Exercise Crystal: simulations that drive National IHR Focal Point capacity-strengthening
Laura Goddard, Qiu Yi Khut, Gina Samaan

Abstract
The International Health Regulations (2005; IHR) require States Parties to designate a National IHR Focal Point (NFP; i.e. a national centre) to ensure timely communications with the World Health Organization (WHO) about all events that may constitute a public health emergency of international concern and, following recent amendments, to designate a National IHR Authority to coordinate IHR (2005) implementation within the Parties. Since 2008, the WHO Regional Office for the Western Pacific has been running an annual simulation exercise, known as the IHR Exercise Crystal, to test and strengthen NFP functionality. This study analyses NFP performance during the IHR Exercise Crystal over a 16-year period (2008–2024, excluding 2009) to inform Member States’ planning for NFP capacity-strengthening in the context of the recent IHR (2005) amendments. Data collected about NFP performance during…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
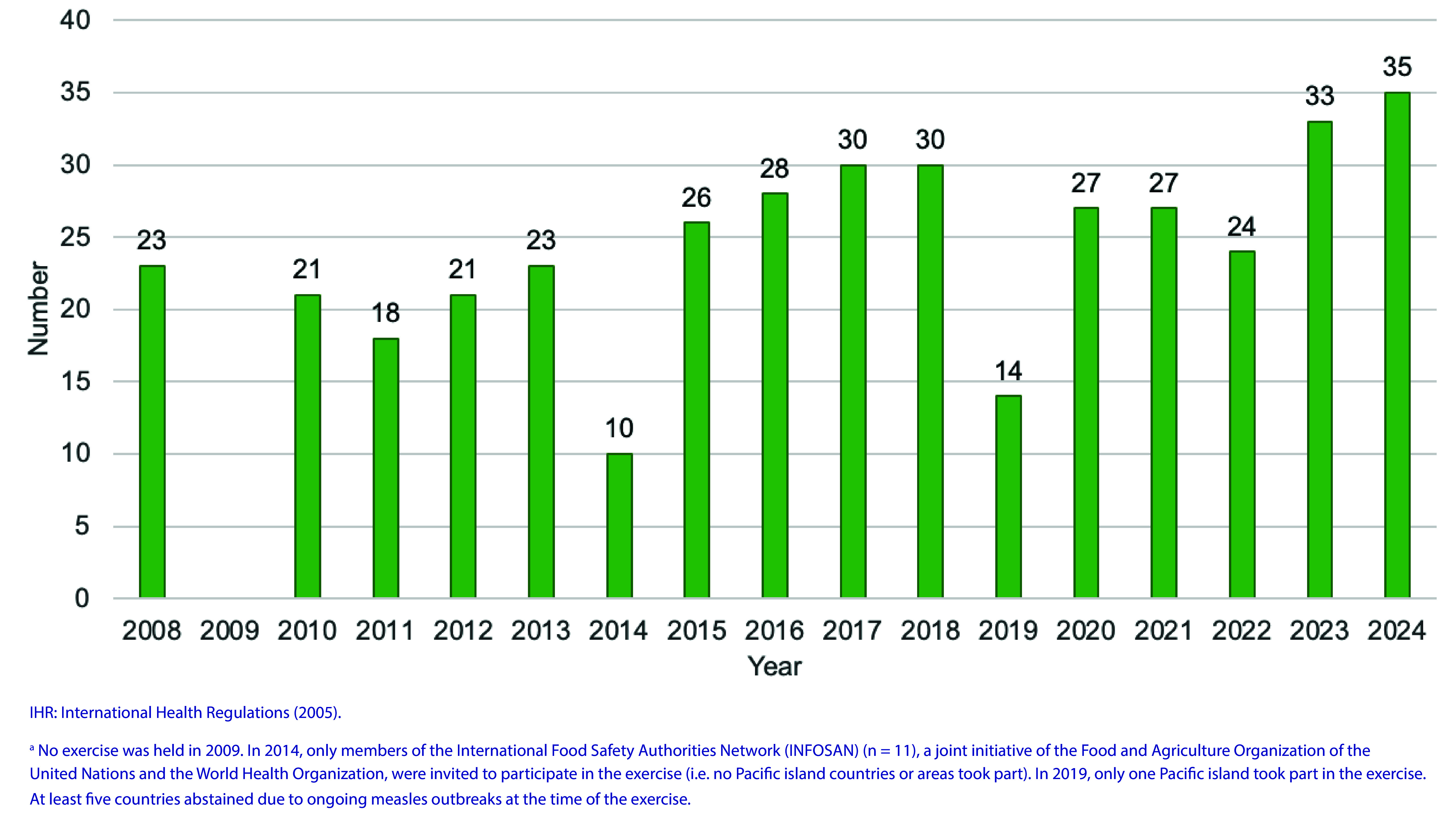 Fig. 1
Fig. 1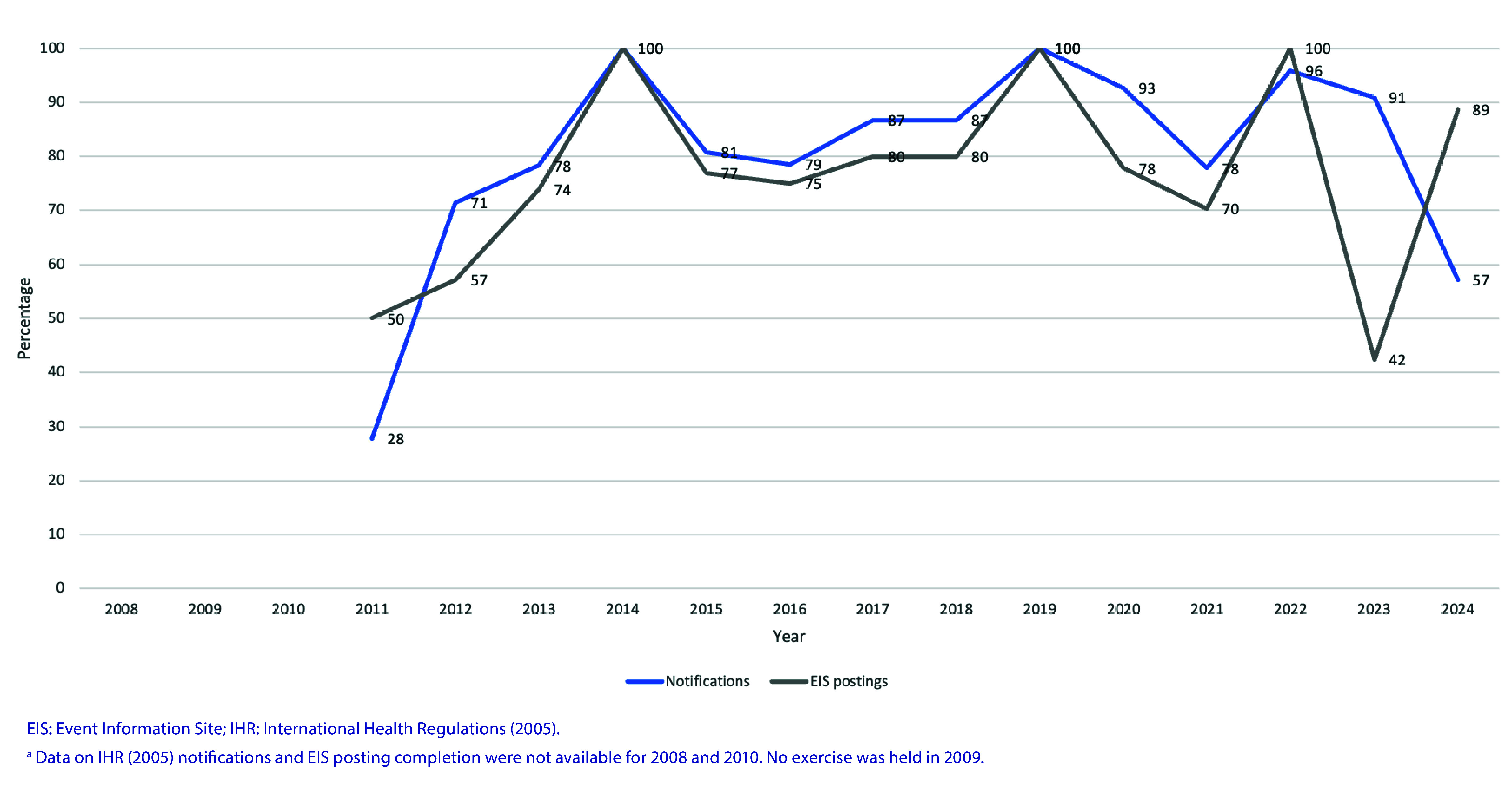 Fig. 2
Fig. 2| Objetive | Year | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
| Variable | Definition |
|---|---|
| The IHR NFP or Contact Point could be successfully contacted by e-mail during the exercise, either through registered contact details or alternative details that had been provided. | |
| Telephone | The IHR NFP or Contact Point could be successfully contacted by telephone during the exercise, either through registered contact details or alternative details that had been provided. |
| Tele- or videoconference | The IHR NFP or Contact Point could successfully join a tele- or videoconference call, held at the beginning or conclusion of the exercise. |
| Notification | The IHR NFP or Contact Point e-mailed the WHO IHR Contact Point to notify the public health event during the exercise. |
| EIS postinga | The IHR NFP or Contact Point e-mailed the WHO IHR Contact Point to share information about the public health event during the exercise for inclusion in an EIS posting. |
| Multisectoral communication | During the exercise, the IHR NFP or Contact Point contacted either the exercise Simulatorb instead of another agency or sector within their country, or a specifically nominated agency, during the exercise. |
| Year | Scenario | No. (%) of participantsa | Variableb | |||||
|---|---|---|---|---|---|---|---|---|
| Telephone | Tele- or video-conferencing | IHR (2005) notificationc | EIS postingc | Multisectoral | ||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Verocytotoxin-producing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Novel |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Public Health Policies and Epidemiology · Delphi Technique in Research
The International Health Regulations (2005; IHR) define countries’ rights and obligations in handling public health events and emergencies that have the potential to cross borders. (1) Signatory States Parties commit to developing core capacities for public health emergencies and, under Article 4, are required to designate or establish a National IHR Focal Point (NFP; i.e. a national centre) to communicate with the World Health Organization (WHO). The NFP must be accessible at all times to communicate with WHO IHR Contact Points and is responsible for sending information to WHO on behalf of States Parties, as well as disseminating information to, and consolidating input from, relevant sectors of the Party’s administration. (1, 2) In the case of territories and areas, States Parties may establish IHR Contact Points specific to each territory or area for the purpose of IHR (2005) communications, although this is not mandatory under the IHR (2005).
IHR (2005) communications and the role of the NFP are central to the Regulations and to global health security. In the recent amendments to the Regulations, which were approved by Member States in June 2024, the requirement to designate or establish an NFP has remained unchanged. (3) However, States Parties must now designate or establish a National IHR Authority, which may be the same entity as an NFP, or a different entity, to coordinate implementation of the Regulations within the State Party. (3) Therefore, in some countries the designation of a National IHR Authority may have an impact on current NFP practices or operations.
In the WHO Western Pacific Region, IHR (2005) implementation is supported through the Asia Pacific Health Security Action Framework (APHSAF). (4) Progress in implementing the IHR (2005), including the NFP and other core capacities, is assessed and monitored through the mandatory States Parties Self-Assessment Annual Report (SPAR) and voluntary assessments, including Joint External Evaluations, simulation exercises, and intra- and after-action reviews. (1, 5) These assessments help to identify strengths and areas for improvement and then translate them into priority actions as part of national planning to build a country’s capacities. (6)
In the Western Pacific Region, the functioning of NFP capacities is routinely assessed through an annual simulation exercise organized by the WHO Regional Office for the Western Pacific. IHR Exercise Crystal has been running since 2008 and aims to test IHR (2005) communication channels and familiarize NFPs and WHO staff with the IHR communication system. (7) Findings from the exercise can inform actions needed to strengthen NFP functionality and should be triangulated with other assessments to better understand the capacity level of countries and to implement priority actions at the national and subnational levels. (5)
This analysis describes the performance of IHR NFPs and Contact Points in the Western Pacific Region during IHR Exercise Crystal over time, with the aim of informing Member States’ planning as they prepare for implementing the IHR (2005) amendments.
Methods
Study design
We conducted a descriptive analysis of IHR NFP and Contact Point performance during IHR Exercise Crystal over a 16-year period (2008–2024, excluding 2009).
Study population and setting
The Regional Office works with health authorities from 37 countries and areas, of which 22 are Pacific island countries and areas, totalling more than one quarter of the world’s population. (8) The Region is very diverse; significant variations exist in Member States’ geography, demographics, health systems and services, disease burden and disaster risk profiles. (9-11) There are, however, many common challenges and approaches that countries and areas in the Region share, including a common approach to IHR (2005) implementation and capacity development through APHSAF. (4)
Data sources and analysis
Data about NFP performance during IHR Exercise Crystal were extracted from reports and monitoring data sets for the years 2008–2024. Monitoring and evaluation data have been collected each year of IHR Exercise Crystal to measure IHR NFP and Contact Point performance against the exercise’s objectives (Table 1); however, when monitoring data sets were not available – for 2008, 2010, 2019 and 2021 – only exercise reports were used.
The study used descriptive statistics to summarize and describe the performance of IHR NFPs and Contact Points in the Western Pacific Region during the exercise for six key variables relating to NFP functions (Table 2). For each variable, the number and percentage of countries meeting the criteria were calculated for each year, and the mean was calculated for all years. These variables assess whether the IHR NFP or Contact Point is available by e-mail or telephone, or through teleconferencing or videoconferencing; whether they notified WHO about the public health event during the exercise; whether they prepared information to share via the Event Information Site (EIS) for NFPs; and whether they engaged with other stakeholders during the exercise.
Results
Between 2008 and 2024, IHR Exercise Crystal was held 16 times. No exercise was held in 2009; however, during 2009, NFPs communicated frequently with the WHO IHR Contact Point on pandemic influenza A(H1N1), which was a public health emergency of international concern. Additionally, in 2014, an exercise was held with the International Food Safety Authorities Network (INFOSAN), jointly governed by the Food and Agriculture Organization of the United Nations and WHO, which was limited to the then-11 INFOSAN member countries. In 2019, at least five countries were unable to participate in the exercise due to measles outbreaks, leading to a lower participation rate that year. Eleven of the 16 exercise scenarios were related to outbreaks of respiratory viruses (Table 3). From 2008 to 2015 (excluding 2014, only States Parties (n = 27) to the IHR (2005) in the Region were invited to participate, with an average of 22 participating countries and areas (range: 18–26) taking part each year. From 2016 onwards, all 37 countries and areas in the Region were invited to participate, with an average of 28 (range: 14–35) taking part each year (Fig. 1). Mean participation for the period 2008–2024 (including 2014) was 78% (Table 3).
Number of countries and areas participating in IHR Exercise Crystal, by year, 2008–2024a
The proportion of participating countries and areas that were accessible via e-mail was consistently high, with a mean of 99% for the period 2008–2024 (Table 3). However, the proportion of participating countries and areas that were accessible via telephone has been suboptimal, with a mean of 64% for the period of 2008–2024 (Table 3). The proportion of participating countries and areas that joined a teleconference or a videoconference (first introduced in 2015) with the Regional Office during the exercise improved over time, with 85% or more successfully attending between 2021 and 2024, for a mean of 73% over the entire period 2008–2024 (Table 3).
The proportion of participating countries and areas notifying the simulated event to the WHO IHR Contact Point has improved over time, with some variation between years. Between 2008 and 2024, a mean of 80% of participating countries and areas notified the simulated event to WHO (Fig. 2). The proportion of participating countries and areas that contributed information to an EIS posting has typically followed a similar trend to that of notifications, with some variation in 2023 and 2024. Between 2008 and 2024, a mean of 77% of participating countries and areas contributed information to an EIS posting (Fig. 2).
Percentage of participating countries and areas completing IHR (2005) notifications and EIS postings during IHR Exercise Crystal, by year, 2008–2024a
Data for the variable about multisectoral communication were limited for the period 2008–2024, as this was not an objective of IHR Exercise Crystal for 6 of the 16 years (Table 1). Although no clear trend in the capacity of NFPs to conduct multisectoral communication was observed over time, the mean performance was 73% for the 9 years of data (Table 3). Furthermore, where data were available, the proportion of NFPs engaging in multisectoral communication was lowest for the scenarios based on a radiological event, and vector-borne disease and non-influenza respiratory disease outbreaks caused by Francisella tularensis and novel coronavirus, and highest for infectious disease outbreaks involving a novel influenza virus or gastroenteritis (Table 3).
Discussion
Since its beginning in 2008, IHR Exercise Crystal has seen strong participation from Member States in the Western Pacific Region, and several key NFP performance indicators have been tracked over time. Our analysis of these indicators demonstrates that the requirement for 24/7 accessibility of NFPs through their registered contact details continues to be a challenge. E-mail has proven to be the most effective means of communication, with a mean of 99% of NFPs successfully being contacted by e-mail, compared with a mean of 64% of NFPs successfully being contacted by telephone. The proportion of NFPs who are able to join the exercise by tele- or videoconferencing has improved over time. These trends are consistent with previous findings about contacting NFPs in the Region (12) and demonstrate that while NFPs’ performance has continued to improve, there remains a need to regularly test and update NFPs’ contact details, at least annually. This is supported by a global survey of States Parties conducted in 2019, which found that communications was one of four critical areas in which NFPs experienced challenges. (13)
Similarly, our finding that the proportion of NFPs notifying simulated public health events to the WHO IHR Contact Point and the proportion of NFPs contributing information to EIS postings have improved over time is consistent with findings from other studies. (12-14) In a study of IHR (2005) States Parties, most (96%) NFPs reported that they were familiar with how to contact their designated WHO IHR Contact Point and that they had the necessary content expertise to discuss a notifiable event with the WHO IHR Contact Point. (13) In another study, 88% of NFPs reported that they had excellent or good knowledge of the Annex 2 decision-making instrument and either excellent (23%) or good (44%) ability to assess potential public health emergencies of international concern under Annex 2. (14) The strong performance in this NFP capacity is likely due to the long-term investments made by WHO and States Parties in institutionalizing the use of Annex 2 through training, guidance documents and standard operating procedures, as well as the development of legal, regulatory or administrative provisions supporting its use. (15-18) However, efforts should be continued to reinforce this capacity and ensure that it is consistently applied across all hazards. This need is highlighted by the decrease in EIS submissions during the 2023 Exercise Crystal, which featured a radiological event.
Our analysis did not find a clear trend in NFPs’ capacity to engage in multisectoral communication; however, on average, 73% of NFPs communicated with another sector or agency during exercise play. It had been previously identified that NFPs experience challenges in intersectoral collaboration within their countries, including having limited access to or experiencing a lack of cooperation from key ministries (13) and that NFPs were not sufficiently empowered to carry out their functions, (13, 19, 20) which creates difficulties in engaging directly with other agencies or sectors and in triggering decision-making processes by national health authorities. (20) For these reasons, it has been recommended that States Parties establish a National IHR Authority that will focus on implementing the IHR (2005) across sectors at the national level, recognizing that the core capacities of the Regulations extend beyond the health sector. (20, 21) Although the roles and functions of NFPs do not change under the June 2024 amendments, (3) the added requirement to designate or establish a National IHR Authority means that it will be even more important to ensure roles and responsibilities are clearly delineated and that States Parties develop, test and maintain up-to-date standard operating procedures, particularly in relation to multisectoral communication and coordination.
States Parties should also continue strengthening and empowering NFPs to conduct their core functions of IHR (2005) communications. Tools such as SPAR and IHR Exercise Crystal can guide continual improvements in NFP functionality, while highlighting the need for a critical foundation of supporting legislation and sufficient resourcing. (22) Furthermore, APHSAF advocates for strengthening the mandate and capacities of NFPs, by ensuring that they are prepared and ready to respond to public health emergencies (e.g. through regular testing), and by enhancing communication, information-sharing and coordination between the National IHR Focal Point system and emergency contacts for other areas and sectors, as well as between countries. (4)
Limitations of this analysis include the inability to capture multisectoral communications that occur outside of e-mail communications observed during an exercise and variations over time in the methods used for monitoring and evaluating IHR Exercise Crystal. Therefore, it is important to consider triangulation with multiple data sources, such as SPAR, when analysing and interpreting the results of simulation exercises. Furthermore, as this study measured IHR (2005) communications in a simulation setting, actual NFP performance in real events may vary due to real-world complexities not reflected in the exercises.
Conclusions
Between 2008 and 2024, States Parties in the WHO Western Pacific Region demonstrated improved NFP capacities in the areas of IHR (2005) notification, contributing information to EIS postings, and participating in tele- and videoconferencing. Continued strengthening is required, particularly in the areas of NFP accessibility and multisectoral communications, alongside ongoing efforts to standardize data collection and assessments. Simulation exercises such as IHR Exercise Crystal are one tool that States Parties can use to assess NFP capacities and guide improvements. NFP functions do not change in the context of the IHR (2005) amendments and the designation or establishment of a National IHR Authority; however, States Parties should clearly define each entity’s responsibilities, and develop and test operational procedures to ensure that NFPs continue to function without disruption. This is critical to advancing health security and IHR (2005) implementation in the Region.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Health Regulations. (2005), third edition. Geneva: World Health Organization; 2016. Available from: https://iris.who.int/handle/10665/246107, accessed 10 December 2024.
- 2National IHR Focal Point guide: designation/establishment of National IHR Focal Points. Geneva: World Health Organization; 2006. Available from: https://www.who.int/publications/m/item/designation-establishment-of-national-ihr-focal-points, accessed 10 December 2024.
- 3International Health Regulations. (2005). Part I – definitions, purpose and scope, principles and responsible authorities. Seventy-seventh World Health Assembly, agenda item 13.3. Geneva: World Health Organization; 2024. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA 77/A 77_ACONF 14-en.pdf, accessed 11 December 2024.
- 4Asia Pacific health security action framework. Manila: WHO Regional Office for the Western Pacific; 2024. Available from: https://iris.who.int/handle/10665/377083, accessed 11 December 2024.
- 5International Health Regulations. (2005): IHR monitoring and evaluation framework. Geneva: World Health Organization; 2018. Available from: https://iris.who.int/handle/10665/276651, accessed 12 December 2024.
- 6World Health Organization strategy (2022–2026) for the National Action Plan for Health Security. Geneva: World Health Organization; 2022. Available from: https://iris.who.int/handle/10665/365581, accessed 12 December 2024.
- 7Crystal E. ten years of strengthening communication between countries and WHO during emergencies. Geneva: World Health Organization; 2018. Available from: https://www.who.int/westernpacific/news-room/feature-stories/item/exercise-crystal-ten-years-of-strengthening-communication-between-countries-and-who-during-emergencies, accessed 12 December 2024.
- 8Where we work. Manila: WHO Regional Office for the Western Pacific; 2024. Available from: https://www.who.int/westernpacific/about/where-we-work, accessed 20 January 2025.