Complete remission in PD-L1 high expression advanced gastric cancer patient with PD-L1 immunotherapy and chemotherapy integration treatment strategy: a case report
Xiaopeng Yu, Wenwen Zhao, Qingqing Feng, Jin Tian, Lili Zhao, Jun Xiao, Hongmei Wei

TL;DR
A patient with advanced gastric cancer achieved complete remission with PD-L1 immunotherapy and chemotherapy but later died from severe side effects.
Contribution
This case report highlights the potential and risks of combining PD-L1 immunotherapy with chemotherapy in PD-L1 high gastric cancer.
Findings
The patient achieved complete remission after PD-L1 immunotherapy and chemotherapy.
The treatment was associated with severe adverse events, including fatal complications from diarrhea.
High PD-L1 expression correlated with improved clinical outcomes in this case.
Abstract
Immune checkpoint inhibitors (ICIs) have become the standard of care in treating patients with human epidermal growth factor receptor 2(HER2) negative gastric cancer, revolutionizing the treatment landscape. The combination of ICIs and chemotherapy has shown improved treatment efficacy and prolonged survival compared to chemotherapy alone. Despite these benefits, this combined treatment is also linked to a higher incidence of adverse events. In this report, we present a case that demonstrates exceptional therapeutic efficacy but also severe adverse reactions. In HER2-negative gastric cancer, patients with higher programmed death-ligand1 (PD-L1) expression demonstrate improved clinical outcomes compared to those with lower PD-L1expression. This case study presents a 66-year-old male diagnosed with stage IV poorly differentiated gastric adenocarcinoma, characterized by hepatogastric…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
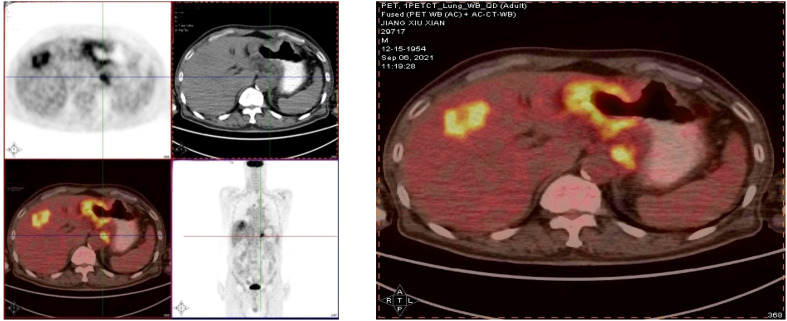 Figure 1
Figure 1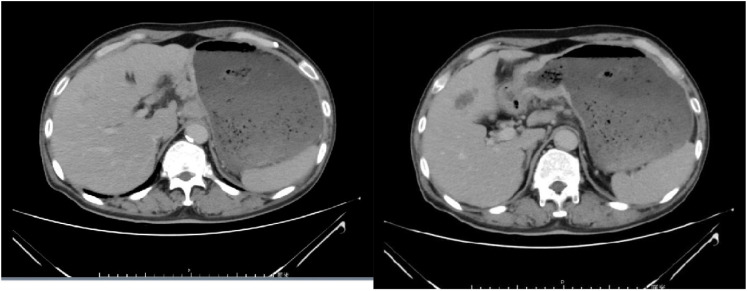 Figure 2
Figure 2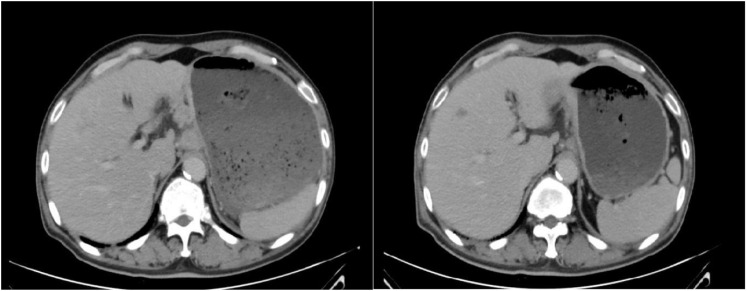 Figure 3
Figure 3 Figure 4
Figure 4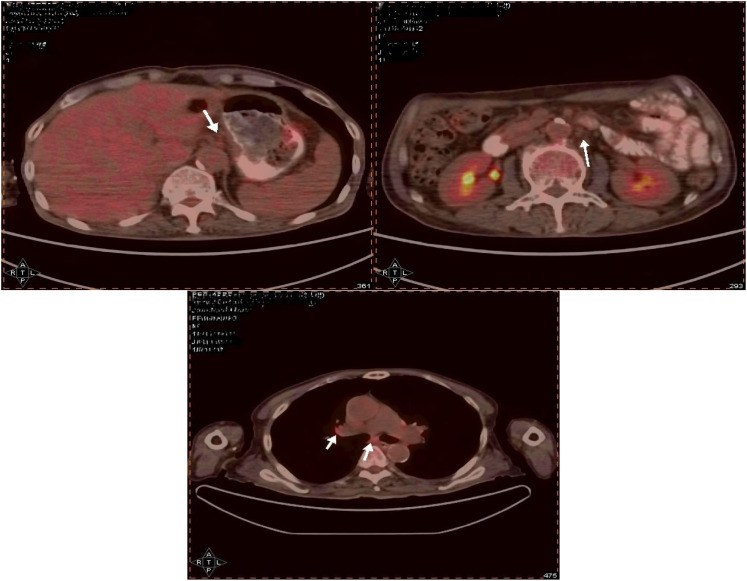 Figure 5
Figure 5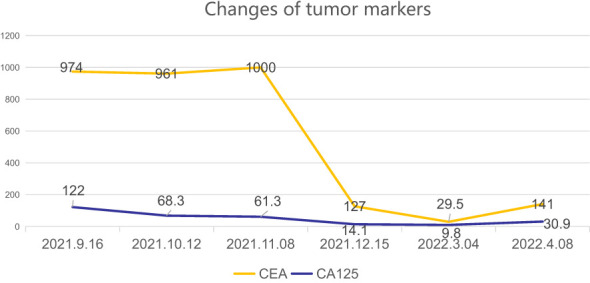 Figure 6
Figure 6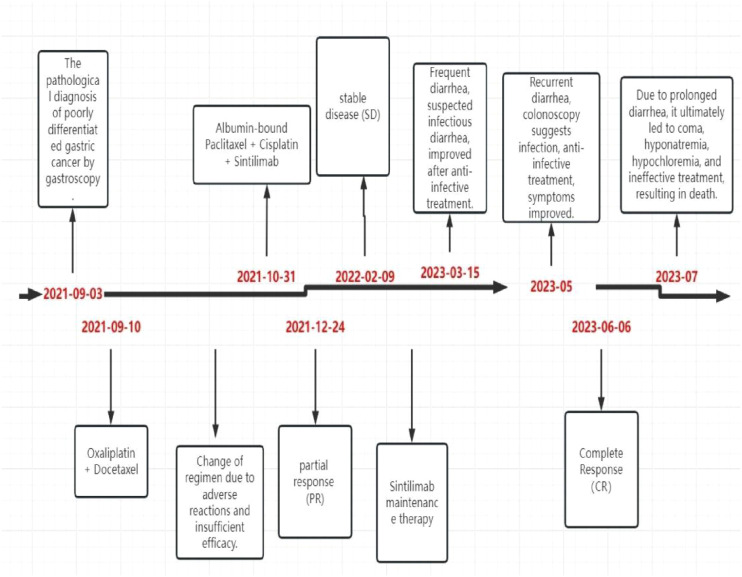 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Cancer Immunotherapy and Biomarkers
Introduction
1
Gastric cancer is a highly malignant cancer and ranks as the second leading cause of cancer-related deaths worldwide (1, 2). Recently, immune checkpoint blockade has become a promising strategy for cancer treatment, with monoclonal antibodies targeting programmed cell death protein 1 (PD- 1), PD-L1, and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4). In the context of treating advanced HER2-negative gastric cancer, the combination of immune checkpoint inhibitors with chemotherapy has shown significant survival benefits in terms of overall survival (OS) and progression-free survival (PFS) (3). The Rationale 305 trial revealed that tislelizumab plus chemotherapy led to a notable improvement in OS (HR 0.74 [95% CI: 0.59-0.94], median OS 17.2 vs 12.6 months; one-sided P = 0.0056) with manageable safety (4). Similarly, the ORIENT- 16 trial demonstrated that the use of immune therapy alongside chemotherapy in patients with CPS≥5 gastric adenocarcinoma resulted in a significant enhancement in OS (median 18.4 vs 12.9 months; HR 0.660; 95% CI 0.505-0.864; P = 0.0023) (5). These trials have validated the viability of this treatment strategy. In this report, we present a case study of a 66-year-old male diagnosed with stage IV poorly differentiated adenocarcinoma of the stomach who underwent treatment with immune checkpoint inhibitors combined with chemotherapy and achieved complete remission. The most frequently observed immune-related adverse events (irAEs) include colitis, endocrinopathies, hepatitis, and pneumonitis (2).In this report, we document a case of a common immune-related adverse event that tragically resulted in fatal outcomes.
Case report
2
Case description:A 66-year-old male presented in early August 2021 with unexplained weight loss, occasional heartburn, acid reflux, poor appetite, and fatigue. He had a 6-year history of diabetes, a smoking index of 1000 pack-years, and a 40-year history of consuming approximately 100ml of strong alcohol daily. The patient had no known drug allergies and no family history of tumors or genetic disorders. Upon admission, clear respiratory sounds were detected in the left lung during auscultation, while the right lung exhibited low respiratory sounds without dry or wet rales. Cardiac auscultation revealed no abnormalities, and there were no alpable or enlarged superficial lymph nodes. On September 3, 2021, the individual underwent enhanced computed tomography (CT) of the upper abdomen at a local hospital, revealing irregular thickening of the gastric wall along with multiple lymph node and liver metastases. Subsequent gastroscopy indicated irregular circumferential elevation, ulceration, and unclear boundaries affecting the entire gastric body, leading to gastric stenosis. Biopsy results confirmed poorly differentiated adenocarcinoma of the gastric body as well as Helicobacter pylori infection. Immunohistochemistry analysis revealed positive expressions of MLH1(+), MSH2(+), MSH6(+), and PMS2(+),indicating microsatellite stability. Additionally, PD-L1 (SP263) testing demonstrated 5% tumor cell (TC) expression, 10% immune cell (IC) expression, and a combined positive score (CPS) of 20. PET-CT confirmed infiltration of the gastric wall to the serosal layer with perigastric, liver gastric ligament, and retroperitoneal lymph node metastases, as well as multiple liver metastases (Figure 1). The patient did not receive any relevant antitumor therapy at an outside hospital. Referred to our hospital on September 8, 2021, for further diagnosis and treatment. Based on the laboratory tests and imaging, the patient was diagnosed with stage IV poorly differentiated adenocarcinoma of the stomach with perigastric, liver gastric ligament, and retroperitoneal lymph node metastases, as well as multiple liver metastases.
Suggestive of gastric cancer, infiltrating the serosal layer into the surrounding adipose tissue (peri-focal, hepatogastric ligament, retroperitoneal) lymph node metastasis, and liver metastasis.
Chemotherapy with oxaliplatin and docetaxel was initiated on September 10, 2021, and continued for 2 cycles. Following two cycles, tumor markers did not decrease, and an enhanced computed tomography (CT) evaluation indicated stable disease (SD) (Figure 2). Due to the limited efficacy of chemotherapy alone and the patient’s PD-L1 CPS20 status, immunotherapy was incorporated into the treatment plan. A combination regimen of albumin-bound paclitaxel, cisplatin, and Sintilimab was administered on October 31, 2021; November 29, 2021; December 24, 2021; and January 18, 2022. The patient did not experience adverse reactions throughout the treatment, suggesting good safety. After four cycles, a partial response (PR) was observed on CT evaluation (Figure 3), followed by stable disease (SD) after six cycles (Figure 4). The maintenance plan included Sintilimab at a dose of 200mg every 21days, with the final treatment given on February 1, 2023.
The efficacy evaluation after 2 cycles chemotherapy is Stable Disease (SD).
The efficacy evaluation after 2 cycles of immunotherapy combined with chemotherapy is Partial Response (PR).
The efficacy evaluation after 4 cycles of immunotherapy combined with chemotherapy is Stable Disease (SD).
During the follow-up examination on June 5, 2023, at our hospital, a positron emission tomography-computed tomography (PET-CT) scan revealed mild thickening of the gastric wall and increased FDG metabolism, suggesting suppression of tumor activity (Figure 5). The tumor marker, carcinoembryonic antigen (CEA), was slightly elevated at 10.9 ng/mL, slightly above the normal range, while other markers remained within normal limits (Figure 6). Subsequent follow-up appointments were conducted every 3 months to monitor the patient’s progress. Imaging examinations consistently revealed no significant advancement of the disease, indicating a stable condition. As of the last evaluation (June 2023), the patient’s progression-free survival (PFS) has reached 21 months.
The gastric wall, liver, and lymph nodes show no increased FDG metabolism, suggesting that tumor activity is suppressed.
The levels of CEA (carcinoembryonic antigen) and CA- 125 (cancer antigen125) have shown significant decreases.
The patient did not experience any specific adverse reactions during treatment. Three weeks after the last treatment on February 25, 2023, the patient developed frequent diarrhea, passing loose stools 8–10 times daily, without abdominal pain, nausea, or vomiting. Symptoms improved after receiving treatment with steroids, gastric protectants, antibiotics, and hydration. However, the diarrhea recurred shortly thereafter, occurring 8 times daily. Upon evaluation in the gastroenterology department, the patient was diagnosed with infectious diarrhea. Treatment with antibiotics and hydration for one week led to symptom relief and discharge. One month later, the patient returned for a follow-up visit and did not report a recurrence of diarrhea. In May 2023, the patient experienced diarrhea again and underwent colonoscopy at a local hospital. The colonoscopy revealed continuous and diffuse lesions extending retrogradely from the distal rectum. These lesions were characterized by rough granular mucosa, diffuse congestion and edema, blurred and disappeared vascular pattern, fragile mucosa, bleeding, and severe areas with erosions or multiple shallow ulcers with purulent material adhering. Pathological findings indicated infiltration of inflammatory cells. Symptoms improved after symptomatic treatment, although specific medications were not specified. During a follow-up on June 4, 2023, the patient did not report diarrhea or abdominal pain, and all auxiliary examinations were normal. However, in July 2023, the patient sought care at another hospital due to persistent diarrhea, which led to coma, hyponatremia, hypochloremia, ineffective treatment, and eventually death. The timetable for diagnosis and treatment intervention for patients is as follows. (Figure 7).
Treatment process and efficacy evaluation.
Discussion
3
In China, 80% of gastric cancer patients are diagnosed at an advanced stage, leading to missed opportunities for surgical resection. HER-2 positive gastric cancer offers more treatment options compared to HER-2 negative cases. The KEYNOTE-811 trial showed a higher objective response rate of 74.4% with pembrolizumab versus 51.9% with placebo (P = 0.00006), including a complete response rate of 11.3% (6). However, only 10-22% of cases are HER-2 positive, with a larger proportion being HER-2 negative. For advanced HER-2 negative gastric cancer, first-line treatment options typically involve systemic chemotherapy or a combination of chemotherapy with anti-PD-L1/PD- 1 monoclonal antibodies (7). The CheckMate-649 trial revealed that the combination of nivolumab with chemotherapy led to a significant improvement in overall survival (OS) and progression-free survival (PFS) compared to chemotherapy alone, especially in patients with a Combined Positive Score (CPS) of 53 or higher. Most trials have indicated that immune combination therapy can be beneficial for patients regardless of PD-L1expression levels. Nevertheless, these studies have also highlighted that immune combination therapy tends to be more effective in patients with high PD-L1expression (3–5). Research has shown that patients treated with programmed cell death protein 1 (PD- 1) inhibitors have a 12.0% to 13.7% incidence of irAEs, with colitis occurring at a rate of 0.7% to 1.6%. The mechanisms behind irAEs are not fully understood, but it is believed to involve nonspecific T cell overactivation and increased cytokine expression, which can lead to a sepsis-like syndrome or abnormal activation of autoreactive T cells (1, 8). In the ORIENT- 16 study, the most common adverse events (incidence ≥ 30%) included decreased platelet count, decreased neutrophil count, decreased white blood cell count, anemia, nausea, vomiting, and increased aspartate aminotransferase.
Gastrointestinal toxicity from PD- 1/PD-L1 inhibitors typically occurred 6 to 8 weeks after starting therapy, but this patient experienced gastrointestinal adverse reactions only after 16 months of immunotherapy (5). Fortunately, this patient exhibits high PD-L1 expression, leading to the adoption of sintilimab in combination with albumin-bound paclitaxel and cisplatin. Subsequent evaluation revealed a complete response. The management of gastric adenocarcinoma poses ongoing challenges, prompting the exploration of novel therapeutic approaches. The integration of immune checkpoint inhibitors with chemotherapy emerges as a promising option for treating advanced HER-2 negative gastric cancer. Noteworthy results from Rationale 305, ORIENT- 16, and CheckMate 649 trials support the efficacy of combining immunotherapy with chemotherapy in patients with complete HER-2 negativity (3–5). These findings underscore the potential of anti-PD-L1 therapy in conjunction with chemotherapy for advanced HER-2 negative gastric cancer. Treatment selection for malignancies involves a dynamic process of refining strategies based on clinical outcomes. The favorable response observed in this case reinforces our confidence in the utility of anti-PD-L1 therapy combined with chemotherapy for advanced HER-2 negative gastric cancer. Collaborative efforts among researchers are anticipated to further enhance the efficacy of this treatment approach in the future.
Regrettably, the patient experienced severe adverse reactions that ultimately led to fatal consequences. Treated with PD- 1 inhibitors for gastric cancer, the patient developed diarrhea, with pathological findings indicating infiltration of inflammatory cells. Based on the patient’s clinical course, age at onset, pre-existing medication history, and symptoms post-drug treatment, a diagnosis of immune-related diarrhea was made. The patient’s demise was not attributed to the cancer itself, but rather to adverse reactions caused by the treatment, a somber realization. Despite showing excellent results of complete remission in the last PET-CT scan, the patient passed away a month later due to uncontrollable gastrointestinal adverse reactions. Had these reactions been manageable, it is possible that the patient’s survival could have been prolonged.
ICIs are a promising cancer treatment, but their use can lead to irAEs, which may affect multiple organs, ranging from mild side effects to severe, life-threatening complications. Currently, reliable biomarkers to predict the risk of immune-related adverse events in patients receiving immune checkpoint inhibitors are lacking. However, research on predictive biomarkers for ICI-related toxicity is progressing rapidly (9).
Common autoantibodies, such as antinuclear antibodies (ANA) and rheumatoid factor (RF), as well as organ-specific antibodies like anti-thyroid antibodies, are considered to have predictive potential (10–13). Additionally, cytokine profiles, such as tumor necrosis factor-α (TNF-α) (14), interleukin-6 (IL-6) (15), interleukin-17 (IL-17) (16, 17), and interleukin-10 (IL-10^)^ (18), may play a role in predicting irAEs. Proteins in serum and other bodily fluids have also shown predictive value for irAEs. Thyroid-stimulating hormone (TSH) is considered the most effective biomarker for monitoring thyroid dysfunction in patients treated with immune checkpoint inhibitors (19–21). Similarly, continuous measurements of serum B-type natriuretic peptide (BNP), troponin, and new-onset electrocardiogram abnormalities help predict cardiovascular irAEs (22). Fecal lactoferrin and calprotectin are commonly used to screen for immune checkpoint inhibitor-induced colitis (23), with calprotectin being particularly useful for assessing treatment response and reducing the need for repeat endoscopies (24).In addition to these biomarkers, baseline absolute counts of neutrophils, lymphocytes, monocytes, eosinophils, and basophils, platelet counts, and changes in white blood cells, lymphocytes, and eosinophils during follow-up are associated with an increased risk of immune-related adverse events. These methods are easy to implement in clinical practice, relatively low-cost, but most studies are retrospective analyses (25–32).
Moreover, research on biomarkers such as genetic variations, gene expression profiles, Human Leucocyte Antigen genotyping, micro RNAs, and gastrointestinal microbiota is gradually progressing (33–40). Despite significant advances in the study of potential predictive biomarkers for immune-related adverse events, no biomarker has been fully validated for widespread clinical application. Apart from routine laboratory tests, other biomarkers have not been recommended for analysis prior to immune checkpoint inhibitor treatment.
The increasing use of ICIs in oncology highlights the importance of monitoring patients for significant irAEs. Vigilance and thorough examination are crucial as irAEs are frequently diagnosed through exclusion. A multidisciplinary approach, involving input from consultants, is usually required to reach the correct diagnosis. Early initiation of glucocorticoids upon diagnosis is essential to prevent rapid deterioration and decrease the chances of severe, fatal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization International Agency for Research on Cancer. GLOBOCAN 2018: estimated cancer incidence, mortality and prevalence worldwide. (Accessed June 16, 2020).
- 2The American Cancer Society. Cancer statistics center. (Accessed June 16, 2020).
- 3Janjigian YY Shitara K Moehler M Garrido M Salman P Shen L. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (Check Mate 649): a randomised,open-label, phase 3 trial. Lancet. (2021) 398:27–40. doi: 10.1016/S 0140-6736(21)00797-2 34102137 PMC 8436782 · doi ↗ · pubmed ↗
- 4Moehler MH Kato K Arkenau H-T Oh D-Y Tabernero J Cruz-Correa M. Rationale 305: Phase 3 study of tislelizumab + chemotherapy vs placebo + chemotherapy as first-line treatment of advanced gastric or gastroesophageal junction adenocarcinoma. J Clin Oncol. (2023) suppl 4):abstr 286. doi: 10.1200/JCO.2023.41.4_suppl.286 · doi ↗
- 5Xu J Jiang H Pan Y Gu K Cang S Han L. LBA 53 Sintilimab plus chemotherapy (chemo) versus chemo as first-line treatment for advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma (ORIENT- 16): First results of a randomized, double-blind,phase III study. Ann Oncol. (2021) 32:S 1331. doi: 10.1016/j.annonc.2021.08.2133 · doi ↗
- 6Janjigian YY Kawazoe A Yañez P YañLi N YañLonardi S Kolesnik O. The KEYNOTE-811 trial of dual PD- 1 and HER 2 blockade in HER 2-positive gastric cancer. Nature. (2021) 600:727–30. doi: 10.1038/s 41586-021-04161-3 PMC 895947034912120 · doi ↗ · pubmed ↗
- 7National Comprehensive Cancer Network. NCCN clinical practice guidelinesin oncology: gastric Cancer(Version 1.2023). [DB/OL]. http://www.nccn.orghttp://www.nccn.org.
- 8Kennedy LB Salama AK. A review of cancer immunotherapy toxicity. CA Cancer J Clin. (2020) 70:86–104. doi: 10.3322/caac.21596 31944278 · doi ↗ · pubmed ↗