A case of the girl with ruptured bladder caused by rectal dilatation due to imperforate anus
Nao Takami, Akinobu Taniguchi, Toshihiko Suzuki, Ryosuke Miura, Yukako Muramatsu, Yoshiaki Sato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
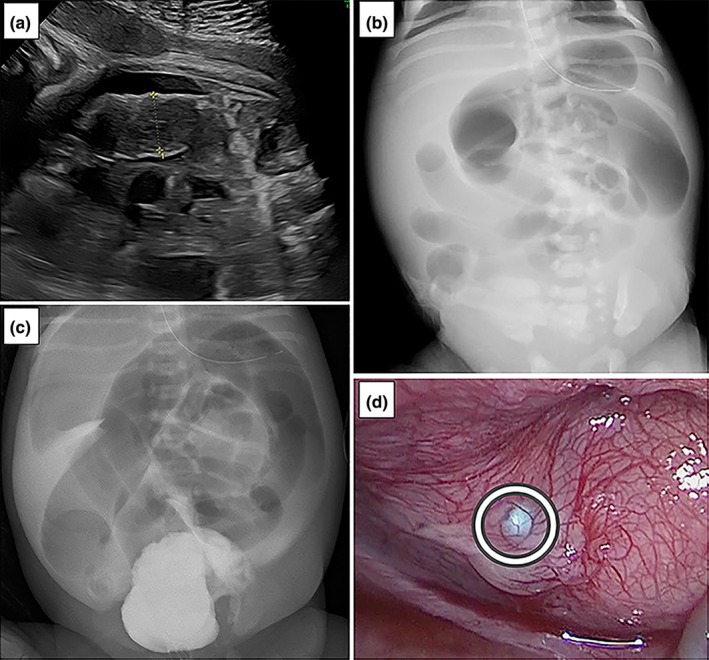 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrological Disorders and Treatments · Congenital gastrointestinal and neural anomalies
Neonatal bladder rupture is rare, and most previous cases have involved boys with urinary tract obstruction due to a posterior urethral valve.1 We report a case involving a girl with trisomy 21 who was noted to have ascites during the fetal period and was diagnosed with a ruptured bladder after birth. Informed consent was obtained from the parents.
The 43‐year‐old mother was referred to our hospital at 36 weeks of gestation due to fetal ascites and intestinal dilation, initially suspected to be meconium peritonitis. Ultrasound revealed low amniotic fluid levels (amniotic fluid index <1 cm), bilateral Grade 2 hydronephrosis, right hydroureter, bowel dilation (Figure 1a), and marked ascites. An emergency cesarean section was performed on the same day because of decreased fetal movement. A female infant was born weighing 2400 g, with Apgar scores of 6 at 1 min and 9 at 5 min. After birth, an imperforate anus was observed. X‐ray showed bowel dilation (Figure 1b). Retrograde cystography was performed on day 1. Following lower ureterography, contrast medium was observed leaking into the intraperitoneal space (Figure 1c), raising suspicion of a ruptured bladder. No fistula was found between the rectum, vagina, and urethra. A balloon catheter was placed to decompress the bladder. Surgery was performed to repair the imperforate anus and bladder rupture. The ascites was clear and pale yellow. A fragile bladder wall was observed on the left side of the bladder body (Figure 1d). When saline was injected into the bladder through a catheter, it leaked into the intraperitoneal space. The perforation was sutured, and anoplasty was performed. Biochemical examination of the ascites showed a blood concentration of urea nitrogen of 26.7 mg/dL and a creatinine concentration of 1.54 mg/dL, indicating that the ascites was urine. Blood tests showed no hyponatremia or hyperkalemia. After the urinary catheter was removed, sufficient spontaneous urination was maintained. On ultrasound, the hydroureter disappeared and the hydronephrosis improved to Grade 1. Magnetic resonance imaging revealed no abnormalities in the spine or spinal cord. Retrograde cystography on day 23 showed no vesicoureteral reflux. Trisomy 21 was diagnosed through chromosome analysis. No ascites recurrence was observed during hospitalization, and the patient was discharged on day 40.
Fetal ascites is uncommon, with 30% of cases originating from urinary causes.2 Neonatal bladder rupture is also very rare. There are several causes of bladder rupture, including urinary tract malformations, neurogenic bladder, and perforation by a catheter. Although various causes have been reported, most in the fetal to postnatal period are due to a posterior urethral valve; hence, most reported cases involve boys. Weller et al. reported a case of bladder rupture caused by urethral obstruction due to neuroblastoma.3 Chute et al. reported a bladder rupture adult case due to bowel dilatation from fecal embolism. They suggested pressure from nearby tissues caused thinning of the bladder, impairing blood flow and leading to perforation.4 Our case was a “covered anus complete”, in which the rectum is prone to dilatation because there is no fistula. In addition, it is difficult to diagnose an imperforate anus in a fetus, but in this case, the fetal ultrasound showed severe intestinal dilation. Based on these conditions, we thought, as in our case, pressure from severe rectal dilation caused urinary tract obstruction, leading to thinning of the bladder wall, impaired blood flow, and eventual rupture. Imaging and ascites examinations are useful for diagnosing bladder rupture. When ascites is detected, hydronephrosis and bladder wall thickness should be checked to differentiate bladder rupture. If the ascites is urine, biochemical tests will show low concentrations of protein and sodium and high blood concentrations of urea nitrogen, creatinine, and potassium. Blood tests will show similar trends because urine accumulating in the abdominal cavity acts as an auto‐dialysis agent.5 Severe hyponatremia and hyperkalemia sometimes occur. In our patient, the biochemical results of the ascites strongly indicated that the fluid was urine.
In summary, we report a girl with a trisomy 21 case whose bladder rupture was suspected to have been caused by urethral compression due to imperforate anus. If a patient suspected of having imperforate anus has ascites, clinicians should consider the possibility of bladder rupture due to increased pressure from imperforate anus.
AUTHOR CONTRIBUTIONS
NT was responsible for writing the manuscript. AT supervised the whole process, including treatment. TS was responsible for treating the patient. YS, YM, and RM critically reviewed the manuscript and contributed to the conception of this report. All authors read and approved the final manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tran H , Nguyen N , Nguyen T . Neonatal bladder rupture. Indian J Pediatr. 2009;76(4):427–429.19205633 10.1007/s 12098-009-0006-4 · doi ↗ · pubmed ↗
- 2Tank ES , Carey TC , Seifert AL . Management of neonatal urinary ascites. Urology. 1980;16(3):270–273.7423705 10.1016/0090-4295(80)90040-0 · doi ↗ · pubmed ↗
- 3Weller MH , Miller K . Unusual aspects of urine ascites. Radiology. 1973;109(3):665–669.4772183 10.1148/109.3.665 · doi ↗ · pubmed ↗
- 4Chute D , Cox J , Archer M , Bready RJ , Reiber K . Spontaneous rupture of urinary bladder associated with massive fecal impaction (fecaloma). Am J Forensic Med Pathol. 2009;30(3):280–283.19696587 10.1097/PAF.0b 013e 318187 e 085 · doi ↗ · pubmed ↗
- 5Oei J , Garvey PA , Rosenberg AR . The diagnosis and management of neonatal urinary ascites. J Paediatr Child Health. 2001;37(5):513–515.11885721 10.1046/j.1440-1754.2001.00656.x · doi ↗ · pubmed ↗