A case report of delayed left ventricular rupture after mitral transcatheter edge-to-edge repair: clip entrapment in hypercontractile left ventricle
Shinichi Kurashima, Makoto Amaki, Tomoyuki Fujita, Takeshi Kitai, Chisato Izumi

TL;DR
This case report describes a rare delayed left ventricular rupture after a heart procedure, successfully treated with surgery.
Contribution
The report highlights a novel complication of clip entrapment in a hypercontractile left ventricle after M-TEER.
Findings
Clip entrapment between a hypertrophied papillary muscle and LV wall may cause delayed LV rupture.
Surgical repair and mitral valve replacement successfully treated the complication.
Elderly patients with limited LV space are at higher risk for this rare complication.
Abstract
Left ventricular (LV) rupture is an extremely rare but possible complication after mitral transcatheter edge-to-edge repair (M-TEER). We describe a delayed LV rupture after M-TEER that was successfully treated with surgical repair. An 83-year-old Asian male with congestive heart failure was referred for treatment of severe mitral regurgitation (MR) due to A1/A2 segment prolapse with abnormally hypertrophied anterior papillary muscle. The patient was at high surgical risk, and M-TEER with MitraClip (Abbott Vascular, Minneapolis, MN, USA) was performed. During the procedure, an NT clip became entangled between the hypertrophied papillary muscle and the LV inferolateral wall. After disentangling the clip, we aimed the clip for a second attempt slightly towards the medial side and inserted it into the LV, avoiding interference with the subvalvular apparatus or LV wall. Grasping in this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
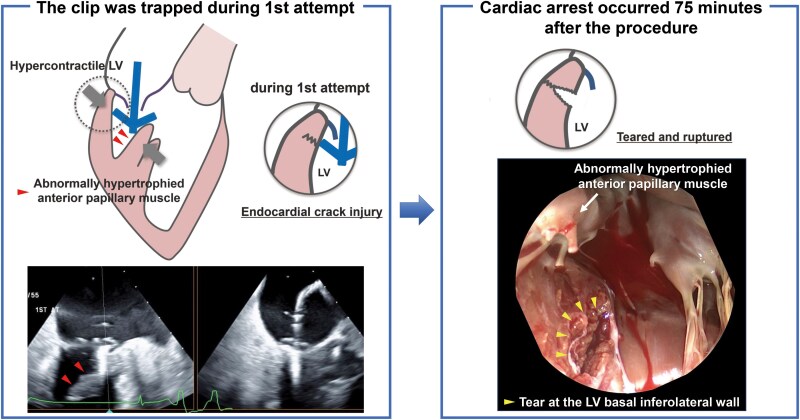 Figure 1
Figure 1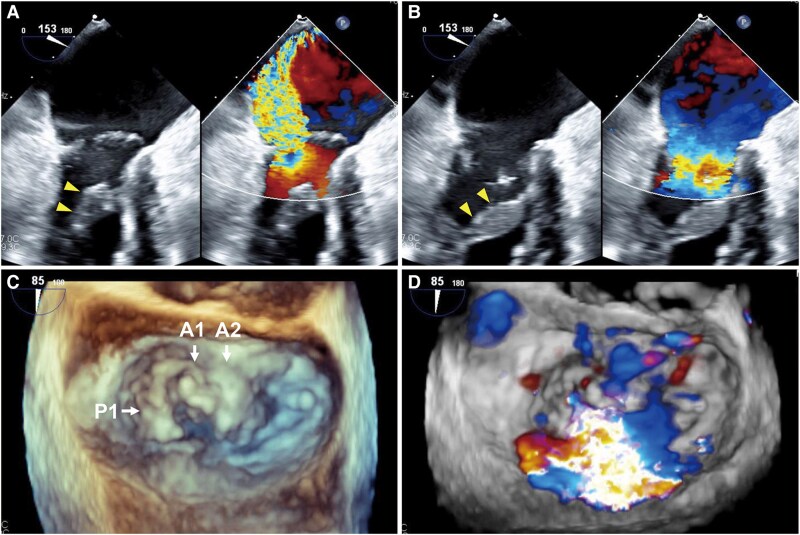 Figure 1
Figure 1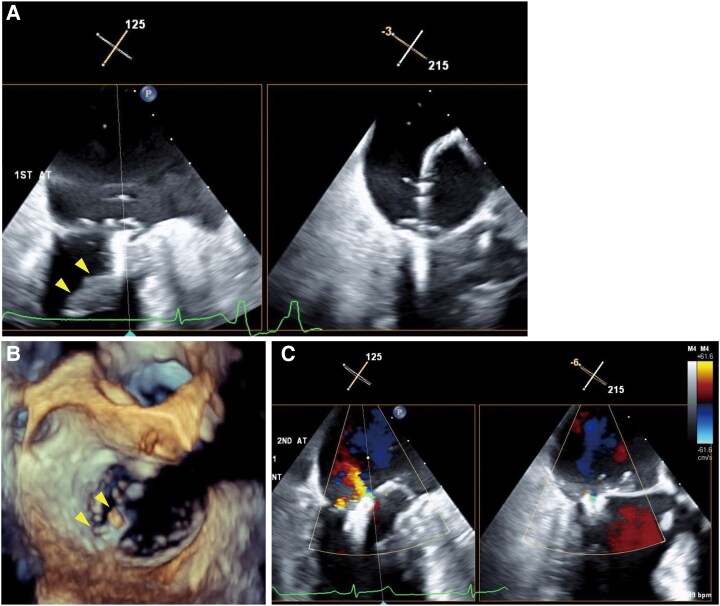 Figure 2
Figure 2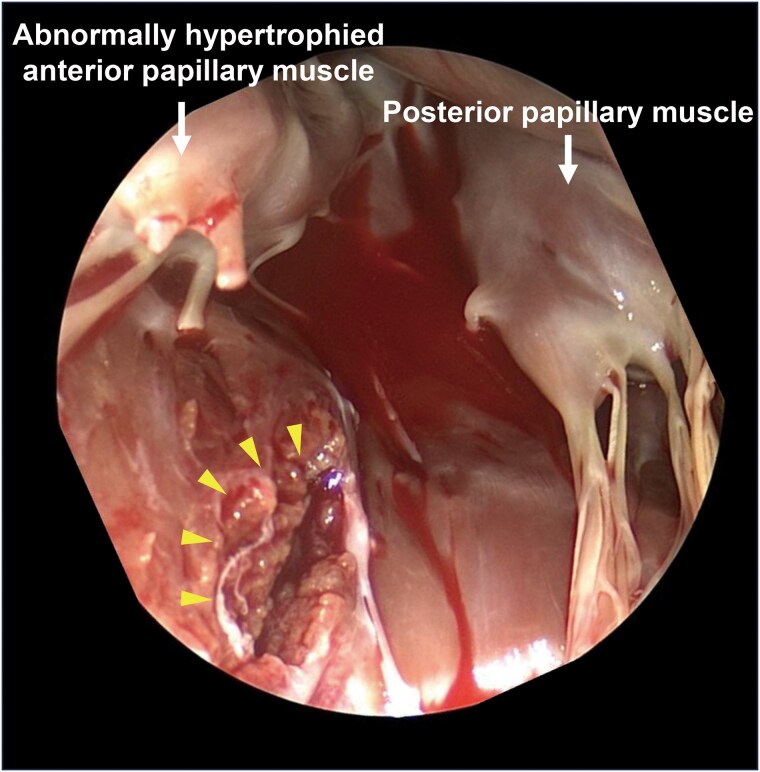 Figure 3
Figure 3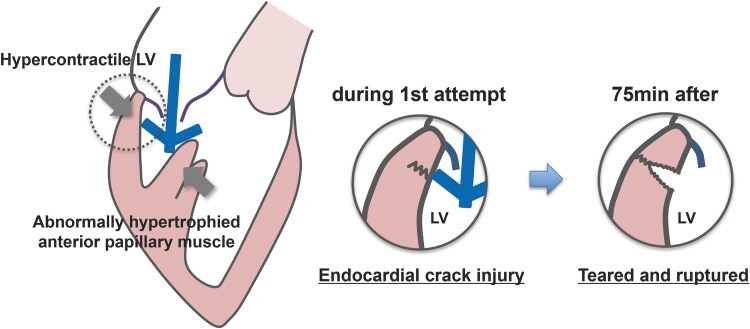 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac Valve Diseases and Treatments · Cardiac pacing and defibrillation studies
Introduction
Mitral transcatheter edge-to-edge repair (M-TEER) is a minimally invasive treatment for both primary and secondary mitral regurgitation (MR) in patients at high surgical risk.^1,2^ Although M-TEER is a safe procedure, there have been fatal complications requiring open chest surgery.^2,3^ Left ventricular (LV) rupture is an extremely rare complication but has recently been reported ‘during’ M-TEER procedure.^4^ We herein report the first case of ‘delayed’ LV rupture after M-TEER successfully treated with emergent LV patch repair and mitral valve replacement (MVR).
Summary figure
**
Case presentation
An 83-year-old Asian male with no prior history of cardiac disease developed exertional dyspnoea 1 month ago and was subsequently admitted to another hospital for acute heart failure. The heart failure was successfully treated with diuretics, and the patient was diagnosed with severe MR due to posterior leaflet prolapse. He had a history of diabetes mellitus, dyslipidaemia, and chronic obstructive pulmonary disease. After 4 months, he was admitted to our hospital for the treatment of severe MR. At admission, he was haemodynamically stable (blood pressure 110/68 mmHg, heart rate 81 b.p.m., and pulse oximetry 98% on room air) and in functional New York Heart Association Class II. He was taking furosemide 40 mg and tolvaptan 7.5 mg for managing fluid retention, as well as empagliflozin 10 mg and rosuvastatin 5 mg. Physical examination revealed no peripheral oedema, clear lung sounds, and an apical holosystolic murmur (Levine 3/6). Electrocardiography showed normal sinus rhythm with no signs of ischaemia or LV hypertrophy. Transthoracic echocardiography (TTE) showed severe MR, with an effective regurgitant orifice area of 40 mm² and a regurgitant volume of 68 mL, calculated using the proximal isovelocity surface area method. Left ventricular ejection fraction was preserved at 65%, with an LV end-diastolic/systolic diameter of 54/37 mm and a septum/posterior wall thickness of 9 mm. Left ventricular strain was within the normal range, and no apical sparing pattern was observed. Transoesophageal echocardiography showed A1/A2 segment prolapse with abnormally hypertrophied anterior papillary muscle (Figure 1; see Supplementary material online, Video S1), which was also observed on TTE (see Supplementary material online, Videos S2–S5).
Preoperative echocardiography. (A) Severe mitral regurgitation due to A1/A2 segment prolapse with hypertrophied anterior papillary muscle (arrowheads) at systole. (B) Hypertrophied anterior papillary muscle (arrowheads) at diastole. (C) 3D image of the mitral valve. (D) 3D colour image of the mitral valve.
The length of the posterior mitral leaflet (PML) was 8.7 mm, and the anterior mitral leaflet was 12.6 mm at the grasping point. The risk of surgical mitral valve repair was moderate with a EuroSCORE Ⅱ of 4.5%. Initially, we considered surgical mitral valve repair due to anatomical concerns. However, after discussions regarding his age and frailty, our heart team concluded that the patient’s surgical risk was high and M-TEER with MitraClip (Abbott Vascular, Minneapolis, MN, USA) was performed.
Since the jet was predominantly from A1-P1 lesion and with limited space between the annulus and abnormally hypertrophied anterior papillary muscle (18.5/10.0 mm at diastole/systole), we selected an NT clip. As the clip was delivered into the A1-P1 lateral lesion, the clip was entangled in the space between the papillary muscle and LV inferolateral wall, and premature ventricular contractions appeared multiple times (Figure 2A and B; see Supplementary material online, Videos S6 and S7). After releasing chordal entanglement and retrieving it back to the left atrium, we aimed the clip for a second attempt slightly towards the medial side of the A1-P1 lesion. Mitral regurgitation significantly improved to mild immediately after grasping and remained after releasing the clip without interfering with the subvalvular apparatus or LV wall (Figure 2C). No pericardial effusion was detected after sheath removal. At the time of extubation, the patient's consciousness was clear. His vital signs were stable, with blood pressure 92/43 mmHg and heart rate 72 b.p.m. After returning to the ward, blood pressure was slightly increased to 135/72 mmHg, but again no pericardial effusion was confirmed. However, sudden cardiac arrest occurred 75 min after the procedure. Chest compressions were immediately initiated, followed by administration of 1 mg intravenous epinephrine twice (total 2 mg) and endotracheal intubation. At the same time, TTE showed massive pericardial effusion. The patient was immediately transferred to the operating room, and extracorporeal circulation was established 15 min after sudden cardiac arrest via femoral arterial and venous cannulation. An emergent sternotomy was done and revealed a tear at the LV basal inferolateral wall just behind the anterior papillary muscle (Figure 3). Surgical patch repair and MVR were performed. After two more open thoracotomies (mediastinal haematoma removal and left atrial thrombectomy), the patient was discharged home without neurological sequelae. Six months after discharge, the patient was admitted with worsening heart failure. Transthoracic echocardiography at readmission showed preserved prosthetic mitral valve function with no residual MR. His condition improved with diuretics, and he remained stable during the 1.5-year follow-up.
The procedure of mitral transcatheter edge-to-edge repair. (A) The clip was entangled to chordae and trapped between hypertrophied papillary muscle (arrowheads) and the left ventricular wall. (B) A 3D mitral valve en face view shows that the clip (arrowheads) was interfering with the inferolateral wall. (C) After the clip deployment, mitral regurgitation was reduced to mild without interference between the clip and the left ventricular wall.
Intraoperative findings. From the surgeon's view, the tear (arrowheads) was observed in the left ventricular inferolateral wall.
Discussion
This is the first report of delayed LV rupture after M-TEER. Recently, Yoshida et al.^4^ reported LV rupture during M-TEER. In their case, the echocardiography showed severe MR due to P3 prolapse. It was considered that the tip of the clip sank into the myocardium during the closing process due to short PML. In addition, LV rupture occurred in the acute phase immediately after grasping. In the present case, P1 length was long enough that the clip arm had not reached the annulus during closure. Moreover, from the surgical findings, the ruptured point was more lateral to the grasping point (where the first attempt was done without grasping), suggesting that rupture was not due to clip grasping of the annulus with a short posterior leaflet.
The most characteristic structure in the present case is abnormally hypertrophied papillary muscle. A workup was performed for underlying cardiac disease including hypertrophic cardiomyopathy and infiltrative cardiomyopathies, especially cardiac amyloidosis. In this case, there were no findings suggestive of such conditions. During the first attempt, although we did not grasp the leaflet, the clip was trapped and sandwiched between the hypertrophied papillary muscle and the hypercontractile LV wall. At this moment, the tip of the clip arm pushed by papillary muscle may have injured and caused a crack at the LV posterior wall and disrupted the endocardium (Figure 4). Also, premature ventricular contractions stimulated by the contact of the clip may have worsened this mechanism by further narrowing the space in the left ventricle. Left ventricular rupture has been reported to occur in 0.8% of cases after MVR, and the mortality rate exceeds 80% when it occurs. Left ventricular rupture commonly occurs in the posterior annulus due to its lack of support from the fibrous skeleton, with advanced age being an additional risk factor.^5^ This anatomic vulnerability of the posterior annulus and tissue fragility due to advanced age may have contributed to the LV rupture in the case of Yoshida et al. as well as in our case. In addition, increased blood pressure after the procedure may have also played the role of crack to tear and resulted in delayed LV rupture.
The mechanism of delayed left ventricular rupture. The open clip trapped between the papillary muscle and the hypercontractile left ventricular wall may have caused a crack in the left ventricular wall, resulting in delayed left ventricular rupture. LV, left ventricle.
Although surgery is a gold standard treatment for symptomatic severe primary MR, about half of the patients do not undergo surgery due to high surgical risk,^6,7^ and they will be candidates for M-TEER. Mitral transcatheter edge-to-edge repair has been applied even in patients with complex mitral anatomies lately. Appropriate clip selection is essential for procedural success. In commissural lesion cases, the NT series is recommended over the XT series due to high risk of clip entanglement or chordal damage.^8^ In our case, the NTW could be considered due to wide flail lesion. However, we selected NT clip with its safeness to dive into dense chordae and hypertrophied papillary muscle. While M-TEER is often favoured for its safety and durability, transcatheter mitral valve implantation (TMVI) may be a viable option in cases with complex lesions, such as multiple jet or severe calcification, which makes repair challenging.^9^ Therefore, a comprehensive anatomical assessment is crucial to inform both clip selection and the consideration of TMVI as a therapeutic alternative. In these challenging cases, the operator’s experience and the volume of the centre are significant factors in achieving successful outcomes.^8^ The eligibility for M-TEER should be evaluated with consideration of the operator’s expertise and the centre’s procedural volume.
Conclusion
Delayed LV rupture should be recognized as a new complication in M-TEER for elderly primary MR patients with limited LV space, especially at near commissure lesions.
Lead author biography
Shinichi Kurashima graduated from Yamagata University with an MD degree in 2016. He is a cardiologist at the National Cerebral and Cardiovascular Center in Osaka, Japan.
Supplementary Material
ytaf265_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Glower DD, Kar S, Trento A, Lim DS, Bajwa T, Quesada R, et al Percutaneous mitral valve repair for mitral regurgitation in high-risk patients: results of the EVEREST II study. J Am Coll Cardiol 2014;64:172–181.25011722 10.1016/j.jacc.2013.12.062 · doi ↗ · pubmed ↗
- 2Chakravarty T, Makar M, Patel D, Oakley L, Yoon SH, Stegic J, et al Transcatheter edge-to-edge mitral valve repair with the Mitra Clip G 4 system. JACC Cardiovasc Interv 2020;13:2402–2414.33011141 10.1016/j.jcin.2020.06.053 · doi ↗ · pubmed ↗
- 3Sorajja P, Vemulapalli S, Feldman T, Mack M, Holmes DR Jr, Stebbins A, et al Outcomes with transcatheter mitral valve repair in the United States: an STS/ACC TVT registry report. J Am Coll Cardiol 2017;70:2315–2327.29096801 10.1016/j.jacc.2017.09.015 · doi ↗ · pubmed ↗
- 4Yoshida A, Mizutani K, Sakaguchi G, Nakazawa GS. Left ventricular rupture after leaflet grasping in transcatheter edge-to-edge mitral valve repair. Eur Heart J Case Rep 2023;7:ytad 614.38111826 10.1093/ehjcr/ytad 614PMC 10726397 · doi ↗ · pubmed ↗
- 5Deniz H, Sokullu O, Sanioglu S, Sargin M, Ozay B, Ayoglu U, et al Risk factors for posterior ventricular rupture after mitral valve replacement: results of 2560 patients. Eur J Cardiothorac Surg 2008;34:780–784.18621539 10.1016/j.ejcts.2008.06.009 · doi ↗ · pubmed ↗
- 6Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Detaint D, Vanoverschelde JL, et al What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur Heart J 2007;28:1358–1365.17350971 10.1093/eurheartj/ehm 001 · doi ↗ · pubmed ↗
- 7Bach DS, Awais M, Gurm HS, Kohnstamm S. Failure of guideline adherence for intervention in patients with severe mitral regurgitation. J Am Coll Cardiol 2009;54:860–865.19695468 10.1016/j.jacc.2009.03.079 · doi ↗ · pubmed ↗
- 8Gavazzoni M, Taramasso M, Zuber M, Russo G, Pozzoli A, Miura M, et al Conceiving Mitra Clip as a tool: percutaneous edge-to-edge repair in complex mitral valve anatomies. Eur Heart J Cardiovasc Imaging 2020;21:1059–1067.32408344 10.1093/ehjci/jeaa 062 · doi ↗ · pubmed ↗