Are Canadian Clinical Practice Guidelines Accounting for Adults With Multiple Chronic Diseases? A Systematic Review
Olivia L. Tseng, Shanjot Brar, Martin Dawes, Hetesh Ranchod, Diane Lacaille, Victoria C.H. Su, Craig Mitton

TL;DR
This paper reviews Canadian clinical guidelines to see how well they address adults with multiple chronic diseases, finding significant inconsistencies.
Contribution
The study systematically evaluates Canadian guidelines for multimorbidity using AGREE II, highlighting gaps in demographic and health outcome information.
Findings
Half of the guidelines were high-quality, but definitions and evidence levels varied.
Most guidelines focused on single diseases and missed health outcomes or demographics.
Pharmacological and nonpharmacological recommendations had more health outcomes than screening or diagnosis.
Abstract
Recommendations that are equipped with essential and adequate information promote adherence and support evidence‐informed decision‐making, which are crucial attributes of patient‐centered care when caring for patients with multiple coexisting health conditions. To systematically evaluate the content of recommendations of Clinical Practice Guidelines in Canada. We searched PubMed, MEDLINE, Embase, and professional organization websites to identify 18 Canadian guidelines addressing 14 diseases prevalent in adults with multimorbidity in nonhospital settings. Two reviewers independently appraised the included guidelines using the international AGREE II tool, extracted 2,509 recommendations and assessed each recommendation to determine the presence of primary health outcomes, as well as secondary demographics and the number of involved diseases. We stratified the findings by potential…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
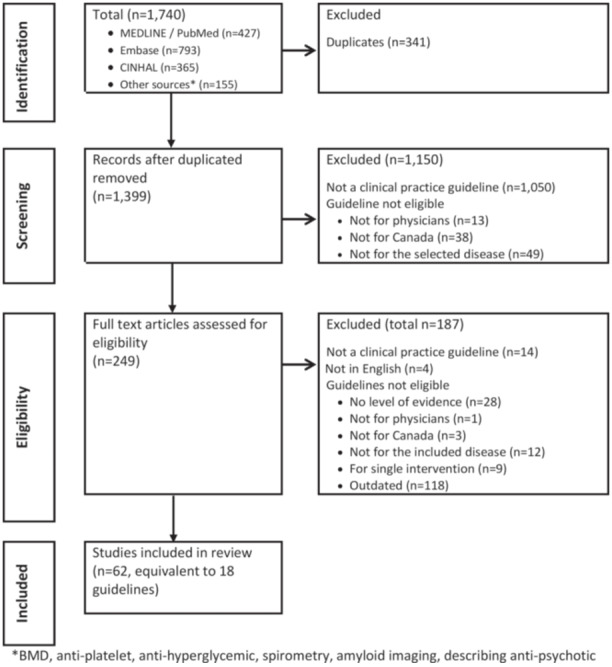 Figure 1
Figure 1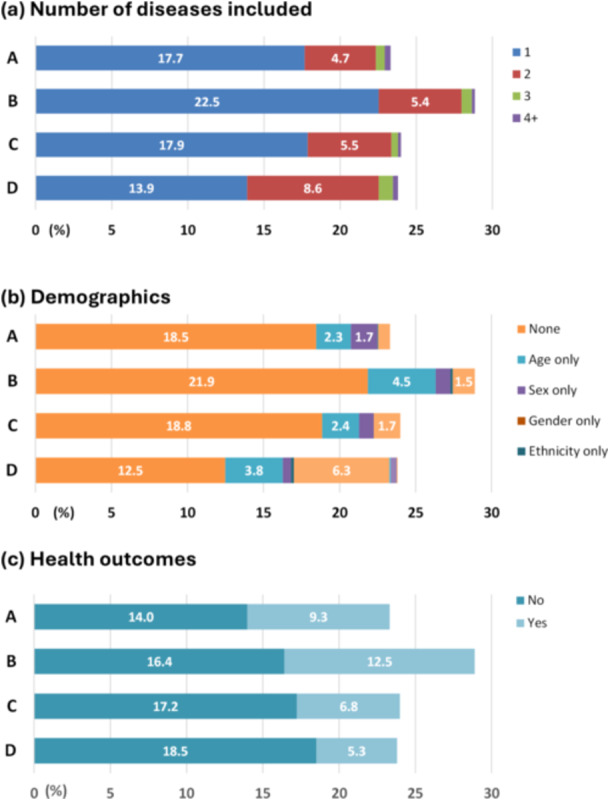 Figure 2
Figure 2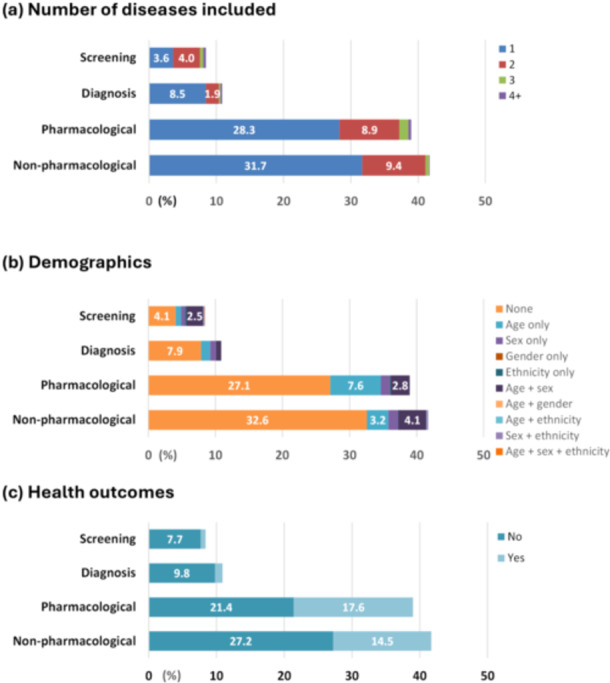 Figure 3
Figure 3| Outcome(s) | Example guide recommendation | Guidelines |
|---|---|---|
| Age, sex, and health outcome | We recommend that a cardiovascular (CV) risk assessment be completed every 5 years for “men and women” aged “40 to 75” years using the modified Framingham Risk Score or Cardiovascular Life Expectancy Model to guide therapy to “reduce major CV events” (Strong Recommendation; High Quality Evidence). | Dyslipidemia [ |
| Coexisting disease ( | For hypertensive patients with “coronary artery disorder (CAD),” but without coexisting systolic heart failure, the combination of an ACE inhibitor and ARB is not recommended (Grade B) | Hypertension [ |
| Sex, Ethnicity | Attainment of a healthy body weight before conception should be pro‐ moted among “Indigenous women” to reduce their risk for gestational diabetes mellitus (GDM) (Grade D, Consensus) | Diabetes [ |
| Assuming all ages, both sexes and any ethnicity, health outcome | We recommend physical activity to “reduce the risk of developing heart failure” in “all individuals” (Grade A). | Heart Failure [ |
| Health outcome | Prophylactic use of anticonvulsant medications in patients with ischemic stroke is not recommended and there is some evidence to suggest possible harm with “negative effects on neurological recovery” (Evidence Level C) | Stroke – acute stroke management [ |
| Guideline | Grading Recommendation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Level of evidence (LOE) | Strength of recommendation (SOR) | |||||||||
| Disease | Year | Organization | Status | Rec ( | System | Format | Levels High‐Low | Factors | Grading High‐Low | Factors |
| Anxiety [ | 2014 | Anxiety Disorders Association of Canada | New | 217 | Custom system |
(LOE) OR SOR (LOE) | 1–4 | Strength of evidence for the intervention |
1st−3rd line, not rec | Level of evidence, clinical trial efficacy, clinical practice effectiveness and side effects |
| Asthma [ | 2012 | CTS | Update | 37 | CHEST grading system | (SOR, LOE) | A–C, consensus | Methodological quality | Strong, weak, consensus | Benefits versus risk and burden including cost, associated with adherence to the recommendations, morbidity, mortality, and quality of life. |
| COPD [ | 2017 | CTS | Update | 23 | CHEST grading system | (SOR, LOE) | A–C, consensus | Methodological strength | 1, 2, consensus | Strength of supporting evidence and strength of recommendation based on benefits versus risks, harms, and burdens |
| Coronary Artery Disease [ | 2014 | CCS | New | 38 | GRADE System 2010 | (SOR, LOE) | High–very low quality | Strength of evidence | Strong, conditional |
Quality of evidence, difference between desirable and undesirable effects, values and preferences and cost (For diagnostic testing): |
| Dementia [ | 2015 | CTFPHC | Update | 1 | GRADE system 2013 | (SOR, LOE) | High–very low quality | Likely further research is to change our confidence in the estimate of effect | Strong, weak | Quality of supporting evidence, the degree of uncertainty about the balance between desirable and undesirable effects, the degree of uncertainty or variability in values and preferences, and the degree of uncertainty about whether the intervention represents a wise use of resources |
| Depression [ | 2016 | CANMAT | Update | 255 | Modified GRADE system |
(LOE) OR SOR (LOE) | 1–4 | Methodological strength | 1st−3rd line | Level of evidence and clinical support reflecting expert opinions on feasibility, availability, and clinical effectiveness |
| Diabetes [ | 2018 | Diabetes Canada | Update | 656 | A standardized tool2 | (SOR, LOE) | 1–4 | Paper's objective, methodological rigor, susceptibility to bias and generalizability | A–D (strong–weak) | Totality of evidence (relative strength in methodology and study findings), uncertainty for studies with conflicting outcomes and applicability to Canadian population |
| Dyslipidemia [ | 2016 | CCS | Update | 66 | GRADE system | (SOR, LOE) | High–very low quality | Methodological strength | Strong, conditional | N/A |
| Heart Failure [ | 2017 | CCS | Update | 183 | GRADE system 2008/2016 | (SOR, LOE) | High–very low quality | Methodological strength | Two levels: Strong and weak | N/A |
| Hypertension [ | 2018 | Hypertension Canada | Update | 219 | Hypertension Canada Grading system | (Custom) |
A–D (strong–consensus) Factor: study methodological quality, effects on a hierarchy of validated clinical outcomes (priority given to cardiovascular morbidity and mortality), and that potential benefits must outweigh potential harms | |||
| Osteoporosis [ | 2014 | Osteoporosis Canada | Update | 14 | CTFPHC | (LOE, SOR) | I, II‐1, II‐2, II‐3, III | Methodological strength | A–D, E | Strength of supporting evidence |
| Rheumatoid Arthritis [ | 2012 | CRA | New | 56 | SIGN system | (LOE, SOR) | I–IV | Methodological strength | A–D (strong‐consensus) | Based on strength of supporting evidence and applicability |
| Stroke [ | 2017‐2018 | HSF | Update | 283 | GRADE system, 2008 | (LOE) | A–C, clinical consideration | Methodological strength, benefits versus harms | None | None |
| Substance use [ | 2018 | Canadian Research Initiative in Substance Misuse | New | 11 | CTFPHC | (LOE, SOR) | I, II‐1, II‐2, II‐3. III | Methodological strength | A–D, E | Strength of supporting evidence |
| Domain Score (%) | ||||||||
|---|---|---|---|---|---|---|---|---|
| 1: Scope and purpose | 2. Stakeholder involvement | 3. Rigor of development | 4. Clarity of presentation | 5. Applicability | 6. Editorial Independence | Mean domain score (SD) | Overall | |
| Anxiety, 2014 [ | 94 | 61 | 68 | 81 | 21 | 92 | 69 (27) | L |
| Asthma, 2012 [ | 100 | 67 | 100 | 100 | 100 | 100 | 94 (14) | H |
| Chronic obstructive pulmonary disease, 2017 [ | 97 | 97 | 79 | 100 | 56 | 100 | 88 (18) | H |
| Coronary artery disease, 2014 [ | 81 | 53 | 29 | 97 | 52 | 88 | 67 (26) | L |
| Dementia, 2012 [ | 97 | 58 | 56 | 94 | 29 | 100 | 73 (29) | L |
| Depression, 2016 [ | 97 | 64 | 60 | 86 | 46 | 100 | 76 (22) | L |
| Diabetes, 2018 [ | 94 | 100 | 98 | 100 | 81 | 100 | 96 (7) | H |
| Dyslipidemia, 2016 [ | 89 | 67 | 41 | 100 | 35 | 100 | 72 (29) | L |
| Heart failure, 2017 [ | 89 | 67 | 64 | 100 | 38 | 100 | 76 (25) | L |
| Hypertension, 2018 [ | 97 | 56 | 98 | 97 | 86 | 100 | 89 (17) | H |
| Osteoporosis, 2010 [ | 92 | 50 | 48 | 60 | 8 | 71 | 55 (28) | L |
| RA, 2011 [ | 100 | 100 | 76 | 92 | 76 | 100 | 91 (12) | H |
| Stroke, 2017 [ | 84 | 94 | 85 | 99 | 80 | 100 | 90 (9) | H |
| Substance use, 2018 [ | 92 | 72 | 66 | 60 | 65 | 88 | 74 (13) | H |
| Mean (SD) | 93 (6) | 72 (18) | 69 (22) | 91 (14) | 55 (28) | 96 (9) | ||
- —This study was not supported by any grants. S.B. was financially supported by a 2018 Summer Student Research award provided by the Faculty of Medicine of the University of British Columbia. O.L.T. was
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Disease Management Strategies · Clinical practice guidelines implementation · Health Systems, Economic Evaluations, Quality of Life
Introduction
1
Multimorbidity is an increasingly significant issue that challenges healthcare systems worldwide. One in three individuals is considered multimorbid, meaning they have two or more coexisting long‐term chronic health conditions [1]. The prevalence of multimorbidity is particularly high in North America, where it affects 43% of the population [1]. Despite being high users of healthcare services [2], individuals with multimorbidity often experience poorer health outcomes [3] and a lower quality of life [4]. Their care needs are often complex, encompassing biomedical, psychological, and social aspects. While this patient group continues to grow, their care remains suboptimal. To tackle these pressing challenges, the World Health Organization (WHO) [5] and the National Institute for Health and Care Excellence (NICE) [6] strongly advocate for a patient‐centered approach. This emphasizes the importance of providing only “selected” and “prioritized” care aligning with the personal preferences of multimorbid patients [7]. However, this approach has not been adequately supported by existing clinical practice guidelines due to their known unclear applicability and interpretability.
Clinical practice guidelines are designed to assist clinicians in delivering consistent, high‐quality care to promote patient health [8, 9, 10]. Most guidelines primarily focus on single diseases, largely due to the lack of research evaluating disease‐disease, disease‐drug, and drug‐drug interactions [11]. Applying multiple guideline recommendations simultaneously to manage the various conditions of a multimorbid patient can lead to fragmented care and an increased treatment burden [12, 13, 14]. Furthermore, most guidelines tend to prioritize generalization over specificity, often developing one‐size‐fits‐all guideline recommendations [15]. These broad guideline recommendations frequently overlook key factors that are essential for patient‐centered care, such as demographic variables that influence treatment outcomes, coexisting health conditions that may interact with drugs and diseases, and the balance of benefits and harms critical for shared decision‐making. The absence of these factors reduces the applicability and interpretability of guideline recommendations, leading to poor compliance driven by increased uncertainty and confusion among both providers and patients [15, 16, 17, 18, 19].
The international experts recommended considering applicability and quality of evidence when applying existing evidence to multimorbid patients, including factors such as the demographics of study populations, as well as the benefits and harms [20]. Moreover, several articles have advocated for incorporating factors such as age, race, and sex into guideline development [21, 22, 23]. However, the extent to which guideline recommendations integrate these factors to facilitate patient‐centered care remains unclear, particularly in countries without a centralized guideline organization, such as Canada. This lack of standardization results in noticeable variations in the development process, content, and format of guideline recommendations. Therefore, this study aims to compare the content of Canadian guideline recommendations from a multimorbidity perspective to enhance awareness and identify knowledge gaps.
Methods
2
This is a systematic review evaluating Canadian guideline recommendations from a multimorbidity perspective. We registered the study protocol at PROSPERO (registration number CRD42020105261, available at: https://ww.crd.york.ac.uk/PROSPERO/ ). We reported study results using criteria from the Preferred Reporting Items for Systematic Review and Meta‐analysis Protocols (PRISMA) [24]. Two independent reviewers (SB/DB, OT) selected studies and extracted data at each stage. Reviewers SB and DB alternated as the first reviewers. The reviewers resolved disagreements by discussion.
A Clinical Practice Guideline is a text document that includes one or more evidence‐based guideline recommendations primarily related to a disease, such as diabetes or hypertension. Each guideline recommendation is a brief statement formulated with research evidence extracted from literature reviews or experts' opinions when research evidence is lacking [25, 26]. Each recommendation answers a clinical question of when and how to screen, prevent, investigate, treat or manage the target disease [8]. The quality of a recommendation is often rated with a level of evidence (LOE), strength of recommendation (SOR) or both [27]. A LOE reflects the methodological quality, validity, and reliability of evidence that forms the recommendation. A SOR indicates the magnitude of outcomes, effects of what would occur when following the recommendation.
Search Strategy
2.1
We included the MEDLINE, Embase, and CINAHL databases in our search for their broad healthcare research content and excluded the CENTRAL data set for controlled trials. We consulted a UBC senior librarian with expertise in clinical systematic reviews to build search strategies. The first author (OT) searched three databases with the keywords and MeSH terms extracted from sample articles related to the study (Appendix I). The search result was then limited to the English language and the year of publication, 2010–2018. We validated the search strategies using 10 sample articles and examined 20% of articles excluded and included when adding or removing keywords or MeSH terms. We also hand‐searched the Canadian Medical Association (CMA) guideline database and Canadian professional organization websites. The search was initially completed in April 2018, which was then revised and executed again on August 26, 2020.
Study Selection
2.2
Articles identified by the search strategy were exported to Endnote X9 reference management software (Clarivate Analytics, Philadelphia), where duplicates were removed. The remaining articles were then exported to an Excel worksheet for title/abstract screening, followed by full article reviews (Figure 1).
*PRISMA flow sheet. BMD, antiplatelet, anti‐hyperglycemic, spirometry, amyloid imaging, describing anti‐psychotic.
We included articles that were the most current guidelines developed for Canadian physician use, targeted one of 14 pre‐selected common diseases in nonhospital settings, included recommendations graded for LOE, and were primarily for adults aged 18+ (Appendix II). Only Canadian guidelines were selected to align with our study aim and to avoid intercountry variation in guideline format. Adults aged 18+ were selected as they account for most patients with multimorbidity [28]. We excluded guidelines focused on interventions (e.g. catheter‐directed treatment) or drugs (e.g. anti‐hyperglycemic) and articles derived from primary guidelines without LOE assigned. Our limited resources restricted us to 14 pre‐selected diseases that commonly coexist in multimorbidity patients based on our literature review [28, 29].
We noticed two unique situations. First, guidelines for three diseases were published as sequentially numbered chapters in more than one peer‐reviewed article, such as DM (342 pages, 37 articles) [30], depression (seven articles) [31], and RA (two articles) [32, 33]. Considering they were generated simultaneously and related, we collated them by disease for quality appraisal and data extraction. We also searched for single references for these three guidelines to reduce the reference complexity. Second, guidelines for hypertension [34, 35] and stroke [36, 37, 38] were published in more than one article: related subtopics by different author teams from the same organizations in the same calendar year. We appraised each article individually. The scores were similar across guidelines for the same disease. So, we reported averaged scores for each disease and collated them accordingly for data extraction.
Quality Appraisal
2.3
We selected the Appraisal of Guidelines for Research and Evaluation (AGREE)‐II criteria [39] for its well‐known reputation in the guideline field. The AGREE tool consists of 23 items categorized into six domains: scope and purpose (Domain 1 (D1), three items), stakeholder involvement (D2, three items), rigor of development (D3, eight items), clarity of presentation (D4, three items), applicability (D5, four items) and editorial independence (D6, two items). Both reviewers (OT and SB) completed online training modules (https://www.agreetrust.org/agree-ii/) before the appraisal. Each reviewer scored a guideline for each item, ranging from 1 (lowest) to seven (highest). Item scores within each domain were used to calculate domain scores in percentage based on the formula “(obtained score – minimal possible score) divided by (maximum possible score – minimum possible score)” [39]. We then generated a mean domain score, an average of six domain scores, for each guideline to represent its overall quality. A guideline was considered high quality if all domains scored at least 50%, a common cut‐off based on Bargeri et al. study [40]. Reviewer agreement (inter‐rater reliability) was assessed by comparing their domain scores using linear weighted Kappa (http://vassarstats.net/kappa.html ) and defined as fair (kappa=0.21–0.4), moderate (0.41–0.6) or substantial (0.61–0.8) [41].
Data Extraction
2.4
The reviewers extracted data onto standardized Excel worksheets, including bibliographic information (author, year), guideline information (disease, new/updated status of the guideline, number of included recommendations, the grading system for recommendation including LOE and SOR, and outcomes) (Appendix III).
A guideline recommendation is defined as a “systematically developed statement to assist practitioners and patient decisions about appropriate health care for specific circumstances” [42]. The recommendations often included the word “recommend and summarized in boxed text, gray‐colored text, summary tables or special paragraphs.
Outcomes
2.5
The primary outcome was whether a recommendation included health outcome information, either positive (benefits) or negative (harms) (Table 1). We initially focused on common ones, quality‐adjusted life years (QALY, cost‐effectiveness) and the number needed to treat (NNT, clinical effectiveness), which existed in fewer than 1% of the extracted recommendations. So, we expanded to include any health outcomes in the final analysis, ranging from QALY to NNT, incremental cost‐effectiveness ratio (ICER), disease incidence and hospitalizations [45], disease incidence, hospitalizations, and side effects. Reviewers categorized a recommendation as “Y” (Yes) if it included health outcome information.
The secondary outcomes were the existence of demographics and the number of coexisting diseases (Table 1). When it had demographic information, each recommendation was categorized as “Y” (Yes) for age, gender, sex, and ethnicity, respectively. Age information in a recommendation can be presented as age group (e.g., 40–60 years old, middle‐aged), age threshold (> 60 years old) or descriptive words of adults, older adults, or all individuals. Sex, defined as biological and physiological characteristics [46], was presented as males, females, men and women in this study. Gender, defined as socially and culturally constructed roles [46], was presented as trans‐men, trans‐women, female‐to‐male, male‐to‐female, transgender males and transgender females. To distinguish between sex and gender in this study, men and women were classified into sex but not gender. Reviewers also counted the number of coexisting diseases included in each recommendation.
Data Analysis
2.6
We conducted descriptive analyzes of frequency counts and percentages stratified by grades and types of recommendations. Both grade and type factors may influence the recommendation distributions.
However, recommendation grading was inconsistent among guidelines. Most studies adopted or modified a GRADE system to grade recommendations in the format of (SOR, LOE) (Table 2). While SOR focused on effectiveness (health outcomes), LOE primarily evaluated methodological strengths. We developed an artificial four‐tiered system to reclassify the extracted recommendations based on their LOEs to promote comparability. The Reviewers reassigned each recommendation into A (highest LOE in the original guideline), B (second highest), C (third highest) or D (lowest). For Osteoporosis and Substance Abuse guidelines, we condensed their original six LOEs into four by aligning their definitions with other guidelines (Appendix IV). We chose LOE over SOR due to more consistent definitions and levels among the included guidelines. Also, SOR overlapped with the study outcomes in evaluating effectiveness based on health outcomes.
The reviewers categorized recommendations into one of the following types.
- Screening (disease screening and prevention and risk factor identification).
- Diagnosis (such as disease criteria, evaluation investigation and prognosis).
- Pharmacological management (prescription drugs).
- Nonpharmacological management treatment (treatments other than medications, such as surgical interventions, referrals, and monitoring with therapeutic goals) or Lifestyle (e.g., exercise, diet, or supplements).
Results
3
We identified 1740 unique articles after 341 duplicates were removed (Figure 1). Reviewers excluded 1150 and 187 articles at the title/abstract and full‐text review stages, respectively. A total of 62 articles fulfilled our selection criteria. We collated them into 18 guidelines for quality appraisal and data extraction.
Study Characteristics
3.1
The included guidelines were published between 2012 and 2018 and developed by Canadian professional organizations (Table 2). Four of them were new guidelines, while the others were updated ones. The number of recommendations varied significantly, ranging from one (Dementia guideline) to 249 (Diabetes guideline). LOE was graded in heterogeneous formats, such as A–D, 1–4 or high‐moderate‐low‐very low.
Quality Appraisal
3.2
Half of the included guidelines were high‐quality, with all domains scoring at least 50%. The mean domain scores ranged from 55 to 96 (Table 3). Most guidelines scored well in the domains of scope and purpose (domain score, 93), clarity of presentation (91), and editorial independence (96). The score of the applicability domain varied significantly across the included guidelines, with the lowest for the osteoporosis guideline [8] and the highest for the asthma guideline (100). Inter‐rater reliability among reviewers (OT, SB) was moderate based on a 0.72 weighted Kappa coefficient (95% CI, 0.68–0.76).
CPG Recommendations
3.3
We extracted and examined a total of 2509 guideline recommendations (Figures 2 and 3, Appendices V and VI). Most of the recommendations mentioned one disease (the one targeted by the guideline, 72%), did not include any demographic information (72%), or did not state health outcomes (66%). When demographic information existed, age‐only or an age‐sex combination was more common than other demographics (i.e., sex only, gender only, ethnicity only, or an age‐ethnicity combination).
Distribution of guideline recommendations by their grades and study outcomes. (a) Number of dieases included. (b) Demographics. (c) Health outcomes.
Distribution of guideline recommendations by their types and study outcomes. (a) Number of dieases included. (b) Demographics. (c) Health outcomes.
When stratified by four levels of evidence (LOE), the distribution of recommendations was roughly equal, ranging from 23% (level A) to 29% (level B). The combination of age and sex was the most common demographic identified in 129 level D recommendations, accounting for 6.3% of all recommendations. Health outcome information was more prevalent in level B recommendations (12.5% of all included recommendations) than in other levels (ranging from 5.3% to 9.3%).
When stratified by type of recommendation, the distribution was skewed. More than 40% of the recommendations were for nonpharmacological management (41%), followed by pharmacological treatments (39%), diagnosis (11%), and screening (9%). Age alone was the most common demographic identified in 66 nonpharmacological management recommendations, accounting for 3.2% of all recommendations. Health outcomes were more frequently stated in pharmacological (17.6%) and nonpharmacological (14.5%) management.
Discussion
4
This study comprehensively assessed the content of guidelines for 14 health conditions prevalent among adult patients with multimorbidity. The findings elucidate the challenges posed by the content in delivering patient‐centered quality care. Specifically, over half of the extracted recommendation statements lacked demographic and/or health outcome data. Demographics are necessary for assessing applicability, ensuring recommendations are suitable for individual patients, while health outcomes are essential for patients to make informed decisions aligned with their personal circumstances and preferences. An unforeseen revelation from our study is the disparity in the length, grading system defining Levels of Evidence (LOE), and organization of recommendations within the guidelines. This variability unintentionally adds complexity and confusion to readers navigating through the guidelines.
Our study, employing a similar multimorbidity lens, diverged from the research conducted by Fortin et al. in 2011 [54], particularly in the examination of Canadian guidelines. A notable point of departure lies in the scale of our analysis: guideline versus guideline recommendation. Fortin et al. assessed 16 guidelines using a validated 14‐item checklist, whereas our study evaluated 2500 individual guideline recommendations extracted from 18 guidelines. While the terms guideline and guideline recommendation are often used interchangeably, it is important to distinguish between them. A guideline typically contains multiple guideline recommendations, short statements, or pieces of advice. In our study, for example, the Diabetes guideline included over 600 recommendations, primarily targeted at adults. Of these, 32 recommendations specified age groups, such as ≥ 40, 14–29, 19–64, ≥ 65, < 55, or < 75; more than 200 mentioned adults, older adults, or older adults; and the remaining recommendations lacked any age‐related information. This suggests that the underlying research evidence for these recommendations may be derived from populations that vary by age, gender, sex, ethnicity, and comorbidities. Any recommendations that lack age‐specific information pose a greater challenge for frontline physicians, as it becomes harder to determine their applicability in practice.
Our study findings highlighted barriers identified by prior studies assessing users' experiences, such as lack of applicability, outcome expectancy, and user‐friendliness [15, 17, 18, 55]. Canadian Thoracic Society, a major guideline developer in Canada, advocates “optimal use of language and format to convey recommendations” to promote guide implementation [56]. In this study, the recommendation statements were presented in various formats: integrated in text, as paragraphs in gray backgrounds, within text boxes, or in summary tables. Some statements stood alone, while others were accompanied by clinical questions or relevant research evidence.
Inconsistent recommendation grading further exacerbated confusion. The 18 included guidelines were graded by at least seven systems and presented in four different formats (LOE alone, (SOR, LOE), (LOE, SOR), or SOR (LOE)). Upon closer examination, we noticed the definitions of LOE and SOR also varied from one guideline to another. What may be classified as level‐A evidence in one guideline could be downgraded to level‐B in another. This inconsistency undermines providers' confidence in applying guideline recommendations, which is a barrier to implementing guidelines.
Individualized care is critical when caring for patients with multimorbidity, especially old adults with limited life expectancy. The process involves balancing positive and negative health outcomes (benefit and harm), prioritizing coexisting diseases, and aligning care options with personal preferences [20]. Although our study identified health outcome information in 33% of the extracted recommendations, they often lack quantitative effects to support decision‐making. An example was ‘to reduce hospital admission,’ which did not specify a rate to quantify the reduction. The omission of the rate was intentional, as guidelines often extrapolate evidence from trial participants to larger populations. However, this generalization process hinders patient‐centered care.
In addition to content and format issues that our study demonstrated, there have been efforts to promote better utilization of Clinical Practice Guidelines for multimorbid patients. One approach entails the harmonization of recommendations across individual or regional guidelines to mitigate inconsistencies. An example is the Canadian Cardiovascular Harmonized National Guidelines Endeavour (C‐CHANGE) [57]. Its 2022 version organized 83 recommendations related to multimorbidity based on disease combinations, such as the triad of obesity, diabetes, and hypertension [57]. Unfortunately, it encountered challenges related to inconsistent formatting and variation in evidence grading, thereby warranting further refinement and standardization. Concurrently, another significant effort centers on leveraging computer technology, including machine learning. Guideline knowledge is being integrated into clinical decision support systems (CDSSs), integrated with electronic health record data or incorporated into a Health Information System [58]. Despite their potential for positively impacting patient care, CDSSs encounter limitations concerning data integration and operational efficiency [59]. More recently, there is growing interest in using artificial intelligence to search databases, extract relevant information and summarize advice that is personalized [60]. However, artificial intelligence remains in its infancy, with potential biases and misleading results. Further studies are needed to resolve these limitations.
Limitations
5
The study had a few limitations. Firstly, we only focused on Canadian guidelines to highlight the need for a centralized guideline development agency. Our study findings could potentially be applicable to other countries with similar settings and multiple independent guideline developers. Secondly, this study was limited to 14 diseases due to resource constraints. Certain common health conditions, such as obesity, were not included. However, our study successfully demonstrated the inconsistent format among 18 guidelines. Adding more guidelines to this study will not meaningfully alter our findings and conclusions. Lastly, the guidelines we selected were developed between 2010 and 2018, which may be outdated and may not fully reflect content issues addressed in more recent guidelines. However, we expect format variations to persist as long as Canada lacks a centralized organization to standardize both the format and content.
Conclusion and Implication
6
Our findings underscore two key issues. Firstly, the absence of a centralized guideline development agency can result in an inconsistent process for distilling research evidence into recommendations, leading to variations in recommendation formats. This lack of uniformity has the potential to confuse both patients and providers, discouraging adherence to recommendations. Secondly, a significant portion of the Clinical Practice Guidelines lacked sufficient information to support evidence‐informed decision‐making, which is fundamental to patient‐centered care.
Conflicts of Interest
The authors declare no conflicts of interest.
Originality of Work and Previous Presentation of Manuscript
This study is completely original. A poster was virtually presented in North America Primary Care Research Group Conference held in San Francisco, California, USA on November 20–24, 2020.
Supporting information
Supplemental info.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. R. Chowdhury , D. Chandra Das , T. C. Sunna , J. Beyene , and A. Hossain , “Global and Regional Prevalence of Multimorbidity in the Adult Population in Community Settings: A Systematic Review and Meta‐Analysis,” E Clinical Medicine 57 (2023): 101860.10.1016/j.eclinm.2023.101860 PMC 997131536864977 · doi ↗ · pubmed ↗
- 2R. Palladino , J. Tayu Lee , M. Ashworth , M. Triassi , and C. Millett , “Associations Between Multimorbidity, Healthcare Utilisation and Health Status: Evidence From 16 European Countries,” Age and Ageing 45, no. 3 (2016): 431–435.27013499 10.1093/ageing/afw 044PMC 4846796 · doi ↗ · pubmed ↗
- 3B. P. Nunes , T. R. Flores , G. I. Mielke , E. Thumé , and L. A. Facchini , “Multimorbidity and Mortality in Older Adults: A Systematic Review and Meta‐Analysis,” Archives of Gerontology and Geriatrics 67 (2016): 130–138.27500661 10.1016/j.archger.2016.07.008 · doi ↗ · pubmed ↗
- 4T. T. Makovski , S. Schmitz , M. P. Zeegers , S. Stranges , and M. van den Akker , “Multimorbidity and Quality of Life: Systematic Literature Review and Meta‐Analysis,” Ageing Research Reviews 53 (2019): 100903.31048032 10.1016/j.arr.2019.04.005 · doi ↗ · pubmed ↗
- 5Multimorbidity: Technical Series on Safer Primary Care (World Health Organization, 2016).
- 6C. Farmer , E. Fenu , N. O'Flynn , and B. Guthrie , “Clinical Assessment and Management of Multimorbidity: Summary of Nice Guidance,” BMJ 354 (2016): i 4843.27655884 10.1136/bmj.i 4843 · doi ↗ · pubmed ↗
- 7I. van der Heide , S. P. Snoeijs , W. G. W. Boerma , F. G. Schellevis , and M. P. Rijken , “European Observatory Policy Briefs” in How to Strengthen Patient‐Centredness in Caring for People With Multimorbidity in Europe? Copenhagen (Denmark): European Observatory on Health Systems and Policies © NIVEL and TU Berlin, eds. E. Richardson and E. Van Ginneken (European Observatory Policy Briefs, 2017), 2017, https://pubmed.ncbi.nlm.nih.gov/29144693.29144693 · pubmed ↗
- 8S. H. Woolf , R. Grol , A. Hutchinson , M. Eccles , and J. Grimshaw , “Clinical Guidelines: Potential Benefits, Limitations, and Harms of Clinical Guidelines,” BMJ 318, no. 7182 (1999): 527–530.10024268 10.1136/bmj.318.7182.527PMC 1114973 · doi ↗ · pubmed ↗