Evaluation with a haemodynamic simulator undergoing mitral transcatheter edge-to-edge repair in a giant left atrium
Yusuke Watanabe, Akihisa Kataoka, Kento Kito, Takuya Nishikawa, Keita Saku

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
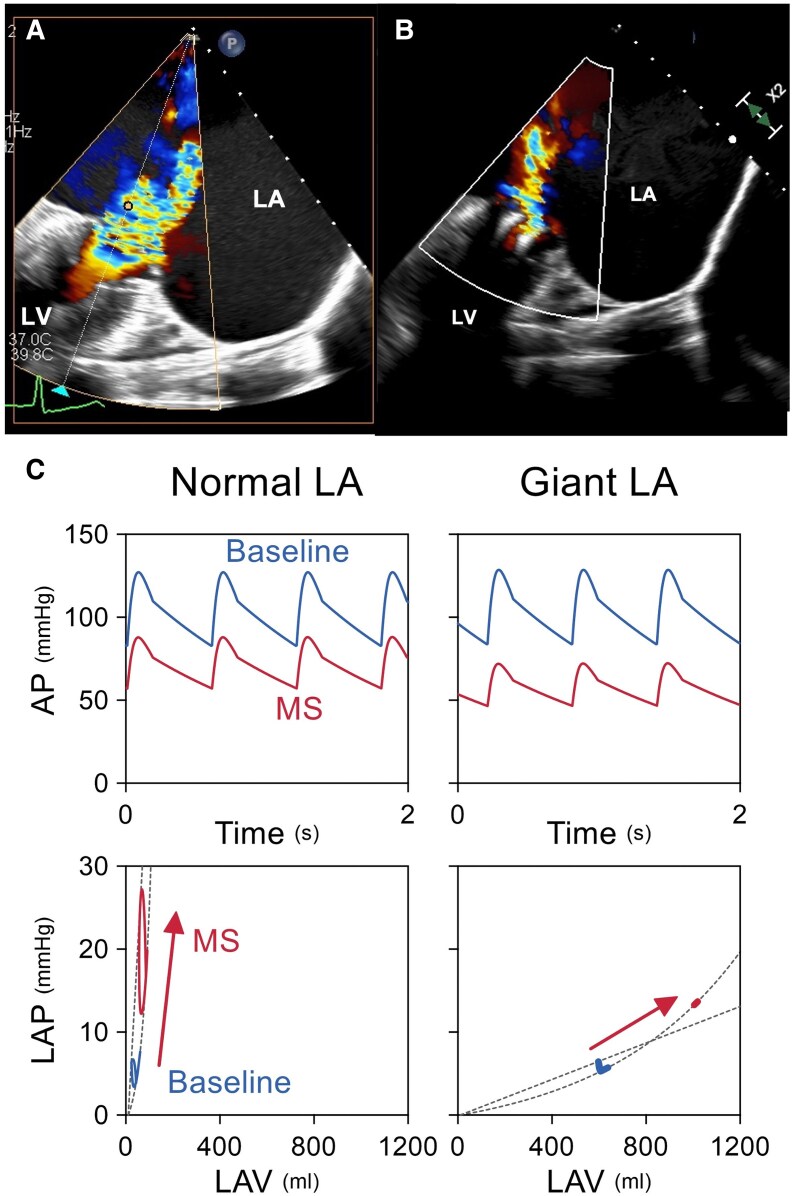 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Cardiac Valve Diseases and Treatments · Cardiac pacing and defibrillation studies
Case description
A 68-year-old woman with atrial fibrillation and a giant left atrium (LA) underwent transcatheter edge-to-edge repair (TEER) for severe atrial functional mitral regurgitation (MR) (see Supplementary material online, Video S1–S4). Although mitral regurgitation improved, she developed hypotension due to iatrogenic mitral stenosis. A cardiovascular simulator visualized impaired left ventricular (LV) filling in this highly compliant LA, supporting the physiological mechanism behind post-procedural instability.
Severe MR with markedly enlarged LA (100 mm) was confirmed on echocardiography. TEER with two MitraClips reduced MR to mild-moderate (Figure 1A, Supplementary material online, Video S5) but raised mitral gradient to 6 mmHg. Hypotension persisted post-procedure. Cardiovascular simulation confirmed that impaired LA pressure build-up contributed to reduced LV filling and hypotension (Figure 1B and C). This case highlights the haemodynamic challenges of TEER in a giant LA. Unlike a normal-sized LA, a giant LA’s high compliance prevents effective pressure generation, impairing LV filling under mitral stenosis conditions. Transcatheter edge-to-edge repai in giant LA cases can lead to iatrogenic MS and haemodynamic instability. Cardiovascular simulation provided valuable insights into haemodynamic changes, enhancing understanding of post-TEER effects (see Supplementary material).
(A, B) Transesophageal echocardiography images pre (A) and post-transcatheter edge-to-edge repair in a giant left atrium (B). (C) Giant left atrium prevents the increase in LV filling, resulting in a significant decrease in cardiac output. TEE, transesophageal echocardiography. TEE, transesophageal echocardiography; TEER, post-transcatheter edge-to-edge repair; LA, left atrium.
Supplementary Material
ytaf261_Supplementary_Data