Experience conducting COVID-19 vaccine effectiveness studies in response to the COVID-19 pandemic in Japan and the Philippines: lessons for future epidemics and potential pandemics
Takeshi Arashiro, Regina Pascua Berba, Joy Potenciano Calayo, Rontgene Solante, Shuichi Suzuki, Jinho Shin, Motoi Suzuki, Martin Hibberd, Koya Ariyoshi, Chris Smith

TL;DR
This paper discusses the challenges and lessons learned from conducting vaccine effectiveness studies in Japan and the Philippines during the COVID-19 pandemic.
Contribution
The paper highlights practical strategies for improving vaccine effectiveness monitoring in future epidemics.
Findings
Japan used transparent reporting to build public confidence in vaccination programs.
The Philippines faced delays due to stakeholder alignment and regulatory approval.
Key challenges included data collection, bias identification, and timely policy communication.
Abstract
Once COVID-19 vaccines were rolled out, there was a need to monitor real-world vaccine effectiveness to accumulate evidence to inform policy and risk communication. This was especially true in Japan and the Philippines, given historical issues that affected vaccine confidence. Neither country had public health surveillance that could be enhanced to evaluate vaccine effectiveness or readily available national vaccination databases. Study groups were established in multiple health-care facilities in each country to assess vaccine effectiveness against both symptomatic infection and severe disease. In Japan, multiple study reports were published in Japanese on the web site of the National Institute of Infectious Diseases and presented at the national government’s advisory board. Nationwide media coverage facilitated transparency and increased the confidence of the government and the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
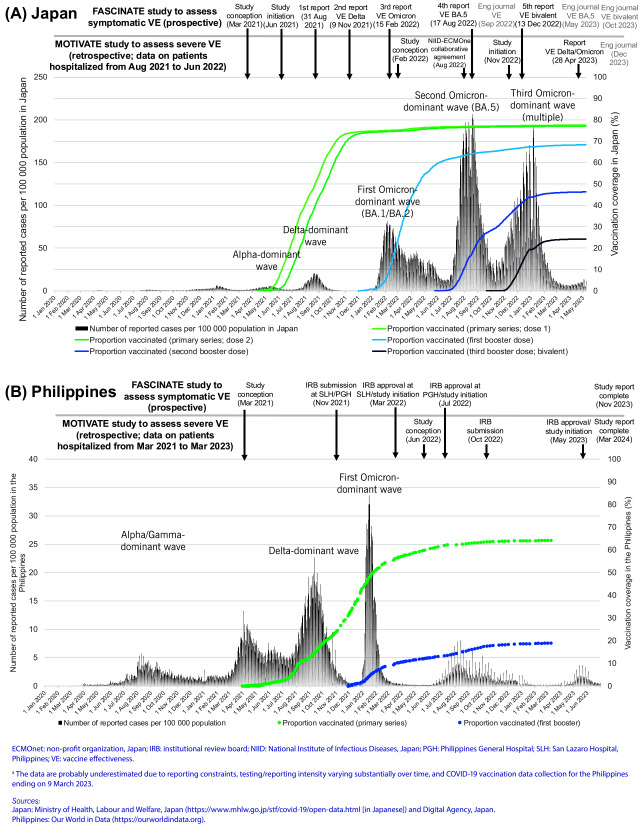 Fig. 1
Fig. 1| Implementation challenges | Solutions/mitigations (checkmark [✓] for the ones used and arrowhead [⮚] for suggestions for future studies) | Countries |
|---|---|---|
|
|
|
|
|
|
|
|
| Epidemiological biases and confounders (see |
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
| Epidemiological biases and confounders | Problem | Approach to reduce biases/confounders (checkmark [✓] for the ones used and arrowhead [⮚] for suggestions for future studies) |
|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVaccine Coverage and Hesitancy · COVID-19 epidemiological studies · Viral Infections and Outbreaks Research
PROBLEM
COVID-19, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has resulted in substantial morbidity and mortality globally. Once vaccines were rolled out, real-world vaccine effectiveness (VE) data were needed to accumulate evidence to inform policy and risk communication. (1) This became more apparent during the early unblinding of randomized controlled trials, (2) together with evidence of waning immunity and the emergence of variants with immune escape properties. (3, 4) Although the World Health Organization (WHO) did not recommend that all countries conduct VE studies on account of methodological complexity and susceptibility to biases, (5) it was considered valuable for Japan and the Philippines to conduct VE studies for several reasons: (1) historical issues with vaccine confidence in both countries and in neighbouring countries (especially given previous issues that affected vaccine confidence, for example, human papillomavirus and influenza vaccines in Japan (6, 7) and dengue vaccine in the Philippines (8)); (2) new vaccine technologies, such as messenger ribonucleic acid (mRNA) vaccines and viral vector vaccines, were rolled out to the general population for the first time and the effects may vary by population subgroup; (3) substantial variation in public health and social measures implemented among countries (which may affect VE estimates (9)); and (4) considerable cumulative burden of infections among different populations (as individuals with prior infection are at least partially protected against subsequent infections and diseases). VE studies in low- and middle-income countries (LMICs) were considered particularly informative for the following reasons: (1) evaluation of vaccines that are mainly distributed in LMICs as part of public health response measures; (2) confirmation that the vaccines remain active through distribution networks (for example, no cold chain breach, as temperature control is especially important for vaccines such as mRNA vaccines); and (3) capacity-building to conduct operational research to inform various public health responses for COVID-19 as well as future epidemics and pandemics.
The authors, together with collaborators established health-care facility-based study groups in Japan and the Philippines to assess VE against symptomatic infection (FASCINATE study) and severe disease (MOTIVATE study). (9-15) This report describes the experience of planning, establishing and executing these VE studies during the COVID-19 pandemic.
CONTEXT
As in other countries, the COVID-19 pandemic substantially affected Japan and the Philippines. The epidemic curve of reported COVID-19 cases and vaccination rollout with selected study milestones in each country are illustrated in Fig. 1. In Japan, the primary series rollout started in mid-February 2021, with the first booster dose in December 2021, the second booster dose in May 2022 and the third booster dose (bivalent vaccines) in September 2022. The second booster dose was administered exclusively to individuals who were ≥ 60 years old, had comorbidities or were health-care or long-term care workers. The majority of the administered vaccines were manufactured by Pfizer-BioNTech and Moderna (99.9% for the primary series).
In the Philippines, the primary series rollout started in March 2021. The first booster dose rollout started in November 2021 among health-care workers (HCWs), senior citizens and immunocompromised individuals, and was expanded to adults aged ≥ 18 years in December 2021. The second booster dose rollout started in April 2022 among HCWs and individuals who were ≥ 60 years old, and in July 2022 among individuals who were ≥ 50 years old and those aged 18–49 years with comorbidities. In the FASCINATE study, among the vaccinees for the primary series, 39% received AstraZeneca, 37% received Sinovac, 18% received Pfizer-BioNTech or Moderna, and 6% received other types. Over 90% of the vaccinees received Pfizer-BioNTech or Moderna booster doses.
Epidemic curves of the number of reported COVID-19 cases and vaccine rollout with study milestones in (A) Japan and (B) the Philippinesa
Existing public health surveillance, such as for influenza-like illness (ILI) and severe acute respiratory infection (SARI), was not easy to enhance rapidly to evaluate VE. Therefore, we collaborated with health-care facilities to set up prospective studies in both countries.
ACTION
Study groups to assess VE against symptomatic infection (FASCINATE study groups) were formed in each country. Mild symptomatic infection was the outcome of choice, as it was the endpoint of the trials. Health-care facilities that routinely testing for SARS-CoV-2 among symptomatic individuals of different ages in the outpatient setting were recruited and the studies were initiated in each country. The FASCINATE study also aimed to elucidate sociobehavioural factors associated with SARS-CoV-2 infection. Subsequently, emerging evidence suggesting that VE wanes against mild symptomatic infection and is also less effective in the Omicron setting resulted in the need to evaluate VE against severe disease. Therefore, additional MOTIVATE study groups were formed and initiated in both countries. For MOTIVATE study groups, health-care facilities that routinely admitted individuals with COVID-19 and pneumonia due to other etiologies (for example, bacterial pneumonia) were recruited. We examined VE against various severe outcomes, including oxygen use, invasive mechanical ventilation use and death. We also collected data on whether medical intervention, such as oxygen use, was due to COVID-19 or other diseases among those who tested positive for SARS-CoV-2.
OUTCOME
In Japan, the study prompted the publication of multiple study reports in Japanese on the National Institute of Infectious Diseases (NIID) web site. They were also presented at the national government’s advisory board to inform policy and risk communication (Fig. 1). Since NIID is part of the Ministry of Health, Labour and Welfare (MHLW) in Japan, authorization was obtained from the MHLW before publication. Published findings were disseminated via multiple nationwide news media platforms, increasing the confidence of the government and the public in the vaccination programme. This continued until the transition to the endemic phase in May 2023. In the Philippines, due to the delay in initiating the study, the report became available in November 2023 for the FASCINATE (outpatient) study and in March 2024 for the MOTIVATE (inpatient) study.
Discussion
Many challenges in conducting VE studies were encountered in both countries (Table 1). Here, four main challenges are highlighted. The first challenge was identifying health-care facilities willing to participate in the study. HCWs were working around the clock in response to the pandemic, and any additional work was often not possible. In Japan, the authors contacted the health-care facilities directly to seek cooperation. In total, 16 clinics and hospitals for the FASCINATE study and 29 hospitals for the MOTIVATE study agreed to join. Specifically, for the MOTIVATE study in Japan, NIID and ECMOnet (a non-profit organization formed by critical care physicians) successfully collaborated to identify health-care facilities. (13) In the Philippines, the FASCINATE study was conducted in two hospitals, while the MOTIVATE study was a single-centre study.
The second challenge was that there was no national database of vaccination records. Therefore, such data were collected at each health-care facility (using either a vaccination card, medical chart or self-report (16)). However, collecting accurate vaccination histories can be resource-intensive, as described in this report. This was a disadvantage compared to some other countries, such as United Kingdom of Great Britain and Northern Ireland, where such data were readily available. However, we saw this as an opportunity to assess VE in an accurate manner by prospectively collecting data that were not readily available and by being able to set a clear clinical case definition to reduce bias caused by unclear definitions. Specifically, for the FASCINATE study, we collected past behavioural data such as attendance at social gatherings that could potentially have been associated with both exposure (for example, the likelihood of vaccination or change in behaviour post-vaccination) and outcome (the likelihood of infection). In fact, the FASCINATE study also aimed to elucidate sociobehavioural factors associated with SARS-CoV-2 infection, which turned out to be important in adjusting for potential biases. (9) For the MOTIVATE study, we collected data on whether medical intervention, such as oxygen use, was due to COVID-19 or other diseases among those who tested positive for SARS-CoV-2, (13) since incidental infection found at the time of hospital admission with unrelated conditions was an issue in using a database to conduct VE studies. (17)
The third challenge was that of evolving epidemiological biases and confounders (Table 2). Due to the prospective nature of the study, we were able to mitigate the majority of these, but the risk of residual bias was considered high in the Philippines study results. A reason for this included the likelihood that most unvaccinated individuals were infected before the study’s initiation (which was immediately after the first Omicron surge, which probably afforded better protection compared to vaccination several months earlier, and differential sociodemographic and risk behaviour status between the vaccinated and the unvaccinated.
The final challenge was the timeline. There was a substantial delay in study initiation in the Philippines. What took time was the alignment with various stakeholders and institutional review board (IRB) approval. Following IRB approval, a memorandum of agreement as well as a non-disclosure agreement needed to be signed and validated by the hospital’s legal department with apostille required. Recruitment was also a challenge, as the investigation started right after the Omicron surge. In Japan, we were able to initiate the study and publish reports in a relatively timely manner to inform policy and risk communication. However, it was not always possible to respond to the rapidly evolving policy and communication needs, especially on VE against severe disease.
For future epidemics and pandemics, preparedness during the inter-epidemic/inter-pandemic periods will be critical so that interventions such as vaccination can be rapidly evaluated when such health emergencies occur. Based on our experience, we summarized three main lessons learned. First is the importance of establishing and maintaining platforms to rapidly evaluate interventions such as vaccination. Ideally, these would be incorporated into public health surveillance (for example, ILI or SARI surveillance) and carried out via prospective data collection. The prospective approach would ensure a clear case definition and collection of essential information, such as relevant potential confounders. If this is not feasible, clinical research networks such as the International Severe Acute Respiratory and emerging Infection Consortium and/or a unified database that can link exposure and outcome data (as well as genomic characterization of infections) may be considered. Specifically, setting up these platforms and monitoring epidemics, such as seasonal influenza and respiratory syncytial virus infection, during the inter-emergency/pandemic period in advance is critical, as these can rapidly be applied to newly emerging respiratory infections with pandemic potential. The second lesson is the usefulness of uniform and practical protocols with careful and agile consideration of biases and confounders to conduct clinical research based on policy and risk communication needs, which would also allow for cross-comparison of studies. A guidance document on VE studies was published by WHO, (5, 17) but it was generic in nature. Therefore, some of the authors at the WHO Regional Office for the Western Pacific prepared a practical protocol, which was used as a basis for a VE study in Viet Nam. The third lesson is the value of communication with all potential stakeholders including IRBs during the inter-emergency/pandemic period to pre-approve generic clinical study protocols that can then be expedited when a health emergency occurs, although incorporating VE evaluation into public health surveillance may eliminate this need.
During health emergencies, responding to the event itself is the priority, and conducting operational studies may seem less important. However, evidence-based decision-making is key to a successful response, and such studies are exactly what inform health emergency response.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1COVID-19 vaccine effectiveness. Geneva: World Health Organization; 2024. Available from: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/surveillance/covid−19-vaccine-effectiveness-and-impact, accessed 1 January 2024.
- 2COVID-19 vaccine trial designs in the context of authorized COVID-19 vaccines and expanding global access: ethical considerations. Geneva: World Health Organization; 2021. Available from: https://www.who.int/publications/i/item/WHO−2019-n Co V-Policy-brief-Vaccine-trial-design−2021.1, accessed 1 January 2024.
- 3Andrews N, Tessier E, Stowe J, Gower C, Kirsebom F, Simmons R, et al. Duration of protection against mild and severe disease by Covid-19 vaccines. N Engl J Med. 2022 Jan 27;386(4):340–50. 10.1056/NEJ Moa 211548135021002 PMC 8781262 · doi ↗ · pubmed ↗
- 4Andrews N, Stowe J, Kirsebom F, Toffa S, Rickeard T, Gallagher E, et al. Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N Engl J Med. 2022 Apr 21;386(16):1532–46. 10.1056/NEJ Moa 211945135249272 PMC 8908811 · doi ↗ · pubmed ↗
- 5Evaluation of COVID-19 vaccine effectiveness: interim guidance. Geneva: World Health Organization; 2021. Available from: https://www.who.int/publications/i/item/WHO−2019-n Co V-vaccine_effectiveness-measurement−2021.1, accessed 1 January 2024.
- 6Reichert TA, Sugaya N, Fedson DS, Glezen WP, Simonsen L, Tashiro M. The Japanese experience with vaccinating schoolchildren against influenza. N Engl J Med. 2001 Mar 22;344(12):889–96. 10.1056/NEJM 20010322344120411259722 · doi ↗ · pubmed ↗
- 7Simms KT, Hanley SJB, Smith MA, Keane A, Canfell K. Impact of HPV vaccine hesitancy on cervical cancer in Japan: a modelling study. Lancet Public Health. 2020 Apr;5(4):e 223–34. 10.1016/S 2468-2667(20)30010-432057317 · doi ↗ · pubmed ↗
- 8Larson HJ, Hartigan-Go K, de Figueiredo A. Vaccine confidence plummets in the Philippines following dengue vaccine scare: why it matters to pandemic preparedness. Hum Vaccin Immunother. 2019;15(3):625–7. 10.1080/21645515.2018.152246830309284 PMC 6605722 · doi ↗ · pubmed ↗