A Case Report of a Rare Cervical Synovial Cyst at the C7-T1 Level
Angel Parushev, Bogomil Iliev, Deyan Dzhenkov, Nadezhda Stefanova, Yanko G Yankov, Mustafa Ali, Yavor Enchev

TL;DR
A rare case of a synovial cyst in the cervical spine was successfully treated with surgery, resolving the patient's symptoms.
Contribution
This report highlights a rare synovial cyst location and emphasizes its importance in spinal lesion differential diagnosis.
Findings
A synovial cyst at C7-T1 caused spinal cord compression and myelopathy in a 52-year-old man.
Surgical excision via a posterior midline approach resolved symptoms and confirmed a hemorrhagic synovial cyst.
Synovial cysts should be considered in the differential diagnosis of extradural spinal lesions.
Abstract
Synovial cysts are rare, non-neoplastic lesions, with occasional cervical spine involvement. These cysts may compress neural structures, causing radicular pain, myelopathy, or neurological deficits. Surgical excision is the standard treatment for symptomatic cases. This case report presents a 52-year-old man with a three-month history of neck pain, stiffness, and progressive left upper limb weakness and numbness. Magnetic resonance imaging (MRI) revealed a left-sided flaval ligament cyst at C7, causing spinal cord compression and myelopathy. Surgical excision was successfully performed via a posterior midline approach. Histopathological findings confirmed a hemorrhagic synovial cyst. Postoperatively, the patient experienced full symptom resolution. Although rare, synovial cysts should be considered in the differential diagnosis of extradural spinal lesions, as their presence carries…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
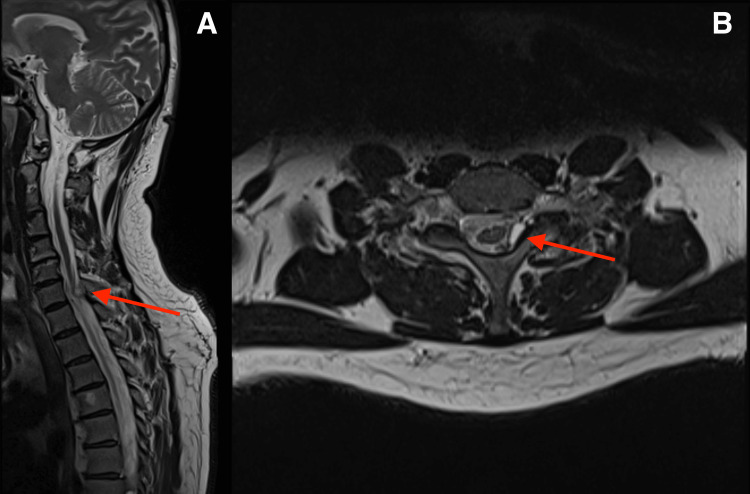 Figure 1
Figure 1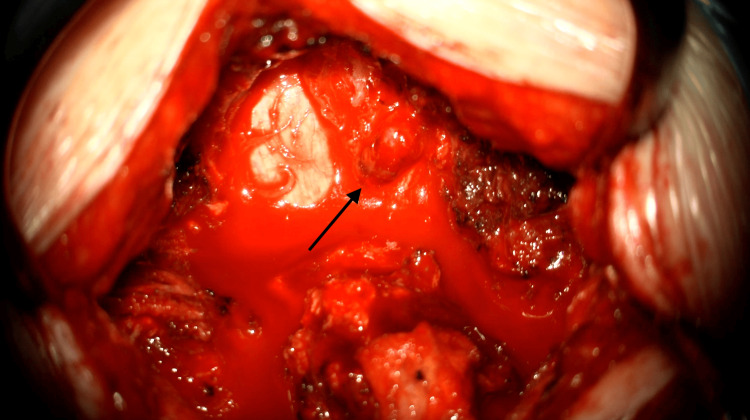 Figure 2
Figure 2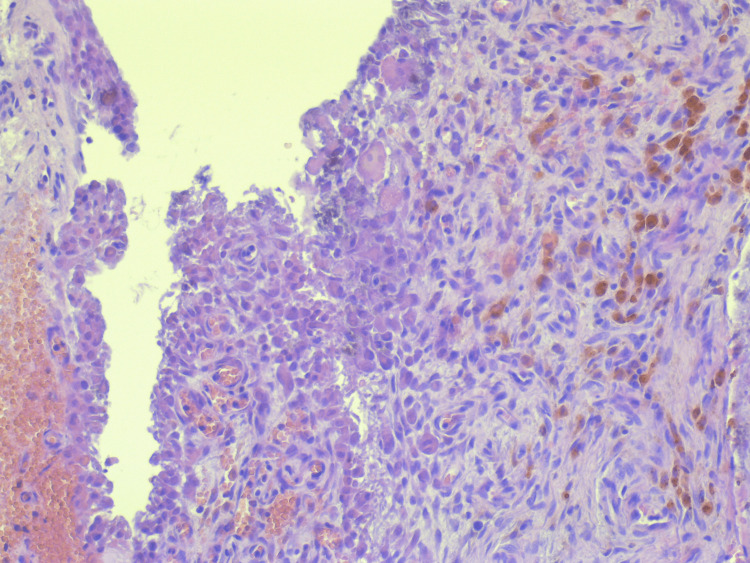 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Orthopaedic implants and arthroplasty · Shoulder Injury and Treatment
Introduction
Synovial cysts are cystic lesions characterized by a synovial lining and are in continuity with the facet joint [1]. These lesions are non-neoplastic and arise from herniation of the synovium through the joint capsule or tendon sheath into adjacent tissues or from the expansion of a pre-existing bursa [2].
In the spine, synovial cysts are often associated with conditions such as osteoarthritis, spinal instability (including spondylolisthesis), and trauma [2]. The first description of this entity dates back to 1880, marking the initial recognition of its clinical and pathological characteristics [3]. Synovial cysts most commonly occur in the lumbar spine, with thoracic and cervical presentations being significantly less frequent [4,5]. Cervical spinal synovial cysts are particularly rare, representing only 2.6% of all spinal synovial cysts [6]. Although uncommon, these cysts can cause spinal cord or nerve root compression, leading to symptoms consistent with mass effect. As they enlarge, synovial cysts may become symptomatic by exerting pressure on neural elements within the spinal canal [7]. For extradural synovial cysts, the current standard of care involves surgical decompression through laminectomy and cyst excision [8].
This case report presents a case of a cervical synovial cyst recently treated in the Clinic of Neurosurgery at the University Hospital "St. Marina", Varna, Bulgaria. Informed consent was obtained from the patient. Additionally, we conducted a review of the relevant literature for this rare entity, focusing on contemporary management strategies and decision-making approaches for this rare condition.
Case presentation
In August 2024, a 52-year-old man was admitted to the Clinic of Neurosurgery at the University Hospital "St. Marina", Varna, Bulgaria. The patient presented with a three-month history of neck pain and stiffness, which had worsened over the past month, accompanied by left upper limb weakness, paresthesia, and pain. He did not report any concomitant disease or any medication to be taken regularly.
Physical examination demonstrated a reduced range of motion in the cervical spine due to pain and stiffness. Clinical findings were consistent with right C8 radiculopathy, evidenced by sensory deficits in the C8 dermatome and weakness in grip strength and finger flexion on the affected side. The biceps reflex was preserved, and tone and reflexes in the lower limbs were symmetrical.
A cervical magnetic resonance imaging (MRI) scan demonstrated a cyst-like lesion (dimensions: 7.3×9×5.3 mm) of the flaval ligament at the level of C7 vertebrae on the left side, causing compression and myelopathy of the spinal cord in the zone of indentation, with noted cervical lordosis, cervicoarthrosis, and mild multisegmental degenerative discogenic pathology with specific characteristics and localization (Figure 1).
Cervical spine MRIA: Sagittal MRI showing a cervical synovial cyst at the C7-T1 level (red arrow). B: Axial MRI demonstrating an intraspinal, extramedullary cyst located left parasagittally, causing spinal cord compression and associated myelopathy (red arrow).MRI: magnetic resonance imaging
Considering these findings, the patient provided written informed consent and underwent surgical excision of the cyst under general anesthesia. A left C7 hemilaminectomy was performed via a posterior midline approach. While most reported cases describe a full laminectomy, we opted for a hemilaminectomy, which provided adequate exposure to visualize and access the lesion while preserving spinal stability. The cyst was visualized under the microscope and found to originate from the left C7-T1 facet joint. Precise excision of the cyst was successfully accomplished using a microsurgical technique, ensuring meticulous removal of the cyst wall while preserving surrounding structures (Figure 2). We decided against using fusion in this case due to the absence of cervical instability on imaging and patient-specific factors, such as age and lack of comorbidities.
Intraoperative image visualizing the cyst following left hemilaminectomy at the C7 level (black arrow)
The histological analysis of the excised mass revealed characteristic features consistent with a synovial cyst. The examination identified fragmented sections of the cystic wall, lined with synovial cells, alongside areas of fibrous connective and cartilaginous tissue interspersed with small foci of calcifications. Extensive zones of hemorrhage were observed, surrounded by perifocally located pigmented macrophages, identified as siderophages. These histopathological findings confirmed the diagnosis of a hemorrhagic synovial cyst (Figure 3).
Histological sections show a synovial cyst lined by a cuboidal epithelium-like fibrous wall, with focal hemosiderophages and areas of dystrophic calcification (H&E, ×10)H&E: hematoxylin and eosin
The postoperative period was uneventful, with immediate resolution of the patient's radicular pain following the procedure. The patient demonstrated good neurological recovery, with improvement in grip strength and sensory function in the affected C8 distribution. Early mobilization was encouraged, and the patient was started on a tailored physiotherapy program to optimize cervical spine mobility, strengthen upper limb musculature, and prevent post-surgical stiffness. Pain was well-controlled with analgesics, and no complications were observed during the hospital stay. The patient was discharged four days after surgery, with instructions to continue physiotherapy and attend regular follow-up appointments to monitor recovery and ensure long-term functional improvement. The patient was evaluated 10 days postoperatively for suture removal and assessment of wound healing, which demonstrated proper healing without complications. A subsequent follow-up at one month revealed complete resolution of neurological symptoms, confirming a successful surgical outcome.
Discussion
Cervical synovial cysts are rare in adults and have not been documented in pediatric or adolescent populations [9]. Nevertheless, there is one case of a 16-year-old girl with a C6-C7 synovial cyst [10]. However, spinal synovial cysts most commonly present during the sixth decade of life [11]. To date, the natural history and pathogenesis of intraspinal synovial cysts remain poorly understood and require further elucidation [12].
Patients may be asymptomatic, and cysts can be discovered incidentally [13]. When cysts grow epidurally into the spinal canal, they can compress neural structures, leading to various clinical symptoms [2]. The clinical presentation of a cyst is influenced by its size, location, and the relationship to surrounding bony and neural structures. Most symptomatic patients report experiencing radicular pain and neurological deficits [4]. These cysts can bleed and have a hemorrhage inside them, leading to the sudden onset of symptoms or their increased volume, identical to our case presentation [14].
Most reported cases of cervical synovial cysts have been located at the C7-T1 level [15]. A recent comprehensive study conducted in 2023 analyzed 96 cases of cervical synovial cysts reported in the literature, categorizing them according to their cervical spine level as follows: C2-C3 (four cases), C3-C4 (11 cases), C4-C5 (12 cases), C5-C6 (seven cases), C6-C7 (seven cases), and C7-T1 (55 cases) [16]. MRI is the imaging modality of choice for diagnosing spinal synovial cysts [17]. On MRI, these cysts appear as well-defined, extradural, intraspinal lesions typically situated adjacent to the facet joint [1].
In symptomatic patients with refractory pain and neurological symptoms, surgical management is advised. According to a systematic review by Bydon et al., spinal synovial cysts recurred in 1.8% of cases treated with decompression alone, while no recurrences were reported when fusion was added [18]. The primary surgical techniques employed included laminectomy and hemilaminectomy, with some cases incorporating fusion. However, the role of motion segment fusion in the management of symptomatic synovial cysts requires further investigation [19].
Conclusions
Although rare, synovial cysts should be considered in the differential diagnosis of extradural spinal lesions, particularly in cases presenting with radiculopathy or neurological deficits. Early identification using appropriate imaging and management is crucial to prevent progressive neurological impairment and optimize patient outcomes. In symptomatic cases with neurological deficits, surgical intervention is recommended, with hemilaminectomy and laminectomy serving as the primary operative techniques.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Imaging of facet joint diseases Clin Imaging Kwee RM Kwee TC 1671798020213433335210.1016/j.clinimag.2021.07.005 · doi ↗ · pubmed ↗
- 2Spinal lumbar synovial cysts. Diagnosis and management challenge Eur Spine J Khan AM Girardi F 117611821520061644020210.1007/s 00586-005-0009-4PMC 3233964 · doi ↗ · pubmed ↗
- 3On the formation of synovial cysts in the leg in connection with disease of the knee-joint. 1877 Clin Orthop Relat Res Baker WM 2101994 https://pubmed.ncbi.nlm.nih.gov/8119018/8119018 · pubmed ↗
- 4Spinal synovial cysts. A case series and current treatment options J Clin Neurosci Themistoklis KM Papasilekas TI Boviatsis KA 173177572018 https://doi.org/10.1016/j.jocn.2018.08.0383015006310.1016/j.jocn.2018.08.038 · doi ↗ · pubmed ↗
- 5The role of spinal fusion in the treatment of cervical synovial cysts: a series of 17 cases and meta-analysis J Neurosurg Spine Bydon M Lin JA de la Garza-Ramos R 9199282120142525955410.3171/2014.8.SPINE 13897 · doi ↗ · pubmed ↗
- 6Synovial cysts at the cervicothoracic junction: illustrative series of three cases Surg Neurol Int Yang DB Harms J Iyer RK Arnold P 1961420233740450410.25259/SNI_88_2023 PMC 10316244 · doi ↗ · pubmed ↗
- 7Bilateral synovial cysts as a rare cause of myelopathy in a 38-year-old woman Cureus Mustroph ML Cerecedo-Lopez CD Groff M Zaidi HA 011201910.7759/cureus.5377 PMC 678684131616609 · doi ↗ · pubmed ↗
- 8Hemorrhagic synovial cyst: an unexpected cause of acute cervical spinal cord compression. Case report Int J Surg Case Rep Radhouane K Dridi H Mansouri N Yedeas MD Harbaoui A Chkili R 5275307720203339583810.1016/j.ijscr.2020.11.040PMC 7704358 · doi ↗ · pubmed ↗