developed aortitis and retroperitoneal fibrosis after nivolumab treatment.
A literature search identified 19 additional cases of ICI-associated aortitis.
Optimal management strategies for ICI-induced aortitis remain unclear and require further study.
Abstract
A 60-year-old man with metastatic supraglottic laryngeal cancer treated with nivolumab, an immune checkpoint inhibitor (ICI), developed abdominal aortitis and retroperitoneal fibrosis. The nivolumab was discontinued and no steroids were initiated. A literature search found 19 other cases of ICI-associated aortitis. The evidence is limited and conflicting on the optimal management of these rare but serious adverse events. With increasing application in the treatment of a multitude of cancer types, physicians must remain aware of aortitis as an adverse event and consider the potential risks vs benefits before initiating ICI treatment for their patient.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
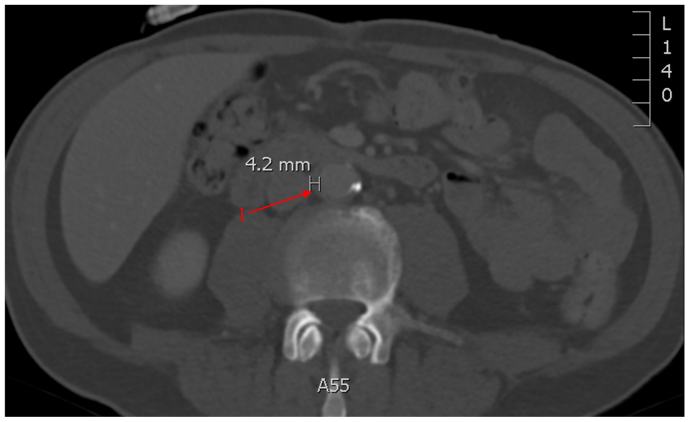 Figure 1
Figure 1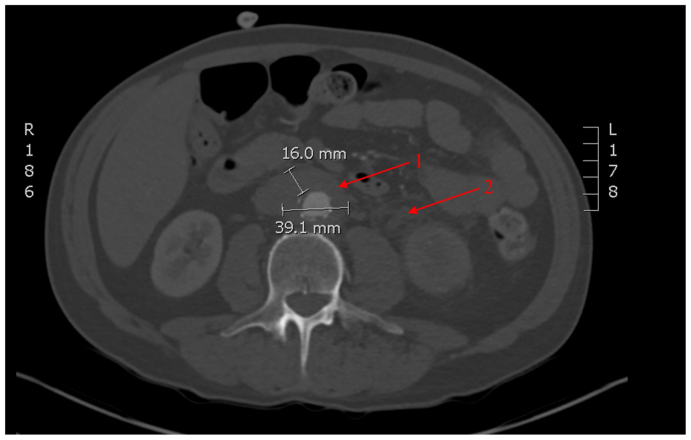 Figure 2
Figure 2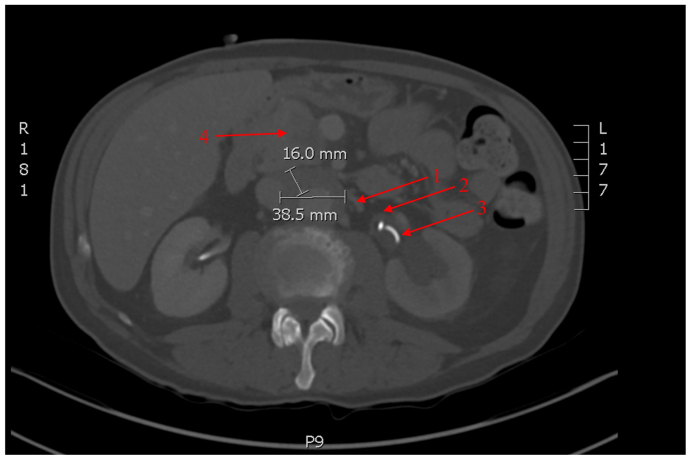 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Abdominal vascular conditions and treatments · Pancreatitis Pathology and Treatment
Immune checkpoint inhibitors (ICIs) are immunotherapy drugs for treatment of a variety of cancer types.1 These monoclonal antibodies inhibit immune checkpoint molecules to provide antitumor activity.2 Despite the clinical benefits, ICIs are associated with immune-related adverse events (irAEs), which are considered off-target tissue damage and involve essentially every organ system.2 Vasculitis is a rare toxicity associated with ICIs, with an estimated incidence of 0.26% and affecting vessels of any size.3^,^4 Aortitis is considered a very rare irAE and carries the risk of aneurysmal degeneration and rupture that can be life threatening.3 This case report describes a patient with metastatic supraglottic laryngeal cancer treated with nivolumab, an ICI, who subsequently developed abdominal aortitis and retroperitoneal fibrosis. The patient consented to publication of their case and images.
Case report
A 60-year-old man was diagnosed with stage IVB squamous cell carcinoma of the supraglottic larynx in June 2020. He had a past medical history of rectal adenocarcinoma treated with neoadjuvant chemoradiation and abdominoperineal resection in 2013, hypothyroidism, and active smoking. The tumour was positive for expression of PD-L1, CD31, and D2-40 markers. A baseline computed tomography (CT) scan showed mild aortic atherosclerotic disease. He was treated with cisplatin with concurrent radical radiotherapy initially.
A CT scan in December 2020 showed findings highly suggestive of pulmonary metastases. Nivolumab, an ICI, was started February 2021 with palliative intent. A CT scan in May 2021 showed improvement of the lung nodules and evidence of mild circumferential infrarenal aortic wall thickening in keeping with early aortitis changes (Fig 1). Acute phase reactants and inflammatory workup were all within normal limits and white blood cell scan was negative for infectious etiology. Repeat imaging in October 2021 and again in January 2022 demonstrated further progression with a maximal wall thickness of 0.8 cm and axial diameter measuring 3.2 cm × 2.9 cm. Owing to these progressive changes, nivolumab was held in March 2022 after discussion with medical oncology, rheumatology, and vascular surgery. The patient was asymptomatic, and the multidisciplinary team decided against steroid treatment.Fig 1. Enhanced computed tomography (CT) scan of the abdomen from May 2021. After 3 months of nivolumab therapy. Early infrarenal aortitis (1) with maximal aortic wall thickness measured at 4.2 mm. Mild aortic calcification is seen, which is stable from prior imaging.
A CT scan 1 month after discontinuing nivolumab demonstrated increased maximal aortic wall thickness of 1.6 cm and axial diameter measuring 3.9 × 3.3 cm and new finding of retroperitoneal fibrosis (Fig 2). At this time, the patient remained asymptomatic. Approximately 3 weeks later, the patient presented to the emergency department complaining of intense left flank pain. A CT scan demonstrated left hydronephrosis from obstruction of the ureter, which was presumed secondary to retroperitoneal fibrosis and a ureteric stent was placed.Fig 2. Computed tomography (CT) angiography of the abdomen from April 2022. One month after the discontinuation of nivolumab. Infrarenal aortitis (1) with maximal aortic wall thickness measured at 16 mm and axial diameter 39.1 mm. New finding of retroperitoneal fibrosis (2).
A follow-up CT scan 6months after discontinuing nivolumab showed stability in the infrarenal aortic measurements (Fig 3). However, the retroperitoneal fibrosis remained active and had further progressed to extend from the left renal vein to the common iliac arteries. Unfortunately, the patient developed additional findings of a necrotic pancreatic head mass and liver lesions concerning for metastases. Subsequent positron emission tomography scan showed no evidence of active aortitis, but ongoing retroperitoneal fibrosis and concerns of a pancreatic primary cancer with metastases to liver and retroperitoneal lymph nodes. The diagnosis of primary pancreatic adenocarcinoma was confirmed with fine needle aspiration. Palliative chemotherapy was initiated; however, treatment was withdrawn owing to the patient's intolerance to feeds. The patient passed away in December 2022.Fig 3. Computed tomography (CT) angiography of the abdomen from September 2022. Six months after the discontinuation of nivolumab. Infrarenal aortitis (1) with stable maximal aortic wall thickness measured at 16 mm and axial diameter 38.5 mm with persistent retroperitoneal fibrosis (2). Left ureteric stent seen (3). Additional findings of a necrotic pancreatic head mass (4) and hypodense liver lesions (not visible in this cross-section).
Discussion
In addition to our case, a literature search yielded 16 case reports and a case series with 3 patients (not included in table, no individual data) with ICI-associated aortitis (Table).5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21 The ICIs with the most reported cases of aortitis are the programmed cell death protein 1 inhibitors nivolumab and pembrolizumab. Other ICIs reported include programmed cell death ligand 1 inhibitors atezolizumab and durvalumab and cytotoxic T lymphocyte antigen 4 inhibitor ipilimumab. Three of these cases were also treated with pegfilgrastim, a granulocyte colony-stimulating factor, which has also been reported to have large-vessel vasculitis as a rare complication.22 Aortitis is diagnosed based on the presence of homogenous circumferential thickening of the aortic wall on imagining or with histopathology.23 Aortic biopsy is not done routinely owing to the significant risks of the procedure. Previous literature reports a diagnosis of vasculitis a median of 3 to 4 months from initiation of ICI.21^,^24 This review calculated a diagnosis of aortitis a median of 3 months from initiation of immunotherapy.TableCases published reporting aortitis associated with immune checkpoint inhibitors (ICIs)CaseCancerICITiming, monthsClinicalLocationTreatmentResultsPresent caseHead and neckNivolumab3AsymptomaticInfrarenal aortaDiscontinue ICIStable aortitis, retroperitoneal fibrosisYildirim 20245Renal CellNivolumab33AsymptomaticThoracic aorta and great vesselsDiscontinue ICI, Steroid course (delayed)Improved 6 monthsRoy 20176LungNivolumab9Back painInfrarenal aortic aneurysmDiscontinue ICI, Steroid courseRemission 8 weeksLoricera 20187MelanomaNivolumab2AsymptomaticThoracic aortaNo dataNo dataHotta 20208LungNivolumab24AsymptomaticInfrarenal aortic aneurysmDiscontinue ICIRemission 2 monthsHenderson 20209ProstateNivolumab + ipilimumab4Chest and shoulder painThoracic aorta and great vesselsDiscontinue ICI, Steroid courseRemission 6 monthsBührer 202410MelanomaNivolumab + ipilimumab16AsymptomaticInfrarenal aortaDiscontinue ICI, steroid courseRemission 3 monthsOhno 202411Head and neckNivolumab23Chest pain, flu-like illnessAortic archDiscontinue ICI, steroid courseAneurysm rupture endovascular repairMort 202212BreastPembrolizumab + pegfilgrastim1.5Left shoulder and arm painAortic arch and great vesselsDiscontinue ICI, steroid courseRemission 8 weeksNinomiya 202213LungPembrolizumab2Flu-like illnessAscending aortaSteroid course, then restarted ICIAneurysmal degeneration surgical repairBloomer 202214MelanomaPembrolizumab15Chest pain, flu-like illnessAortic archDiscontinue ICI, steroid side effects, TocilizumabRemission, unknown timingKhan 202415MelanomaPembrolizumab3AsymptomaticAscending aortic aneurysmDiscontinue ICIAneurysmal degeneration surgical repairPinkston 201616MelanomaPembrolizumab1Abdominal painPerivisceral aortaNo dataNo dataLiguori 202117PancreaticAtezolizumab2Abdominal painPerivisceral aortaSteroid course, then restarted ICIRecurrence treated with steroids, restart ICI with second recurrence, switch to different ICI no recurrenceShiraha 202418LungAtezolizumab + pegfilgrastim2Back painThoracic aorta and great vesselsSteroid course, then ICI restartedRemission 3 monthsIto 202319LungDurvalumab + pegfilgrastim12 daysFlu-like illnessAortic archDiscontinue ICI (hepatitis B, no steroids)Remission 1 monthBan 201720MelanomaIpilimumab2Abdominal pain, flu-like illnessThoracic aortaDiscontinue ICI, steroid courseSymptom relapse treated with prolonged steroid taper
The management of ICI irAEs is challenging owing to a lack of standard guidelines and evidence-based recommendations, which vary based on affected organ system, severity, and clinical judgment.25 These recommendations include discontinuation of ICIs and initiation of high-dose steroids (prednisone or methylprednisolone 1-2 mg/kg/d), which is tapered over 4 to 6 weeks.25 Despite these recommendations, there is little to no evidence to support whether steroid treatment is effective; both responders and nonresponders to steroids have been reported.24 From the case reports, 11 patients received steroids, of which there were 2 steroid nonresponders11^,^20 and 8 steroid responders.5^,^6^,^9^,^10^,^12^,^13^,^17^,^18 Bloomer et al14 used tocilizumab as a steroid-sparing agent for their patient who was having side effects, and they had remission of the aortitis. Ban et al20 commented that a prolonged steroid taper may be necessary with severe immune reactions to achieve full response. Ohno et al11 treated with steroids but still had aneurysmal degeneration and rupture requiring repair. Of the three cases that did not receive steroids, two went into remission8^,^19 and one had aneurysmal degeneration requiring repair.15 Furthermore, it remains unclear when or if at all ICIs should be resumed after effective steroid treatment; three of the cases reinitiated ICIs after the steroid course. Ninomiya et al13 restarted the ICI and there was aneurysmal degeneration requiring surgical repair. Liguori et al17 restarted the ICI and there was recurrence of symptoms and extension of the aortitis, which was treated successfully with another course of steroids. Shiraha et al18 reported no recurrence with the reinitiation of ICI. Treating asymptomatic patients with steroids is also unclear. Four cases in the series were asymptomatic. Two received steroids and experienced remission.5^,^10 Two cases did not receive steroids, one of which experienced remission8; the other had aneurysmal degeneration requiring repair.15
In our patient's case, treatment with steroids may have prevented the progression of retroperitoneal fibrosis, which caused ureteric obstruction. However, at the time of the multidisciplinary meeting, the patient was asymptomatic. From the gathered cases, it seems that discontinuation of the ICI and steroids is the most common strategy and is effective at achieving remission. Even in patients who are asymptomatic, steroids may prevent the progression of complications such as aneurysmal degeneration and rupture and prevent further interventions. However, these conclusions are limited by the low case numbers. Steroids are not benign, having numerous adverse effects; therefore, the decision to give steroids should be based on multidisciplinary discussion and patient presentation.26
Conclusions
Although rare, our literature search found 19 cases of aortitis in patients receiving ICIs; therefore, it is imperative to keep vascular-related irAEs in mind when prescribing for patients with cancer. As the indications for immunotherapy expand, these rare complications will become more frequent, and more data will be needed to guide their management. An appropriate strategy for treatment includes discontinuing the ICI and considering steroids. In the absence of sufficient literature, physicians must rely on multidisciplinary discussion and weighing the severity of the aortitis against the treatment of the cancer and potential side effects from steroids.
Funding
None.
Disclosures
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dang Q.M.Watanabe R.Shiomi M.Rheumatic immune-related adverse events due to immune checkpoint inhibitors-A 2023 update Int J Mol Sci 24202356433698271510.3390/ijms 24065643 PMC 10051463 · doi ↗ · pubmed ↗
- 2Alsaab H.O.Sau S.Alzhrani R.PD-1 and PD-L 1 checkpoint signaling inhibition for cancer immunotherapy: mechanism, combinations, and clinical outcome Front Pharmacol 820175612887867610.3389/fphar.2017.00561 PMC 5572324 · doi ↗ · pubmed ↗
- 3Liu G.Chen T.Zhang X.Hu B.Shi H.Immune checkpoint inhibitor-associated cardiovascular toxicities: a review Heliyon 102024 e 2574710.1016/j.heliyon.2024.e 25747 PMC 1090768438434280 · doi ↗ · pubmed ↗
- 4Salem J.E.Manouchehri A.Moey M.Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study Lancet Oncol 192018157915893044249710.1016/S 1470-2045(18)30608-9PMC 6287923 · doi ↗ · pubmed ↗
- 5Yıldırım R.Shikhaliyeva A.İçer H.An underrecognized association: immune checkpoint inhibitor-related aortitis, a case report with the review of the literature Int Cancer Conf J 1320242352393896205110.1007/s 13691-024-00668-4PMC 11217252 · doi ↗ · pubmed ↗
- 6Roy A.K.Tathireddy H.R.Roy M.Aftermath of induced inflammation: acute periaortitis due to nivolumab therapy BMJ Case Rep 20172017 bcr 201722185210.1136/bcr-2017-221852 PMC 574778428942413 · doi ↗ · pubmed ↗
- 7Loricera J.Hernández J.L.García-Castaño A.Martínez-Rodríguez I.González-Gay M.Blanco R.Subclinical aortitis after starting nivolumab in a patient with metastatic melanoma. A case of drug-associated aortitis?Clin Exp Rheumatol 36201817129799390 · pubmed ↗
- 8Hotta M.Naka G.Minamimoto R.Takeda Y.Hojo M.Nivolumab-Induced periaortitis demonstrated by FDG PET/CT Clin Nucl Med 4520209109123270181510.1097/RLU.0000000000003215 · doi ↗ · pubmed ↗