Role of functional mapping on Gallium-68 perfusion positron emission tomography and computed tomographic imaging (PET/CT) to assess the risk of long-term radiation-induced lung toxicity after stereotactic body radiation therapy
François Lucia, David Bourhis, Frédérique Blanc-Béguin, Gaëlle Goasduff, Mohamed Hamya, Simon Hennebicq, Maëlle Mauguen, Romain Floch, Margaux Geier, Ulrike Schick, Maëlys Consigny, Olivier Pradier, Grégoire Le Gal, Pierre-Yves Salaun, Vincent Bourbonne, Pierre-Yves Le Roux

TL;DR
This study shows that using functional imaging improves the prediction of long-term lung damage after radiation therapy for lung tumors.
Contribution
Functional dosimetric parameters from perfusion PET/CT outperform anatomical ones in predicting radiation-induced lung toxicity.
Findings
Functional parameters in FV50% and FV70% were significantly higher in patients with long-term RILT.
Anatomical and low functional volume parameters did not differ between patients with and without RILT.
Functional imaging could guide radiotherapy planning to reduce long-term toxicity risk.
Abstract
•SBRT is a real alternative treatment for inoperable lung tumors but remains associated with significant pulmonary toxicity.•Perfusion PET/CT imaging is a very attractive test for functional lung avoidance during radiotherapy planning.•This prospective study compare anatomical and functional dosimetric parameters to predict the risk of long-term RILT.•The predictive value of functional parameters outperforms the standard parameters for the risk of grade ≥2 long-term RILT.•Functional parameters could be useful to guide radiotherapy planning to reduce the risk of long-term RILT. SBRT is a real alternative treatment for inoperable lung tumors but remains associated with significant pulmonary toxicity. Perfusion PET/CT imaging is a very attractive test for functional lung avoidance during radiotherapy planning. This prospective study compare anatomical and functional dosimetric…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
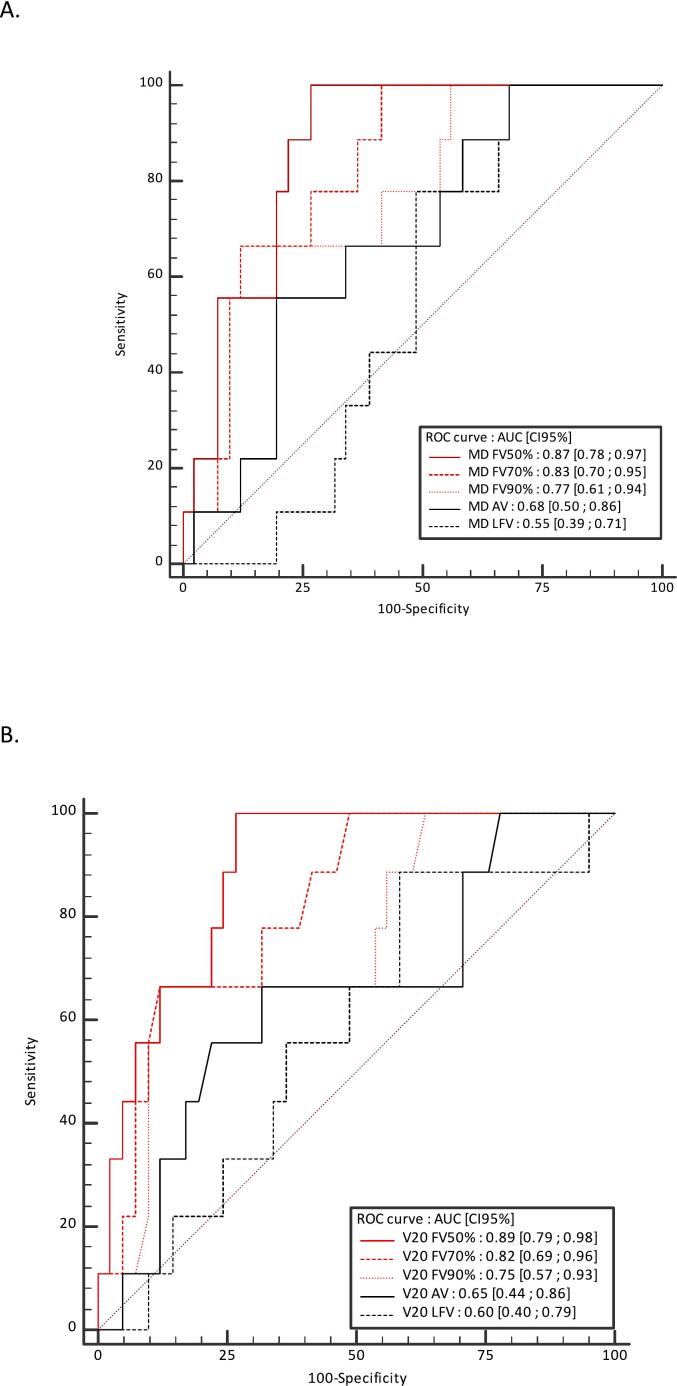 Figure 1
Figure 1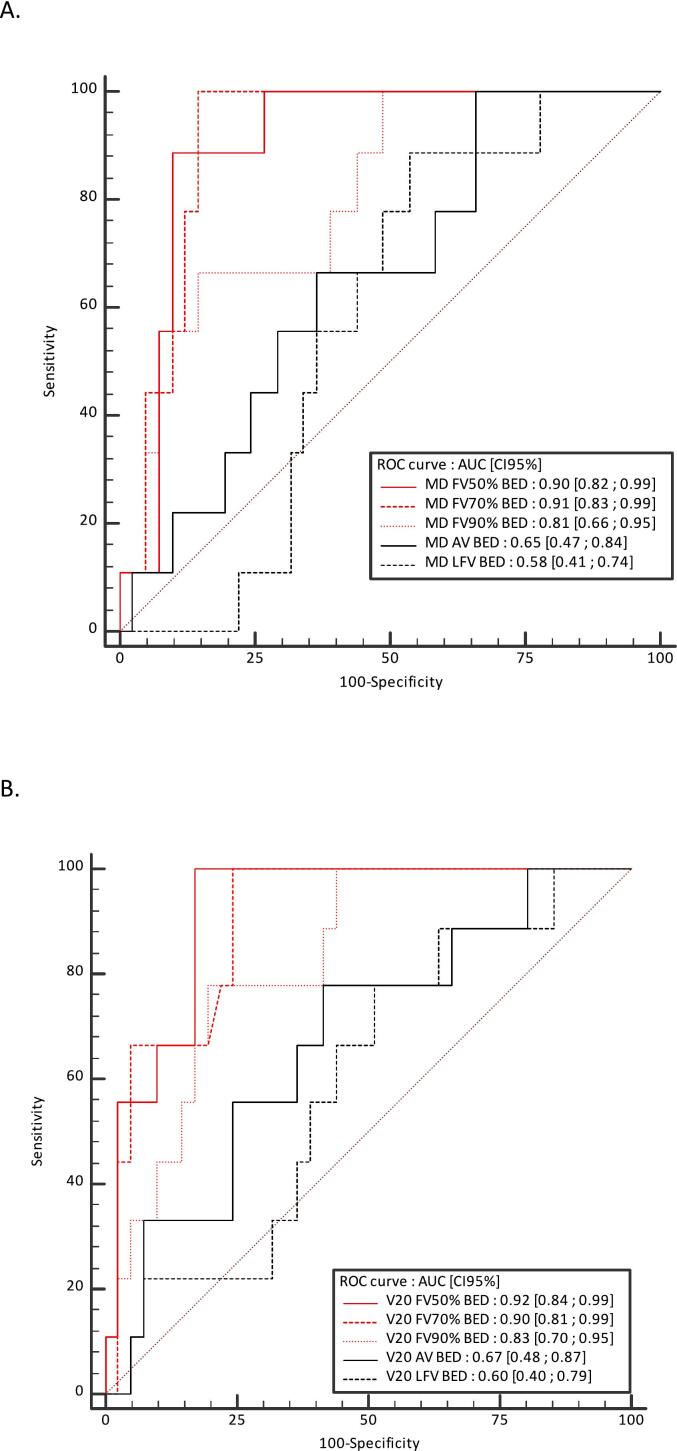 Figure 2
Figure 2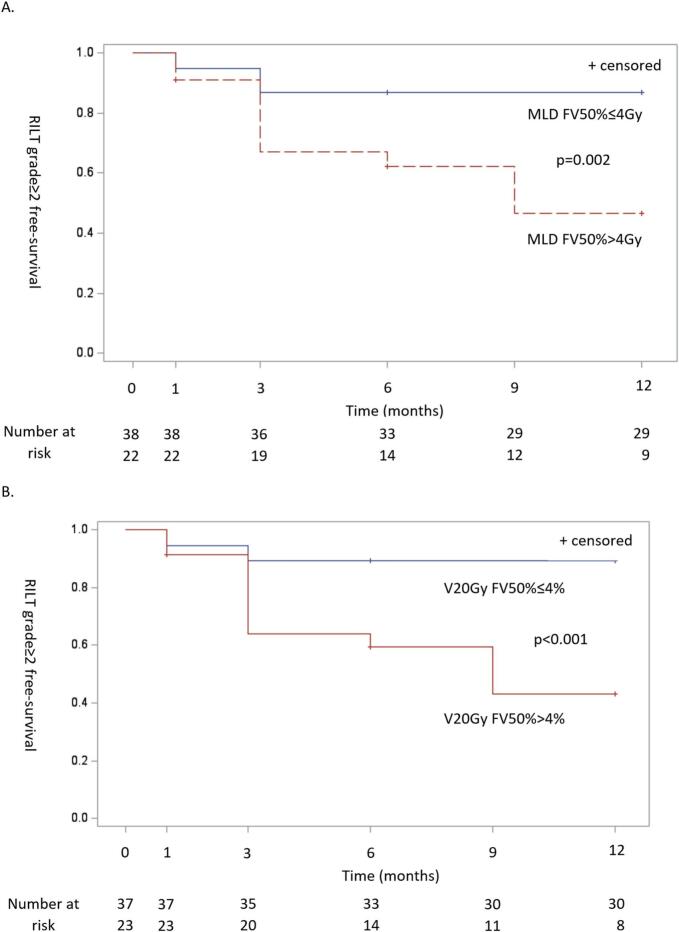 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Radiotherapy Techniques · Lung Cancer Diagnosis and Treatment · Medical Imaging Techniques and Applications
Introduction
1
Over recent years, stereotactic body radiotherapy (SBRT) has demonstrated efficacy in treating early-stage non-small cell lung cancer and lung metastases with less toxicity than conventionally fractionated RT [1,2]. Nevertheless, SBRT is still associated with a late radiation-induced lung toxicity (RILT) requiring medical intervention (grade ≥2 according to the National Cancer Institute Common Terminology Criteria for Adverse Events [CTCAE] version 5.0 grading scale) of the order of 15–20 % [3].
The prediction models in the literature used standard dosimetric parameters based on the anatomic lung. These models had moderate performance with Area under curve (AUC) values of 0.63 to 0.77 [4,5] indicating that the predictive accuracy needs to be improved. Development of an accurate prediction model for RILT is an important challenge [3].
Current treatment planning dosimetric constraints are applied on the anatomical lung volume defined on CT images, and simplistically assume that lung tissue is functionally homogeneous. However, multiple studies have now demonstrated that patients’ lung function is spatially heterogeneous, especially in patients with lung tumors due to tumor or tobacco-related comorbidities [6,7]. Thus, despite respect of standard lung dose constraints, the RILT rate remains significant [3].
One strategy for mitigating RILT could be to preferentially spare the radiation dose to highly functional regions of the lung. Various imaging techniques have been proposed for lung functional mapping and radiotherapy planning. The majority of studies used perfusion single-photon emission computed tomography (SPECT) imaging and demonstrated the ability of functional lung optimized planning techniques to spare regions of functional lung. However, the predictive value of functional dose-volume parameters based on SPECT images on RILT has not been clearly demonstrated [8].
Lung perfusion positron emission tomography and computed tomographic imaging (PET/CT) is an emerging modality for regional lung function assessment [[9], [10], [11]]. As compared with conventional lung scintigraphy, ^99m^Tc is substituted with ^68^Ga to label Macro aggregated albumin (MAA) particles. PET/CT is a vastly superior technology for image acquisition, with an approximately 100 times higher sensitivity, higher spatial resolution (3–4 mm with PET compared with 15 mm with SPECT), and greater access to respiratory-gated acquisition [12,13].
In a previous analysis, we found that the predictive value of PET perfusion-based functional parameters outperforms the standard CT-based dose volume parameters for the risk of grade ≥2 acute RILT [14]. However, RILT is generally divided into an acute phase (acute RILT), within 3–6 months after RT, often referred to as radiation-induced pneumonitis, and a late phase (long-term RILT), often referred to as radiation-induced pulmonary fibrosis, which is a chronic toxicity with a long-term impact on the patient's quality of life [15].
The aim of this analysis was to compare the performance of anatomic and functional dosimetric parameters based on lung perfusion PET/CT imaging to predict the risk of symptomatic long-term RILT in patients with lung tumors treated with SBRT.
Material and methods
2
Study design and participants
2.1
The PEGASUS trial is a single-center prospective study [16]. The eligible study population consisted of patients aged >18 years planned to be treated in the radiotherapy department of our institute, with SBRT for primary or secondary lung tumors. Exclusion criteria included the inability to give informed consent, patients under guardianship or curatorship, pregnant or breastfeeding women, and contra-indication to the administration of human albumin macroaggregates. The study was approved by the Nord Ouest IV Ethics Committee (ID RCB: 2021-002224-20) and registered in ClinicalTrial.gov registry (NCT04942275). Written informed consent was obtained from all participants.
Radiation therapy
2.2
A respiratory-sorted 4-dimensional computed tomography (4DCT) data set was generated using the planning CT (Siemens, Somatom) coupled with Varian real-time position management (RPM) gating system (Varian Medical Systems, Palo Alto, CA, United States). From the respiratory-sorted image phases, average (AVG) and maximum intensity projection (MIP) series were reconstructed. The internal target volume was delineated on the basis of a four-dimensional planning CT scan to take account for tumour motion on a MIM Maestro v7.2.3 (MIM Software, Cleveland, Ohio, USA) workstation. The internal target volume (ITV) was expanded 3 mm in all plans to create the planning target volume (PTV). Treatment plan was performed on the Pinnacle V16.2 planning system (Philips Medical Systems (Cleveland), Inc.) using the AVG series. Treatment was planned and delivered with modulated arc therapy (VMAT) using a TrueBeamTM STX 2.0 linac linear accelerator (Varian Medical Systems, Palo Alto, CA, United States) equipped with Varian RPM gating system with a prescription dose of 48 to 60 Gy in 3 to 8 fractions depending on proximity to organs at risk (OAR) [14] (Supplemental data A). As per the protocol of this pilot study, and given that doses to the target volume and the OARs were respected, either the anatomical plan or functional plan could be delivered to the patient.
Lung perfusion PET/CT
2.3
All patients underwent lung perfusion PET/CT scan acquired on a digital Biograph Vision 600 PET/CT scanner (Siemens Healthineers, Knoxville, TN, United States) [16] (Supplemental data A).
The lung volumes were delineated using MIM Maestro v7.2.3 (MIM Software, Cleveland, Ohio, USA). An automatic contouring of the whole lung anatomical volume (AV) was initially performed based on Hounsfield unit value and then visually adjusted to match normal contours if required. Within the AV, three lung functional volumes were defined using an automated relative to whole lung function segmentation method, delineating the minimal volume containing 50 % (FV50%), 70 % (FV70%) and 90 % (FV90%) of the total activity within the AV, respectively [17]. We also defined a low functional lung volume (LFV) as follows: LFV = AV-FV90% (approximately 25 % of the AV containing 10 % of lung function [17].
PET/CT and planning CT registration
2.4
Functional volumes were defined on PET, and AV was defined the CT component of PET (CT_PET_), then all volumes were stored associated with CT_PET_ in DICOM RT-STRUCT format. Dose distribution map was associated with the average of planning 4DCT (AVG) in DICOM RT-DOSE format. Second, AVG and CT_PET_ were registered, with a rigid followed by a deformable registration using MIM Maestro v7.2.3 (MIM Software, Cleveland, Ohio, USA) and the VoxAlign Deformation Engine, a constrained, intensity based free-form deformable registration algorithm [18,19], in order to take into account differences in terms of respiratory cycle. Finally, lung functional volumes and AV were transferred to AVG, allowing optimization to lung volumes and dose-volume analysis.
End-point: RILT evaluation
2.5
RILT was assessed prospectively by a radiation oncologist, without access to dose statistics for the functional pulmonary volume, every 3 months until 12 months after completion of SBRT, based on clinical and imaging evaluation according to NCI CTCAE version 5.0 (pneumonitis or fibrosis) [3,20].
The main endpoint of the present analysis was grade ≥2 long-term RILT at 12 months as assessed with NCI CTCAE version 5.0 [3,20].
Statistical analysis
2.6
Clinical parameters included in the analysis were age, sex, Eastern Cooperative Oncology Group (ECOG) performance status (PS), smoking history including pack-years, histology (primary vs secondary), tumor volume, spirometry including forced expiratory volume in one second (FEV1) and diffusion capacity of the lung for carbon monoxide (DLCO).
Dosimetric parameters included dose fractionation, dose received by 99 % volume of PTV (D99%), PTV maximum dose (DPTVmax), PTV minimum dose (DPTVmin) and PTV mean dose (DPTVmean), mean dose (MD) to lung volume, percentage volume of lung getting 5 to 30 Gy dose (Vx) in 5-Gy increments.
MD and percentage of volume getting 5 to 30 Gy dose (VxFVy) were extracted from five lung volumes: the AV, three lung functional volumes (FV50%, FV70%, FV90) and the LFV. We also reported the Biologically Effective Dose (BED), using the formula BED = D x (1 + [d/(α/β)]), where variables are as follows: d = Dose per fraction, in Gy, D = Total dose (number of fractions x dose per fraction), in Gy, and α/β ratio = 3 Gy for the lungs.
Population characteristics were compared between RILT and non-RILT groups by Wilcoxon tests for quantitative variables and by Fisher's Exact tests for qualitative variables. The Wilcoxon test was also used to compare dose-volume parameters between RILT and non-RILT groups. The area under the curve (AUC) of each ROC curve for the five lung volumes as predictors of RILT (AV, FV50%, FV70%, FV90%, LFV) was calculated.
We also performed a time dependent analysis, using Kaplan-Meier curves, of the probability of grade ≥2 RILT occurrence between groups classified as high risk and low risk defined according to cutoff values obtained with Younden indices of previous ROC curves. In this analysis, patients lost to follow-up or who died are censored. Analyses were performed using SAS 9.4. Multivariate statistical tests were not performed due to the small sample size and low number of patients experiencing toxicity. However, we performed statistical significance adjustment, due to multiple testing, using the Benjamin-Hochberg false discovery rate (FDR) procedure with a threshold adjusted p-value of 5 %.
Results
3
Study population
3.1
Between July 2021 and January 2022, 60 consecutive patients who consented to participate in the study and met inclusion criteria with primary or secondary lung tumors were enrolled into this prospective study. Lung SBRT was not performed in one patient with NSCLC due to a brain progression of the disease, for which systemic treatment was initiated. Out of the 59 patients, 50 patients were alive at 12 months. Patient characteristics and dose target volumes are presented in Table 1.Table 1. Patient characteristics.**Total(N = 50)**Grade 0–1(N = 41)****Grade ≥ 2(N = 9)P valueAdjusted P valueAgeNo. (No. missing)50 (0)41 (0)9 (0)0.550.65Median (q1;q3)69.5 (63.0;72.0)68.0 (63.0;72.0)71.0 (63.0;75.0)GenderMale25 (50 %)18 (44 %)7 (78 %)0.140.24Female25 (50 %)23 (56 %)2 (22 %)TobaccoMissing4 (8 %)3 (7 %)1 (11 %)0.160.26Active smoker13 (28 %)13 (34 %)0 (0.0 %)Former smoker21 (46 %)16 (42 %)5 (62 %)Non smoker12 (26 %)9 (24 %)3 (38 %)Pack-years smokingNo. (No. missing)28 (22)26 (15)2 (7)0.430.55Median (q1;q3)40.0 (20.0;57.5)40.0 (20.0;60.0)30.0 (20.0;40.0)Asbestos exposureMissing6 (12 %)6 (15 %)0 (0 %)0.570.65No39 (89 %)30 (86 %)9 (100 %)Yes5 (11 %)5 (14 %)0 (0 %)WeightN (N missing)45 (5)37 (4)8 (1)0.240.35Median (q1;q3)60.0 (56.0;79.0)59.0 (54.0;76.0)73.5 (58.0;93.5)Performance statusN (N missing)48 (2)39 (2)9 (0)0.981.00Median (q1;q3)1.0 (0.0;1.0)1.0 (0.0;1.0)0.0 (0.0;1.0)COPDNo35 (70 %)28 (68 %)7 (78 %)0.710.77Yes15 (30 %)13 (32 %)2 (22 %)AsthmaNo47 (94 %)39 (95 %)8 (89 %)0.460.57Yes3 (6 %)2 (5 %)1 (11 %)Previous pulmonary embolismNo46 (92 %)37 (90 %)9 (100 %)1.001.00Yes4 (8 %)4 (10 %)0 (0 %)Other(s) comorbiditie(s)No6 (12 %)5 (12 %)1 (11 %)1.001.00Yes44 (88 %)36 (88 %)8 (89 %)Thoracic surgeryNo36 (72 %)28 (68 %)8 (89 %)0.410.54Yes14 (28 %)13 (32 %)1 (11 %)LocalizationCentral6 (12 %)5 (12 %)1 (11 %)1.001.00Peripheral44 (88 %)36 (88 %)8 (89 %)ITV volume in ccMedian (q1;q3)5.9 [3.0; 9.9]5.9 [2.8; 9.9]5.9 [3.5; 9.0]0.710.77PTV volume in ccMedian (q1;q3)12.9 [8.2; 21.3]13.1 [8.1; 21.6]12.6 [9.9; 20.5]0.760.80SBRT dose54 Gy18 (36 %)16 (39 %)2 (22 %)0.480.5948 Gy60 Gy26 (52 %)6 (12 %)20 (49 %)5 (12 %)6 (67 %)1 (11 %)Abbreviations: COPD = chronic obstructive pulmonary disease; SBRT = stereotactic body radiation therapy.
Toxicity
3.2
Out of the 50 patients, 9 (18 %) had grade ≥ 2 long-term RILT according to the CTCAE version 5.0 criteria. 45 (76 %) patients had some nonspecific radiological changes on CT scan. Two (4 %) patient developed grade 3 long-term RILT. There were no deaths attributed to RILT. No patient had a rib fracture or thoracic pain. Other symptom reported by the patients were asthenia in 3 (6 %) patients, all grade 1.
Comparison of dosimetric parameters in patients with and without long-term RILT
3.3
Dosimetric parameters in patients with and without long-term RILT are presented in Tables 2 and S1.Table 2. Dosimetric parameters.Total (N = 50)Median IQRGrade 0–1 (N = 41)Median IQRGrade ≥ 2 (N = 9)Median IQRP value****Adjusted p valueMD AV (Gy)2.9 (2.0;4.3)2.8 (1.9;3.8)4.3 (2.5;4.6)0.100.20MD LFV (Gy)2.3 (1.0;4.3)2.6 (0.9;4.4)2.1 (1.2;2.5)0.650.73MD FV50% (Gy)3.1 (1.6;4.2)2.7 (1.4;3.7)4.8 (4.1;5.5)0.0010.006MD FV70% (Gy)3.1 (1.9;4.1)2.7 (1.8;3.8)4.8 (3.7;5.6)0.0040.013MD FV90% (Gy)2.8 (2.1;4.5)2.8 (1.8;3.6)4.8 (3.1;5.3)0.0140.031MD AV (Gy) BED7.6 (6.0;11.3)7.5 (5.4;10.2)9.5 (6.8;11.4)0.160.26MD LFV (Gy) BED5.9 (1.8;11.4)6.2 (1.8;11.7)4.1 (2.8;6.2)0.480.59MD FV50% (Gy) BED6.2 (3.4;11.3)5.6 (3.0;9.3)14.3 (11.6;16.7)<0.0010.005MD FV70% (Gy) BED7.4 (4.9;10.2)6.5 (4.1;8.3)12.2 (10.5;16.6)<0.0010.005MD FV90% (Gy) BED8.1 (5.3;9.8)7.1 (4.3;9.0)12.3 (8.2;15.1)0.0060.017V5Gy AV (%)13.6 (9.7;20.4)12.4 (9.1;18.4)15.8 (12.6;23.3)0.140.24V5Gy LFV (%)9.6 (3.7;22.1)10.1 (3.7;22.1)8.3 (5.9;14.7)0.730.77V5Gy FV50% (%)16.1 (8.7;21.3)12.5 (6.6;18.7)23.2 (17.8;25.3)0.0080.022V5Gy FV70% (%)14.4 (10.2;20.0)12.8 (9.4;17.9)24.0 (15.5;30.1)0.0090.022V5Gy FV90% (%)14.0 (10.2;18.6)13.3 (10.0;17.3)24.1 (13.4;27.4)0.0310.066V5Gy AV (%) BED15.9 (12.5;22.5)15.6 (11.6;21.3)16.3 (15.5;28.0)0.210.33V5Gy LFV (%) BED13.7 (4.2;24.2)13.7 (4.2;24.3)13.7 (9.1;15.5)0.730.77V5Gy FV50% (%) BED13.1 (7.6;23.4)10.2 (7.4;19.9)26.0 (21.6;29.3)0.0020.009V5Gy FV70% (%) BED13.8 (9.1;22.9)11.6 (8.9;19.4)25.6 (19.5;28.6)0.0020.009V5Gy FV90% (%) BED15.5 (9.5;21.1)13.9 (9.3;19.5)23.9 (17.5;30.6)0.0080.022V20Gy AV (%)3.0 (2.0;5.1)2.7 (2.0;4.7)5.1 (2.2;6.6)0.180.28V20Gy LFV (%)2.6 (0.4;5.8)2.8 (0.4;5.8)0.6 (0.3;3.4)0.380.50V20 Gy FV50% (%)3.5 (1.2;4.9)2.2 (1.0;3.9)6.4 (4.7;8.9)<0.0010.005V20 Gy FV70% (%)3.4 (1.4;5.6)2.8 (1.3;4.2)6.8 (4.0;8.2)0.0040.013V20 Gy FV90% (%)3.4 (1.7;5.1)3.2 (1.5;4.6)6.9 (2.9;7.5)0.0260.057V20Gy AV (%) BED6.8 (4.7;10.7)6.7 (4.6;9.2)9.7 (7.1;14.2)0.110.21V20Gy LFV (%) BED6.0 (1.4;11.1)6.4 (1.4;11.3)3.3 (1.4;7.1)0.380.50V20 Gy FV50% (%) BED5.5 (2.5;9.9)5.1 (2.3;6.6)12.4 (9.7;16.7)<0.0010.005V20 Gy FV70% (%) BED6.0 (3.5;9.2)5.4 (3.4;7.7)11.9 (9.0;13.2)<0.0010.005V20 Gy FV90% (%) BED6.8 (4.0;9.7)5.6 (3.5;7.7)10.2 (9.2;13.8)0.0040.013Abbreviations: AV = anatomic volume; BED = biologically effective dose; EQD2 = equivalent dose in 2-Gy fractions; FV = functional volume; LFV = low functional volume; MD = mean dose; VxGy = percentage of lung volumes receiving xGy.
After FDR adjustment, median (IQR) MD in the AV and LFV volumes were not statistically different in patients with and without long-term RILT with p = 0.20 and p = 0.73, respectively. In contrast, median MD was significantly higher in the FV50%, FV70% and FV90% volumes in patients with long-term RILT with p = 0.006, p = 0.013 and p = 0.031, respectively.
After FDR adjustment median V20Gy in the AV and LFV volumes were not statistically different in patients with and without long-term RILT with p = 0.28 and p = 0.50, respectively. In contrast, median V20Gy was significantly higher in the FV50% and FV70% volumes, but not in the FV90% volume, in patients with long-term RILT, with p = 0.005, p = 0.013 and p = 0.057, respectively.
The results in BED were slightly higher (See Tables 2 and S1).
Among the clinical characteristics tested, none was found to be significantly higher in patients with long-term RILT grade ≥2 (Table 1).
ROC curves assessing the ability of the MD AV, LFV, FV50%, FV70% and FV90% and V20 AV, LFV, FV50%, FV70% and FV90% to discriminate between patients with and without long-term symptomatic RILT are shown in Fig. 1, Fig. 2. AUCs (CI 95 %) for MD AV, LFV, FV50%, FV70% and FV90% were 0.68 (0.50–0.86), 0.55 (0.39–0.71), 0.87 (0.78–0.97), 0.83 (0.70–0.95), 0.77 (0.61–0.94), respectively. AUCs for V20Gy AV, LFV, FV50%, FV70% and FV90% were 0.65 (0.44–0.86), 0.60 (0.40–0.79), 0.89 (0.79–0.98), 0.82 (0.69–0.96), 0.75 (0.57–0.93), respectively. The results in BED were slightly higher (See Fig. 2).Fig. 1. Receiver operating characteristic (ROC) curves to assess the ability of the mean dose (A) and V20Gy (B) of anatomic volume (AV), low functional volume (LFV), and the minimal volume containing 50% (FV50%), 70% (FV70%), and 90% (FV90%) of the total activity within the AV to discriminate between patients with and without long-term symptomatic radiation-induced lung toxicity. Abbreviations: AUC = area under the curve; MD = mean dose.Fig. 2. Receiver operating characteristic (ROC) curves to assess the ability of the mean dose (A) and V20Gy (B) in biologically effective dose (BED) of anatomic volume (AV), low functional volume (LFV), and the minimal volume containing 50% (FV50%), 70% (FV70%), and 90% (FV90%) of the total activity within the AV to discriminate between patients with and without long-term symptomatic radiation-induced lung toxicity. Abbreviations: AUC = area under the curve; MLD = mean dose.
Time-dependent analysis of the occurrence of grade ≥2 RILT
3.4
Based on ROC analysis, MD FV50% and V20 FV50% were the most predictive parameters of long term RILT. The most discriminant values of functional dosimetric parameters to separate patients with low- or high-risk grade ≥2 RILT occurrence were 4 Gy for MD FV50% and 4 % for V20Gy FV50%, respectively. Time-dependant analysis of the occurrence of grade ≥2 RILT were significantly different for MD and V20Gy FV50% (p = 0.002 and p < 0.001, respectively) and are presented in Fig. 3.Fig. 3. Risk of ≥grade 2 radiation-induced lung toxicity according to (A) MD FV50% (cut-off of 4 Gy) and (B) V20Gy FV50% (cut-off of 4 %) over time.
Discussion
4
In this prospective study, functional dose parameters based on lung perfusion PET/CT imaging outperformed anatomical lung parameters to predict the risk of long-term RILT grade ≥2 after SBRT.
The incidence of symptomatic grade ≥2 long term RILT in our study (18 %) was in line with that of the published literature, which is around 15–20 % [3,21,22]. Because of the difficulty in differentiating radiation pneumonitis and fibrosis on the basis of clinical and imaging findings [23,24], they are referred to as acute or long term « radiation-induced lung toxicity.
It is important to note that the presence or absence of acute RILT at 3 months does not allow to prejudge the presence of long term RILT. In our study, of the 10 patients with grade ≥2 long-term RILT, 3 had no acute toxicity at 3 months. In contrast, 3 patients with acute RILT and evaluable at 12 months had no long term toxicity, with regression of their symptoms after treatment with corticosteroids. Our result underlines the difference between acute and long-term RILT, and the need to improve prediction of long-term toxicity with the risk of sequelae for the patient. Although corticosteroids are the cornerstone of the clinical management of radiation pneumonitis, advanced knowledge of the molecular mechanisms underlying lung injury has led to the development of other promising pharmaceuticals to treat radiation fibrosis [25,26]. As long-term use of corticosteroids can have adverse side effects and are inefficient, the prediction of long-term RILT using a non-invasive tool is clinically significant to allow prevention or earlier and more appropriate therapeutic management.
Functional lung avoidance radiotherapy planning is an emerging concept to reduce the RILT [6,8]. In our study, all dose volume parameters were significantly higher in the FV50% and FV70% volumes in patients with long-term RILT (p < 0.05). In contrast, no significant difference was observed with the AV and the LFV. Furthermore, AUCs of MD and V20Gy in all FV were between 0.75 and 0.89 vs 0.65 to 0.68 in the AV and 0.55 to 0.58 in LFV. No significant differences were observed between the anatomical (7/43 with RILT grade ≥2) and functional (2/7 with RILT grade ≥2) plans groups. This finding could be attributed to a limited sample size and optimization that was not guided by established dose constraints on functional lung volumes.
This analysis confirmed our previous results at 3 months [14]. FV70% and FV50% are the two functional volumes that are most predictive of grade 2 or higher acute and late RILT. These two functional volumes seem to have a better predictive power for late toxicity compared to acute RILT, with AUCs of approximately 0.9 for late toxicity versus 0.8 for acute toxicity. The optimal cut-off values to distinguish patients at high risk of acute or late RILT are, for the mean dose to FV50% and FV70%, 3 Gy in physical dose and 11 Gy and 9 Gy in BED, respectively. As outlined in a recent systematic review and meta-analysis on functional lung avoidance radiotherapy [8], no study had previously demonstrated a statistically significant better predictive value of functional versus anatomical lung volumes for RILT risk [8]. We adopted a different methodology on several points. First, we assessed patients treated with SBRT while all previous studies were performed in patients treated with conventional RT. Second, we used PET rather than SPECT imaging for lung functional volume mapping. PET/CT is a vastly superior technology for image acquisition, with an approximately 100 times higher sensitivity, higher spatial resolution, and greater access to respiratory-gated acquisition [9,10], allowing a more precise functional lung volumes mapping and a better co-registration with radiation plans. Third, we used an automated relative to whole lung function threshold segmentation method for lung functional volumes delineation. This delineation method provides reliable and reproducible functional lung volumes, and is clinically meaningful to clinicians [17].
ROC curves analysis provides insight on the potential use of lung perfusion PET/CT images for lung avoidance SBRT planning. For instance, the rate of grade ≥2 RILT was 3.0 % in patients with MD in the FV50% <4 Gy, as compared with 47.1 % for patients with MD in the FV50% >4 Gy. The rate of grade ≥2 RILT was 3.1 % in patients with V20 FV50% <4%, as compared with 44.4 % in patients with V20 FV50% >4%. All functional parameters were able to separate patients at high versus low risk of developing grade ≥2 RILT over time, allowing a personalized optimization of radiation treatment planning according to the individual heterogeneity of regional lung function distribution. Moreover, the low functional lung volume was not predictive of long-term symptomatic RILT, opening up perspectives for further adaptation of radiation plans by irradiating these areas to better spare the functional lung volumes.
Our study has several limitations. Firstly, in this pilot study whose primary aim was to assess the feasibility of adapting the radiotherapy treatment plan to lung functional volumes, the number of patients was relatively small. The low power may explain why no statistical difference was observed in dose volumes parameters in the anatomical volumes. However, functional lung dose parameters based on lung perfusion PET/CT imaging clearly outperformed anatomical lung parameters to predict the risk of long-term RILT grade ≥2. Secondly, changes in pulmonary function testing (PFT) and impact on QoL were not available for the majority of patients. These changes would be interesting to analyze in a future trial in view of the results of previous studies [27,28]. Finally, there is a potential bias due to the challenge of differential diagnosis between RILT vs. progression of COPD or neoplasia.
Strengths of the study include the prospective design, with PET/CT scans systematically performed before initiation of SBRT. All patients had a close monitoring and follow up. RILT gradation was performed blindly, using the National Cancer Institute Common Terminology Criteria for Adverse Events, a widely accepted tool used for RILT evaluation.
In conclusion, functional dose parameters based on lung perfusion PET/CT outperformed standard CT parameters to predict the risk of long-term RILT grade ≥2 after lung SBRT. Functional lung avoidance planning may be a simple and non-invasive method to reduce radiation-induced lung sequelae, while delivering an optimal dose to the tumor and preserving others organs at risk. Randomized trials are now needed to determine whether a functional planning is superior to a conventional anatomical planning to reduced radiation-induced lung toxicity.
Consent to participate
8
The study was approved by the Nord Ouest IV Ethics Committee (ID RCB: 2021-002224-20) and registered in ClinicalTrial.gov registry (NCT04942275). Written informed consent was obtained from all participants.
Author contribution
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by François Lucia and Pierre-Yves Le Roux. The first draft of the manuscript was written by François Lucia and Pierre-Yves Le Roux and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics approval
All procedures were performed in accordance with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study design and exemption from informed consent were approved by the Institutional Review Board of Brest University Hospital.
Funding
This study received funding from “la ligue contre le cancer” (CD29 and CD22). The sponsor had no role in the design, analysis, or interpretation of the results.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ball D.Mai G.T.Vinod S.Babington S.Ruben J.Kron T.Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): a phase 3, open-label, randomised controlled trial Lancet Oncol 20201949450310.1016/S 1470-2045(18)30896-930770291 · doi ↗ · pubmed ↗
- 2Milano M.T.Katz A.W.Zhang H.Okunieff P.Oligometastases treated with stereotactic body radiotherapy: long-term follow-up of prospective study Int J Radiat Oncol Biol Phys 83201287888610.1016/j.ijrobp.2011.08.03622172903 · doi ↗ · pubmed ↗
- 3Kong (Spring)F.-M.Moiseenko V.Zhao J.Milano M.T.Li L.Rimner A.Organs at risk considerations for thoracic stereotactic body radiation therapy: what is safe for lung parenchyma?Int J Radiat Oncol Biol Phys 110202117218710.1016/j.ijrobp.2018.11.02830496880 PMC 9454379 · doi ↗ · pubmed ↗
- 4Saha A.Beasley M.Hatton N.Dickinson P.Franks K.Clarke K.Clinical and dosimetric predictors of radiation pneumonitis in early-stage lung cancer treated with Stereotactic Ablative radiotherapy (SABR) - An analysis of UK’s largest cohort of lung SABR patients Radiother Oncol 156202115315910.1016/j.radonc.2020.12.01533333139 · doi ↗ · pubmed ↗
- 5Liu Y.Wang W.Shiue K.Yao H.Cerra-Franco A.Shapiro R.H.Risk factors for symptomatic radiation pneumonitis after stereotactic body radiation therapy (SBRT) in patients with non-small cell lung cancer Radiother Oncol 156202123123810.1016/j.radonc.2020.10.01533096168 · doi ↗ · pubmed ↗
- 6Siva S.Devereux T.Ball D.L.Mac Manus M.P.Hardcastle N.Kron T.Ga-68 MAA Perfusion 4D-PET/CT scanning allows for functional lung avoidance using conformal radiation therapy planning Technol Cancer Res Treat 15201611412110.1177/153303461456553425575575 · doi ↗ · pubmed ↗
- 7Le Roux P.-Y.Leong T.L.Barnett S.A.Hicks R.J.Callahan J.Eu P.Gallium-68 perfusion positron emission tomography/computed tomography to assess pulmonary function in lung cancer patients undergoing surgery Cancer Imaging 1620162410.1186/s 40644-016-0081-527544383 PMC 4992565 · doi ↗ · pubmed ↗
- 8Bucknell N.W.Hardcastle N.Bressel M.Hofman M.S.Kron T.Ball D.Functional lung imaging in radiation therapy for lung cancer: a systematic review and meta-analysis Radiother Oncol 129201819620810.1016/j.radonc.2018.07.01430082143 · doi ↗ · pubmed ↗