Proximal tibiofibular synostosis in HDP SPECT/CT bone scan: A case report
Eliluane Pirazzo Andrade Teixeira, Charles-Edouard Decorads, Inès Castarède, Sana Boudabbous, Valentina Garibotto

TL;DR
A case report describes a rare bone condition in a 47-year-old man using HDP SPECT/CT imaging.
Contribution
This case highlights the use of HDP SPECT/CT for characterizing proximal tibiofibular synostosis.
Findings
HDP SPECT/CT revealed proximal tibiofibular synostosis in a patient with a history of repetitive microtraumas.
The imaging findings aid in understanding the condition's pathogenesis and treatment planning.
Abstract
We report the HDP SPECT/CT findings in a case of proximal tibiofibular synostosis in a 47-year-old man with a history of repetitive microtraumas from former sports activities. Characterization of this rare entity using 99mTc-HDP SPECT/CT is essential for understanding its pathogenesis and guiding appropriate treatment strategies.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
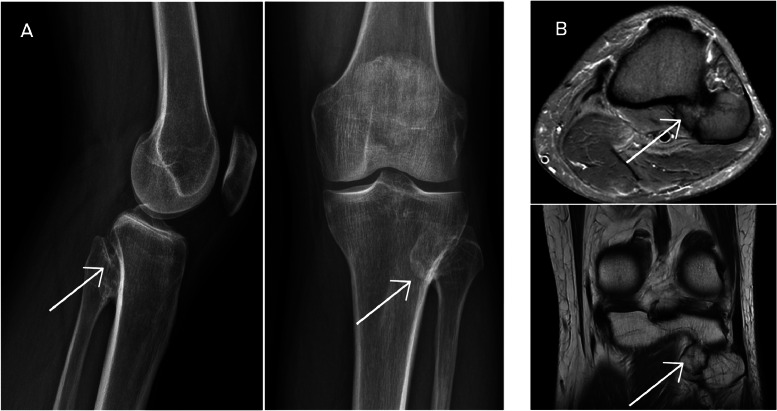 Figure 1
Figure 1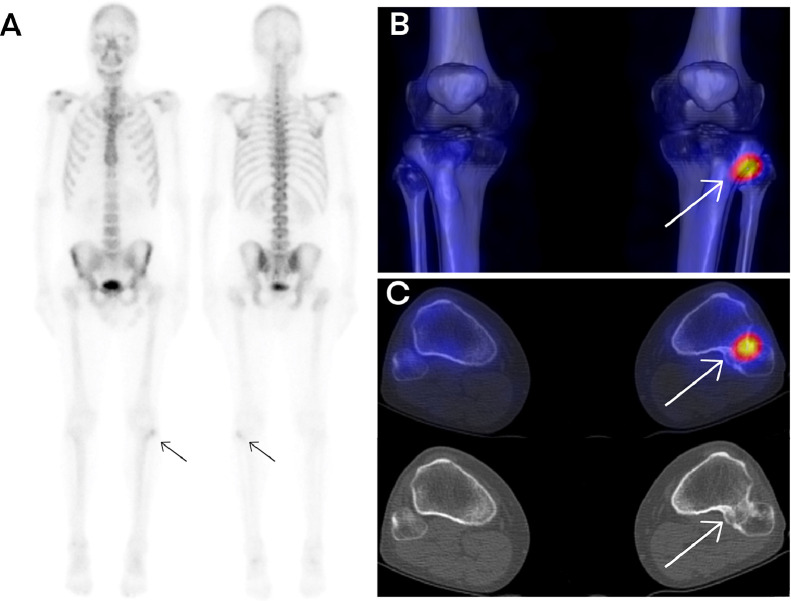 Figure 2
Figure 2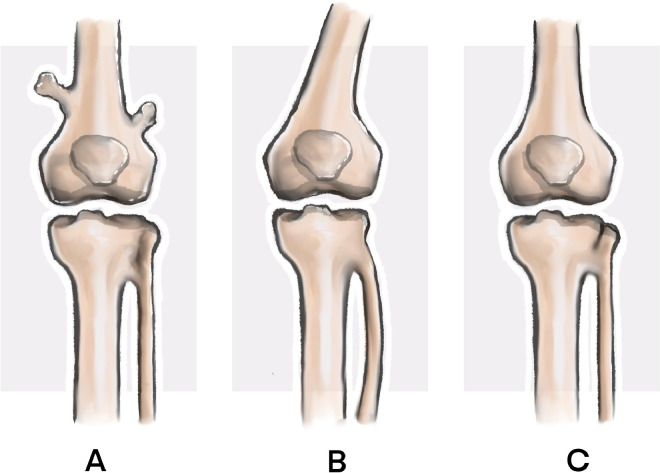 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Bone health and treatments · Bone fractures and treatments
Case report
A 47-year-old man, previously active in martial arts, skateboarding, and snowboarding for over 2 decades, presented with chronic right knee pain radiating from the foot to the mid-thigh. The pain was constant, aggravated by movement, and exacerbated by cold, rainy, or windy weather. He reported a progressive enlargement of a palpable bony mass at the fibular head. Physiotherapy failed to alleviate symptoms, and complex regional pain syndrome (CRPS) was initially suspected.
Initial plain radiographs and MRI of the right knee demonstrated an enlarged fibular head without signs of dislocation or subluxation. A 3-phase bone scintigraphy using technetium-99m HDP revealed focal increased radiotracer uptake at the proximal tibiofibular joint, suggestive of elevated osteoblastic activity.
Subsequent HDP SPECT/CT imaging confirmed the presence of a bony bridge between the proximal tibia and fibula, indicative of a synostosis [1]. There was no evidence of joint dislocation or subluxation. The absence of a cartilaginous cap on MRI excluded the diagnosis of osteochondroma. These findings were consistent with a nonosteochondroma-related proximal tibiofibular synostosis.
Discussion
Proximal tibiofibular synostosis is a rare condition that can have either congenital or acquired origins [2]. It is frequently overlooked due to its nonspecific clinical presentation, which may include posterolateral knee pain, localized swelling, and reduced ankle mobility. The rarity and subtlety of symptoms contribute to delayed diagnosis and misinterpretation (Fig. 1, Fig. 2, Fig. 3).Fig. 1(A) Lateral, anteroposterior, and posteroanterior plain radiographs of the right knee showing an enlarged fibular head. (B) Axial and coronal MRI images confirming the enlarged fibular head without dislocation or subluxation.Fig 1. Fig. 2(A) Whole-body scintigraphy showing focal increased uptake at the proximal tibiofibular joint. (B) 3D SPECT/CT fusion and (C) 2D SPECT/CT images demonstrating bony bridging between the proximal tibia and fibula.Fig 2. Fig. 3Schematic representation of Takai's classification of proximal tibiofibular synostosis: Type A (osteochondroma-related), Type B (congenital/childhood-onset), and Type C (acquired in adulthood).Fig 3
Radiographic evaluation typically reveals bony bridging between the proximal tibia and fibula [3]. Differentiating congenital from acquired forms—resulting from repetitive trauma, previous surgery, or inflammatory processes—is crucial for determining prognosis and management. MRI plays a key role by demonstrating cortical continuity and the absence of a cartilaginous cap, features that help rule out osteochondroma.
Takai et al. proposed a classification system for proximal tibiofibular synostosis [4]:
- •Type A: Osteochondroma-related.
- •Type B: Congenital or childhood-onset.
- •Type C: Acquired in adulthood.
Based on the patient’s clinical history and imaging findings, this case aligns with Type C synostosis, likely acquired due to repeated microtraumas over years of intense physical activity.
Management is typically conservative in asymptomatic or mildly symptomatic cases. In cases with persistent pain or functional impairment, surgical intervention may be considered. Options include resection of the fibular head, excision of the synostosis, or corrective osteotomy.
Conclusion
This case highlights the diagnostic utility of HDP SPECT/CT in evaluating proximal tibiofibular synostosis [5]. This imaging modality provides both anatomical and metabolic information, facilitating differentiation between congenital and acquired forms and supporting treatment planning in symptomatic patients.
Patient consent
I confirm that written informed consent was obtained from the patient for the publication of this case report, including all accompanying images and clinical information. The patient has approved the content and understands that all identifying details will remain confidential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Savelli G.Maffioli L.Maccauro M.De Deckere E.Bombardieri E.Bone scintigraphy and the added value of SPECT in detecting skeletal lesions Q J Nucl Med 4512001273711456373 · pubmed ↗
- 2Sferopoulos N.K.Synostosis of the proximal tibiofibular joint Case Rep Med 2010201079459410.1155/2010/794594 PMC 289269720592991 · doi ↗ · pubmed ↗
- 3Hey H.W.Ng L.W.Ng Y.H.Sng W.Z.Manohara R.Thambiah J.S.Radiographical definition of the proximal tibiofibular joint—a cross-sectional study of 2984 knees and literature review Injury 47620161276128110.1016/j.injury.2016.01.03526975794 · doi ↗ · pubmed ↗
- 4Wakayama T.Imanishi J.Yazawa Y.Okubo T.Kaneko K.Bilateral non-osteochondroma-related proximal tibiofibular synostosis Skeletal Radiol 431220141737174210.1007/s 00256-014-1932-424915740 · doi ↗ · pubmed ↗
- 5Kuwert T.Skeletal SPECT/CT: a review Clin Transl Imaging 2201450551710.1007/s 40336-014-0090-y · doi ↗