The use of extended reality in microsurgical free flap planning – A systematic review
Kristian Havndrup Rasmussen, Magnus Balslev Avnstorp, Peter Sinkjær Kenney, Nicco Krezdorn, Michael Rose

TL;DR
This paper reviews how extended reality (XR) technologies like virtual and augmented reality can help plan complex microsurgical procedures more effectively than traditional imaging methods.
Contribution
The study systematically evaluates the current use and effectiveness of XR in microsurgical free flap planning, highlighting workflow and accuracy improvements.
Findings
Virtual reality offers better anatomy visualization and is more time-efficient than CT angiography.
Augmented reality is more accurate and faster than Doppler ultrasound.
Successful XR use requires a well-designed workflow.
Abstract
Dissecting free tissue flaps can be challenging and time-consuming. Imaging technologies are typically used to assist with preoperative planning. However, conventional methods have limitations that could potentially be overcome by extended reality technologies. This systematic review aimed to evaluate the current use of extended reality (XR) in preoperative planning for microsurgical free flaps and assess its effectiveness as a tool in this context. The systematic review was conducted following the preferred reporting items of systematic reviews and meta-analyses guidelines. Articles identified through the PubMed, Ovid, Web of Science, and Scopus databases were screened based on titles and abstracts, and relevant articles were assessed in full text. Inclusion criteria were: use of XR for vascular visualization in plastic and reconstructive surgery, reported workflow, accuracy,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
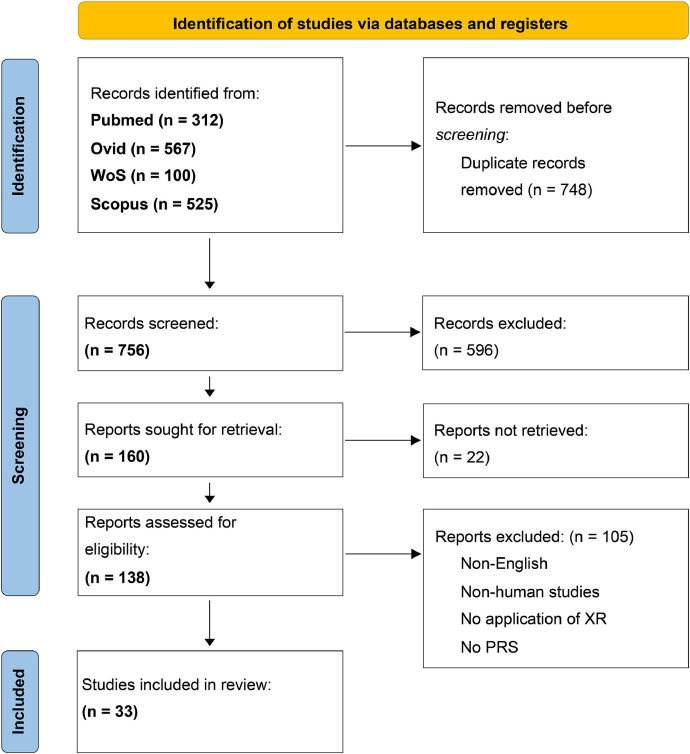 Figure 1
Figure 1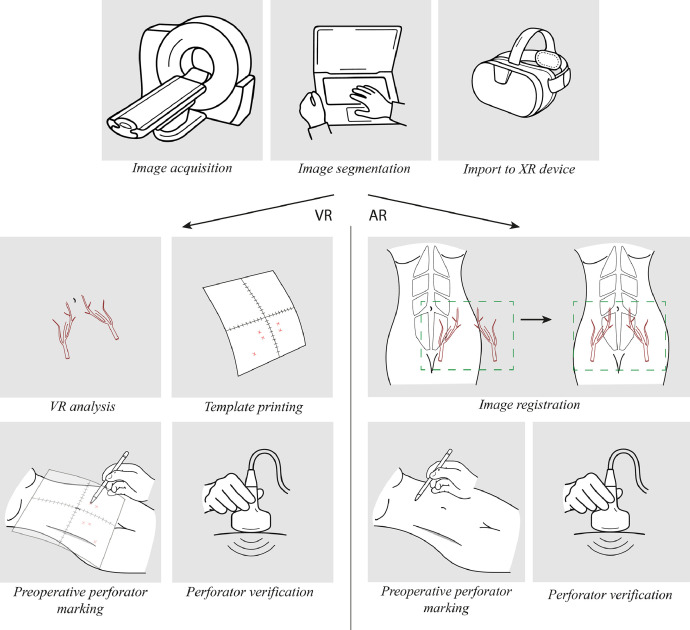 Figure 2
Figure 2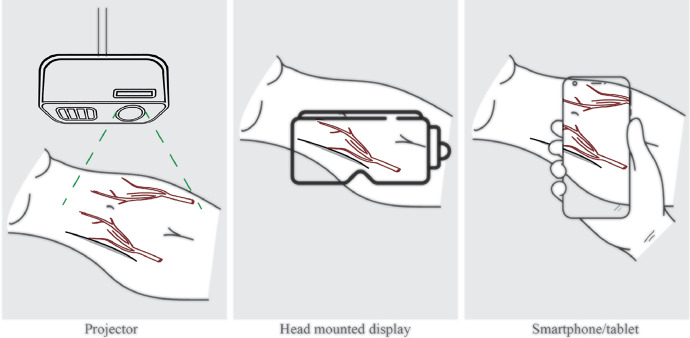 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Facial Trauma and Fracture Management · Surgical Simulation and Training
Introduction
In microsurgical reconstruction, meticulous dissection of the perforator vessels supplying the flap tissue is crucial. The dissection of these vessels can be difficult and time-consuming.1 If executed improperly, damage to the vessels could result in flap loss or other complications such as partial necrosis or hematoma. Additionally, it is important to account for the variations in the vascular anatomy when raising free flaps such as a deep inferior epigastric artery perforator (DIEP).2 Identifying and localizing relevant perforators is crucial in optimizing flap survival and minimizing complication rates and procedure times.
Different techniques have been used for preoperative planning of free flaps, including Doppler ultrasound,3^,^4 color duplex scanning,5 and computed tomography angiography (CTA),6^,^7 the latter is generally considered the gold standard. Additionally, 3D rendered CTAs can be used.8 Magnetic resonance angiography (MRA) has also been used for perforator identification with accurate results.9 Non-imaging methods evaluating target perforators intraoperatively has also been proposed.10 However, conventional imaging methods continue to have some limitations, including the transfer of information from modalities, such as CTA or MRA to the patient, and lack of opportunities for intraoperative navigation. New methods to overcome these limitations could possibly improve preoperative planning, intraoperative guidance, and surgical outcomes, including operative time and complication rates.
Extended reality (XR) refers to technologies capable of combining real-world objects with digital objects to varying degrees. XR encompasses virtual reality (VR), a completely virtual environment, and augmented reality (AR), a mixed real environment with digitally overlayed images. XR images can be generated from data obtained from CTA or MRA, providing surgeons with novel means of interacting with the data.
XR technologies have shown promise as tools for preoperative planning and intraoperative navigation within several surgical specialties such as orthopedic hip surgery, spine surgery, urology, and neurosurgery.11, 12, 13, 14
In this systematic review, we aimed to examine the utilization of XR technologies in the context of perforator localization within plastic and reconstructive surgical procedures. We sought to address its performance compared to other methods with respect to aspects such as workflow, accuracy, operative time, and complications.
Methods
This systematic review was authored in accordance with the preferred reporting items of systematic reviews and meta-analyses (PRISMA) guidelines.15
Research question
This systematic review sought to answer the following research question:“In the context of perforator identification in plastic and reconstructive free flap surgery, how does the utilization of extended reality compare to other non-extended reality technologies regarding user experience and clinical outcomes?”
Systematic literature search
A systematic literature search was conducted by the primary author, KHR, on October 18, 2023 and updated on December 1, 2023 and October 18, 2024. The literature search was designed around the research question using 2 search blocks, incorporating the search terms related to XR technologies and plastic and reconstructive free flap surgery. These 2 search blocks were linked with the Boolean operator “AND.” Details of the systematic literature search are provided in Supplementary Information 1.
The systematic literature search was performed across 4 databases: PubMed, Ovid, Web of Science and Scopus. Subsequently, a de-duplication process was carried out using EndNote 20, following the methodology described by Bramer et al.16. The resultant articles were manually and critically appraised by the author, KHR, using the Covidence screening tool (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org). Initially, the articles were screened based on titles and abstract, and relevant articles were retrieved and assessed based on the full text.
Inclusion criteria for the studies were: Utilization of XR for vascular visualization, plastic and reconstructive surgical procedures or simulation of one, report on workflow, accuracy, preoperative or intraoperative time, and surgeons’ opinion of XR or complications. Articles not available in full text, not written in English, non-human studies, or review articles were excluded.
Data extraction
Data extracted by the primary author, KHR, included title, authors, year of publication, study design, XR technique, imaging modality, the setting in which XR is applied, population size, flap type, and outcomes included accuracy of examined XR modality, postoperative complications, preoperative or intraoperative times, workflow, and surgeons’ opinions on the technology.
This review included studies that lacked quantitative data but instead provided descriptive accounts of the workflow related to the implementation of XR technologies in plastic and reconstructive flap surgery. Although these studies lack data, they were included to offer insights into the process of incorporating these technologies in surgical procedures.
Synthesis
The included studies were grouped depending on the type of XR modality used. Among the 33 included studies, 7 used VR and 26 used AR. Outcome data were standardized and compared. Outcome data are presented in Table 1, Table 2.Table 1. Characteristics of the included studies in the VR groupTable 1Author(s)Imaging modalityStudy designSettingPopulation sizeProcedureCEBM levelOutcomeJBI scoreP. Gacto, et al.20CTACase reportPreoperative planningn = 1ALT flap5Total match between VR visualized dominant perforator and intraoperative findings0 postoperative complications5/8Gacto-Sanchez, et al.21CTACohort study (consecutive patients)Preoperative planningn = 12DIEP flap3100% correlation between preoperatively selected perforator and intraoperative findingsError of VR perforator localization compared with intraoperative findings:Mean error = 0.23 cm (95% CI, 0.17-0.30)Perforator <4 cm from the umbilicus: Mean error = 0.17 cm (95% CI, 0.09-0.024)Perforator >4 cm from the umbilicus: Mean error = 0.31 cm (95% CI, 0.21-0.42)5/11C. Suárez-Mejías, et al.22CTACohort studyPreoperative planningn = 35 (consecutive)DIEP flap3Mean operative timeCTA-VirSSPA = 478 min (SD 56.94)Control (Doppler) = 606.29 min (SD 81.94)(p < 0.001)Flap related postoperative complicationsCTA-VirSSPA = 0Control = 14(p < 0.001)Donor site complicationsCTA-VirSSPA = 2Control = 15(p = 0.001)7/11T. Suffee, et al.23CTACase series (prospective)Preoperative planningn = 30 (33 flaps), consecutiveDIEP flap4Perforator chosen by radiologist (CTA): 16/30 (53%)Perforator chosen by surgeon (VR): 10/30 (33%)Concordance of best perforator between VR and CTA = 33 %8/10G. De la Cruz-Ku, et al.26MRICase reportPreoperative planningn = 1NSM + Recon-struction53 perforators identified in the breast preoperatively, all of these were conserved during surgery6/8D. Freidin, et al.25CTACase series (prospective)Preoperative planningn = 30 (42 flaps)DIEP flap4Surgeons’ rating of VR vs. CTA in preoperative planningModified surgical plan after VR assessment in 4/42 flaps, no complications were reportedFlap loss in 1/42 flapsMinor complications in 6/42 flaps6/10A. Di Via Ioschpe, et al.24CTARetrospective case seriesPreoperative planningn = 44DIEP flap, SIEA flap4Pearson correlation between VR and CTA based on distance of perforator from umbilicus:Unilateral perforator: R = 0.960, p < 0.001Bilateral perforators: R = 0.930, p <0.001Time spent on interpretation of images:CTA: Average 60 minVR (first 10 patients): 37 minVR (next 20 patients): 9.3 min7/10Abbreviations: ALT, anterolateral thigh; CTA, computed tomography angiography; DIEP, deep inferior epigastric artery perforator; NSM, nipple-sparing mastectomy; SIEA, superficial inferior epigastric artery; VR, virtual realityTable 2Characteristics of the included studies in the AR groupTable 2ReferenceAR typeImaging modalityStudy designSettingPopulation sizeProcedureCEBM levelOutcomeJBI scoreS. Battaglia, et al.27TabletCTACase series (consecutive)Preoperative planning/intraoperative navigationn = 3FF flap4Description of workflow3/10S. Battaglia, et al.28TabletCTCase seriesPreoperative planningn = 8Pedicled flap40 flap-related postoperative complications1 non-flap-related postoperative complication (temporary paralysis of facial nerve)4/10A. Fitoussi, et al.31TabletCTProof of conceptPreoperative planningn = 12 (26 perforators)DIEP flap5Median distance between AR and Doppler markings 2 mmMedian distance between AR and CTA markings: 2.5 mm92% of the AR markings were ≤1 cm from Doppler markingNo total flap loss or partial necrosisN. Pereira, et al.41SmartphoneCTACohort studyPreoperative planningAR group:n = 30 (60 inguinal areas)Non-AR group: n = 15SCIP flap3100% correlation between AR and Doppler markings for DIEP, sSCIP and dSCIP100% correlation with AR markings with intraoperative findings (30/30)Average flap harvest time reduced by 20% from 90 min (Doppler) to 72 min (AR)6/11N. Pereira, et al.42SmartphoneCTAProspective case seriesPreoperative planningn = 89 (101 flaps)SCIP flap4Postoperative complications after implementing AR to SCIP flap:9/101 revision surgeries6/101 flap losses12/101 partial flap losses2/101 wound dehiscence1/101 hematoma1/101 seroma8/10N. Pereira, et al.47SmartphoneCTAProof of conceptPreoperative planningn = 15 (30 thighs/groins)SCIP flap5AR images showed 100% correlation to Doppler ultrasoundS. Hummelink, et al.32ProjectorCTATechnical reportPreoperative planningn = 9DIEP flap5Audible Doppler signal at AR marking in 98/100Correctly identified perforators84.3% ± 25.8% (AR) vs. 56.9% ± 31.4% (Doppler) (p = 0.030)Average distance from marking to intraoperative findings:4 mm ± 3 mm (AR) vs. 7 mm ± 4 mm (Doppler; p = 0.009)S. Hummelink, et al.34ProjectorCTACase seriesPreoperative planningn = 10DIEP flap4Description of workflow7/10S. Hummelink, et al.35ProjectorCTAProof of conceptPreoperative planningn = 6 (9 breasts)DIEP flap5Audible Doppler signal at AR marking in 41/420 complicationsM. P. Chae, et al.29ProjectorCTACase seriesPreoperative planningn = 6ALT flap3, TUG flap1, DIEP flap24Description of workflow2/10I. J. Cifuentes, et al.51ProjectorDIRTProof of conceptPreoperative planningn = 3 (6 thighs)ALT flap5100% correlation of AR projection and Doppler signalTime needed to identify perforators via AR 3.5 min (range 3.3-4.0 min)S. Hummelink, et al.33ProjectorCTARCTPreoperative planningn = 49 (69 flaps) Projection: n = 28 (40 flaps) Doppler: n = 21 (29 flaps)DIEP flap2Mean preoperative perforator localization time:2.3 ± 0.8 (AR) vs. 20 ± 5.5 min (Doppler,p = 0.001)Correctly identified perforators:61.7 ± 7.3 (AR) vs. 41.2 ± 8.2 (Doppler,p = 0.020)Flap harvest time:136 ± 7 (AR) vs. 155 ± 7 (Doppler, p = 0.012)No significant difference in complications between the 2 groups9/13J. Martschinke, et al.38ProjectorCTAPilot studyPreoperative planningn = 10DIEP flap5Description of workflowY. F. Tang, et al.44ProjectorCTAProspective cohortPreoperative planningn = 14ALT flap3Accuracy of AR projection vs. Doppler90.2% (37/41) vs. 82.4% 28/34)Sensitivity of AR projection vs. Doppler97.4% (37/38) vs. 73.7% (28/38)Complications:1 patient with infection,1 patient with partial flap necrosis4/11N. Yodrabum, et al.46Projector, smartphoneCTACase seriesPreoperative planningn = 8FF flap4Average error of AR projection vs. Doppler0.7 ± 0.2 cm3/10E. L. Meier, et al.52ProjectorDIRTProof of conceptPreoperative planningn = 50 (71 flaps)DIEP flap5Description of workflowDIRT vs. CTA compared with intraoperative findings: 56.8% (DIRT) vs. 59.8% (CTA) of perforators visualized by imaging corresponded to an intraoperatively located perforator54.7% of direct matches between DIRT and intraoperative perforators appeared within the first 5 emerging hotspotsTotal match between DIRT-based AR, Doppler, CTA, and intraoperative findings in 50.8% of perforators; 62.7% of these emerged within the first 5 DIRT hotspots47.5% of all DIRT hotspots were directly related to a CTA-images perforator27.0% of all DIRT hotspots were related to SIEV/SIEA vessels25.5% of DIRT hotspots were unexplainedM. Katayama, et al.37HMDCTACase reportsPreoperative planningn = 2Lower extremity reconstruction5Difference in depth perception between 2 types of holograms3/8T. R. Jiang, et al.36HMDCTATechnical reportExperimentaln = 7Simulation5Accuracy in illuminated vs. non-illuminated conditions: 2.85 mm vs. 1.35 mm, P = 0.02No significant difference between accuracy in different light intensitiesNo significant difference in accuracy induced by head rotation or walkingT. S. Wesselius, et al.45HMDCTAProof of conceptPreoperative planningn = 1DIEP flap5Description of workflowT. Nuri, et al.40HMDCTACase reportPreoperative planningn = 1ALT flap510 min for alignment of AR overlay1 cm difference between AR and Doppler markingsAR markings corresponded perfectly with intraoperative findings0 postoperative complications4/8I. Seth, et al.43HMDCTACase seriesPreoperative planning/ intraoperative navigationn = 5DIEP flap4Description of workflowTime spent converting CTA to AR-usable file = approx. 60 min per caseImage registration = 7-10 minPerforator markings = 5-7 minPerfect match between AR and Doppler ultrasound in 4/5 casesIn the 1 case with misalignment, CTA was 16 months old and the patient had lost weight5/10M. F. Berger, et al.50HMDMRAPilot studyPreoperative planningn = 10DIEP flap5Description of workflowSUS = 67, qualifying as "moderate to good"G. Masterton, et al.39HMDCTAProof of conceptPreoperative planningn = 2DIEP flap5Description of workflowD. J. Cholok, et al.30HMD, simulatedCTATechnical reportExperimentaln = 19Simulation5Mean difference between naked eye visualization and HMD visualization for 2 points was 9.9 mm (SE 0.106) and 13.7 mm (SE 0.106)F. N. Necker, et al.49HMDCTAProof of conceptPreoperative planningn = 4DIEP flap5Through AR and HMDs, 2 surgeons can be in a shared physical-virtual space and discuss the relevant anatomy and DIEP flap harvest while being at different locationsY. Liu, et al.48HMDCTAExperimentalPreoperative planningn = 40 (20 experimental and 20 control)ALT and fibula osteocutaneous flaps2No statistically significant difference in operative time.Significantly less average blood loss in the AR group compared with the CDU group (24 mL vs. 56 mL).Slightly less recognition rate of perforators in the AR group vs. the CDU group (93.9% vs. 97.2%), non-significantAbbreviations: ALT, anterolateral thigh; CDU, color Doppler ultrasound; CTA, computed tomography angiography; DIEP, deep inferior epigastric artery perforator; DIRT, dynamic infrared thermography; FF, free fibula; HMD, head-mounted display; MRA, magnetic resonance angiography; RCT, randomized controlled trial; SCIP, superficial circumflex iliac artery perforator; SE, standard error; SIEA/SIEV, superficial inferior epigastric artery/vein; SUS, system usability assessment; TUG, transverse upper gracilis
Quality assessment
All articles were assigned a center for evidence-based medicine (CEBM) level of evidence.17 Because of the limited research on XR technologies in plastic and reconstructive surgery, no articles were excluded based on a low CEBM level of evidence. However, readers should consider the low level of evidence of some of the included studies.
Quality assessments were performed using the Joanna Briggs Institute (JBI) Critical Appraisal Tools.
Results
Study selection
The systematic literature search identified 756 articles after de-duplication. After title/abstract and full-text screening, 33 articles met the eligibility criteria and were included in the systematic review. Two articles18^,^19 were excluded as they reported on studies that were covered by 2 other articles. An overview of the systematic literature search is presented in the PRISMA flowchart in Figure 1. Details about the characteristics of the included studies can be found in Table 1, Table 2.Figure 1PRISMA 2020 flowchart*. Abbreviations: 3D = three-dimensional, PRS = plastic or reconstructive surgery, WoS = Web of Science, XR = extended reality*Figure 1:
Quality assessment
CEBM level of evidence
In the VR group, 2 studies ranked as level 3, 3 studies ranked as level 4, and 2 studies ranked as level 5. In the AR group, 2 studies ranked as level 2, 2 studies ranked as level 3, 7 studies ranked as level 4, and 12 studies ranked as level 5.
JBI Critical Appraisal Tools
In the VR group, the cohort studies scored a mean of 6/11 (range 5-7), case series scored a mean of 7/10 (range 6-8), and case reports scored a mean of 5.5/8 (range 5-6). In the AR group, randomized controlled trials (RCTs) scored 9/13, cohort studies scored a mean of 5/11 (range 4-6), case series scored a mean of 4.6/10 (range 2-8), and case reports scored a mean of 3.5/8 (range 3-4).
Some studies were not critically appraised using the JBI Critical Appraisal Tools, as they were designed as proof of concept studies or technical reports; hence, they were included to provide insights into the implementation of XR technologies in plastic and reconstructive surgery.
Workflow of XR-assisted preoperative planning
The workflow of incorporating XR technologies in preoperative planning for microsurgical reconstructive procedures are described in several studies. For VR and AR, some of the steps described below are identical, whereas others differ between the technologies. Moreover, differences in the workflow within VR and AR are described in the literature. A generalized workflow will be introduced below and is illustrated in Figure 2
- 1.Image acquisition Figure 2. Overview of the workflow of XR-based preoperative planningFigure 2:
For VR and AR, image data need to be acquired for processing. In 6 of the included studies on VR, images were based on CTA data.20, 21, 22, 23, 24, 25 In one VR study, MRI was used.26 In the AR studies, CTA was the most used,27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49 while MRA was used in 1 study50 and direct infrared thermography (DIRT) was used in 2 studies.51^,^52 DIRT uses thermal cameras to generate color-coded temperature maps of the tissues, enabling the visualization of perforators, which appear as hotspots in the image.52
When using AR, anatomical landmarks must be identified for later alignment of AR image with the patient (see step 4). Skin landmarks with adhered radiopaque markers have been suggested.45 Other studies suggest landmarks such as the xiphoid process, umbilicus, anterior superior iliac spinae, or superior border of the pubic symphysis.33^,^41^,^50 Additionally, oil fiducials markers, which are glues with oil that can be visualized on MRA, has been suggested as landmarks when using MRA-based AR.50
One study obtained a 3D surface scan of the abdomen to account for soft-tissue deformation, which may improve the accuracy of the AR system.50 In 1 case, a splint was made to fix the extremity in a certain position during scanning and surgery, minimizing the shift between AR overlay and upper extremity position during surgery.37
- 2.Image segmentation
Image data are then imported into computer software for processing. Tissues are segmented to facilitate good visualization of the vessels of interest.22^,^25 The 3D images made through image segmentation are then imported into other types of software such as Blender for manipulation, in which color and transparency can be added or adjusted.37^,^43
- 3.Import to XR device
The 3D image file is then imported into the chosen XR device, which for VR can be either a computer or VR headset, and for AR, it can be either a computer with a projector, smartphone/tablet, or head-mounted display (HMD), which is a glasses-like device with a see-through display capable of superimposing digital data onto the real world (Figure 3).Figure 3. Projector-based AR, HMD-based AR, and smartphone/tablet-based ARFigure 3:
VR workflow
- 4.VR image analysis
VR images are then observed and analyzed by the surgeon. In early VR, these images were viewed on a computer screen.20, 21, 22, 23 In more recent VR, the images are imported into VR 3D glasses, the surgeon uses these glasses to view and analyze the images.24^,^25 The VR images can be viewed from different angles, which allows localization and measurement of the vessels of interest.21^,^24, 25, 26 Thus, the most suitable perforator for flap harvest can be determined.23
- 5.Transfer of anatomical information to patient and preoperative perforator marking
After measurement is carried out in the VR setting, they can be printed as a template scale, which is then transferred to the patient and the anatomy is traced onto the patient.21^,^23 Suffee et al. suggested to verify the appearance of a vessel using Doppler ultrasound.23
AR workflow
- 4.Image registration
The registration process ensures that the overlay of the 3D images corresponds accurately to the real-world anatomy. This alignment is typically performed manually,43^,^50 although automatic methods of alignment have been reported.34^,^38^,^52 This should ideally facilitate complete matching of the superimposed image-based anatomy and real-world anatomy in orientation and size, thereby enabling the initiation of flap preparation.45 Previously identified anatomical landmarks (step 1) are located40^,^45^,^50 using sterilized stainless-steel pointers with a QR marker for HMDs.45 An alternative registration method where the scale of the 3D model is adjusted to match the patient using the umbilicus as a reference point has also been proposed.39
- 5.Preoperative perforator marking
Following registration, the linkage of the holographic anatomy to the patient eliminates the necessity for visible anatomical landmarks, enabling the surgeon to initiate preoperative planning guided by the holographic overlay of the vascular anatomy.45 If relevant to the surgery, other structures such as lymph nodes can also be displayed, as suggested by Hummelink et al.34. Besides using the digital overlay of the vascular anatomy for preoperative planning, some studies also suggest using it intraoperatively for guiding the dissection.27^,^43
One study proposed a method to verify the presence of a perforator at the AR-based perforator marking by examining the area using a Doppler ultrasound unit.39
Virtual reality
Seven studies (24%) investigated VR for preoperative planning of microsurgical flaps.20, 21, 22, 23, 24, 25, 26 Outcome data are presented in Table 1.
Accuracy of VR-assisted preoperative planning
Four studies evaluated the accuracy of VR for preoperative perforator identification.
In determining “the most suitable perforator” for DIEP flaps through preoperative imaging, Suffee et al. found VR to be inferior to CTA.23 Contrastingly, Di Via Ioschpe et al., in a retrospective manner, compared perforator visualization using VR with visualization using CTA and reported a strong correlation between the 2 methods when examining three-dimensional distances.24 The mean error of VR-assisted perforator markings compared to intraoperative findings has been reported to be 0.23 cm, and significantly less for perforators located closer than 4 cm to the umbilicus.21 A case report demonstrated perfect alignment between preoperative perforator markings and intraoperative findings,20 and another case report identified and conserved all preoperatively visualized perforators in the breast.26
Preoperative and intraoperative use of time
Two studies evaluated either preoperative or intraoperative times used in relation to VR for microsurgical reconstruction.
Using VR for preoperative planning of DIEP flap-based breast reconstruction, Suarez-Mejias et al. observed a 21% reduction in total operative time, from 606 to 478 min, compared with Doppler ultrasound-based preoperative planning.22 In addition, Di Via Ioschpe et al. observed a reduction in the time spent to analyze preoperative imaging for 10 patients undergoing abdominal-based free flap, from 60 min using CTA to 37 min using VR. The time used to analyze VR imaging was lesser for the subsequent 20 patients.24
Postoperative complications
Four studies evaluated the rate of postoperative complications following VR-assisted free flap surgery. In one study, VR-assisted DIEP flap planning resulted in significantly less postoperative complications related to the flaps and donor-sites compared to Doppler ultrasound planning, although the type of complications were not specified.22 In other studies, postoperative complications were addressed but failed to provide comparative results to other methods.20^,^23^,^25
Surgeons’ opinions
Freidin et al. compared VR to CTA for preoperative planning of abdominal free flaps for breast reconstruction. A questionnaire based on a 1-5 Likert scale was used. They concluded that in 96.55% of the 30 cases, the surgeons rated VR to provide new information. Overall, 72.4% of the surgeons rated VR to be superior to CTA in terms of similarity to reality. However, in most cases, the surgical plan remained unchanged when visualizing the perforators using VR, suggesting that CTA is a more reliable method for preoperative planning.37
Augmented reality
Twenty-six studies investigated AR for preoperative planning of microsurgical flaps.27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46^,^50^,^51 Outcome data are presented in Table 2.
Accuracy of AR-assisted preoperative planning
Fifteen studies evaluated the accuracy of AR for perforator localization. In general, the accuracy is reported in comparison with either conventional perforator visualization methods or with intraoperative findings (measurements relative to umbilicus).
Five studies compared preoperative AR markings of perforator localization with Doppler markings.30^,^31^,^40^,^46^,^50 Among these studies, the distance between AR-markings and Doppler markings ranged from 2 to 17.7 mm.
Three studies compared preoperative AR markings with intraoperative measurements of perforator localization in relation to the umbilicus.32^,^41^,^44 The mean error in accuracy of these studies ranged from perfect correlation to 5.3 mm error. One study compared these results to Doppler markings, and reported greater accuracy of AR compared to Doppler (5.3 mm vs. 19.7 mm).44
Three studies examined the ability of AR to detect the presence of perforators and compared this to handheld Doppler,32^,^33^,^44 demonstrating greater sensitivity for perforator localization of AR compared to handheld Doppler. In contrast, one study reported slightly less recognition rate of perforators by AR compared with color Doppler ultrasound (93.9% vs. 97.2%), although these results were non-significant.48
Eight studies evaluated the accuracy of AR-based perforator localization by using Doppler ultrasound on AR-based markings, thus in theory confirming the presence of a perforator at this marking.29^,^31^,^32^,^35^,^41^,^43^,^47^,^51 In 7 of the studies, Doppler signal was positive in 92% to 100% of the perforators. In a case series involving 5 patients, perfect match between AR markings and Doppler signal was found in 4 out of 5 cases. In the case where perfect match was not achieved, AR images based on a 16-month-old CTA were used. During this period, the patient’s weight distribution changed, resulting in a 10 mm difference between AR marking and Doppler ultrasound.43
A study evaluated the accuracy of HMD-based AR perforator localization under different lighting conditions, various visual angles, and movement-induced errors in a simulated perforator localization setting.36 No significant difference in accuracy based on the visual angle, light intensity, and no movement-induced errors was observed. When comparing localization accuracy under illuminated (specifically at low intensity) and non-illuminated conditions, a significant difference in the mean error was found (2.85 mm vs. 1.35 mm, P = 0.02).36 In addition, they found HMD-based AR to be accurate with a minimum mean error of 1.35 mm and maximum error of 3.18 mm.36
Preoperative and intraoperative use of time
Nine studies reported on the influence of AR on preoperative planning time or intraoperative time.
Six studies evaluated additional time required to integrate the AR system into their workflow.29^,^33^,^39^,^40^,^43^,^50 Time required to generate 3D images was reported to range from 1033^,^50 and 15 min39 to 60 min.43 Image registration was completed between 7 and 11 min40^,^43^,^50; however, one study reported nearly instantaneous registration, which prompted them to abandon plans to measure its duration.29
Three studies reported on the time spent on preoperative perforator localization. In an RCT, the use of AR significantly reduced the time spent on preoperative planning compared with the Doppler ultrasound (2.3 min vs. 20 min).33 Other studies reported mean times spent on perforator localization using AR from 3.5 to 7 min.43^,^51
Two studies evaluated the impact of using AR for preoperative planning on intraoperative time. Hummelink et al. demonstrated a significant reduction in flap harvest time by 12%, from 155 to 136 min, when comparing Doppler to AR.33 Similarly, Pereira et al. reported a reduction in flap harvest time by 20%, from 90 to 72 min, when using a smartphone-based AR perforator localization app.41 In contrast, Liu et al. observed no significant difference in operative time when using AR or color Doppler ultrasound for preoperative planning of ALT or free fibula flaps.48
Postoperative complications
Eight studies reported on the complications following AR-based preoperative planning.
In an RCT, Hummelink et al. found no significant difference in flap-related nor donor site-related complications between an AR and a Doppler group.33 Liu et al. observed significantly less average blood loss when using HMD-based AR for preoperative planning of ALT and free fibula flaps, compared to color Doppler ultrasound (24 mL vs. 56 mL).48 Six other studies, primarily case series, reported the rates of complications and by the nature of their studies, they precluded direct comparison with other imaging modalities.28^,^31^,^35^,^40^,^42^,^44
Surgeons’ opinions
One study assessed feasibility of AR use for surgical flaps through questionnaires, using the System Usability Scale based on a 1-5 Likert scale. They reported a mean SUS score of 67, classifying the system as “moderate to good” in a classification system proposed by the authors.50 However, experienced surgeons rated the AR system as a “nice, but not necessary tool for clinical practice”.50
Discussion
XR technologies are emerging in the medical field. With their abilities to provide new representations of CT and MR scans, they open up new possibilities in the preoperative and intraoperative phase of microsurgical free flap procedures. We performed a systematic review to examine the utilization of XR in perforator localization and its comparison with other imaging modalities in terms of workflow, user experience, and clinical outcomes.
From this review, we found that XR technologies, VR and AR, show promise in the field of plastic and reconstructive surgery. Both technologies were found to be capable of reducing the time spent on preoperative perforator mapping and total intraoperative time compared with CTA and Doppler, respectively.22^,^24^,^33^,^41 Reducing preoperative times may be beneficial for surgical departments and patients, although it could be argued that preoperative perforator marking could be done, for example, a day in advance of the surgery, thereby not influencing the surgical capacity. Reducing intraoperative times may be beneficial in a clinical setting by increasing the surgical capacity and reducing patient complication rates by reducing anesthesia time. However, “free-style” free flap techniques, in which no technologies are used preoperatively to identify perforators, are also proposed as time-reducing without increasing the complication rates.53 This could limit the necessity for developing new technologies to aid perforator localization, although it could be argued that some surgeons, especially the less experienced surgeons, may continue to benefit from technologies such as XR for these complicated procedures.
AR shows promise in improving perforator localization accuracy, demonstrating greater accuracy when compared with Doppler.32^,^33^,^44 However, CTA is considered the gold standard for perforator mapping. Therefore, future research should focus on comparing CTA with and without XR technology. Regarding perforator localization accuracy, one source of error may be the difference between the anatomy visualized through AR (based on e.g., CTA) and actual anatomy at the time of surgery. Seth et al. reported that in one case, a small weight distribution change in the abdomen led to a change in perforator localization between AR-visualized CTA-based anatomy and the intraoperative anatomy (16 months post CTA).43 However, using DIRT as an imaging modality for e.g., projector-based AR may overcome this problem by projecting real-time anatomy onto the patient, thereby possibly improving perforator localization accuracy.52
However, the results from the studies on VR perforator localization accuracy are contradictory. Therefore, more studies are needed to make any conclusions.
One study found that VR had the potential to lower complication rates when compared with Doppler,22 and another study found no difference in complication rates when using AR instead of Doppler.33 However, most studies did not include comparisons with other modalities; therefore, the impact of these technologies on complication rates is still unknown.
User experience was assessed in a VR study and another AR study. VR has been proved to provide the surgeons with more realistic anatomical information,37 and AR was scored as a moderate to good system, although experienced surgeons rated the system as “nice, but not necessary for clinical practice”,50 which could indicate that they considered conventional methods to be sufficient for preoperative planning. An interesting aspect is whether XR technologies are more beneficial for less experienced surgeons, which should be examined in future studies.
When using AR for perforator identification, surgeons can realistically assess digital representations of the anatomy and real anatomy simultaneously, which may be beneficial in preoperative planning and intraoperative navigation, as suggested in 2 studies.27^,^43 However, this is not the case when using VR for perforator identification, as the surgeon will be in a completely digital environment that is separate from the actual patient. Interestingly, no studies on perforator identification have yet compared VR to AR; hence, the benefits of bridging the gap between the digital and real world is still unknown. Additionally, the quality of the radiologic dataset used for 3D rendering may also influence the quality of the XR images, which could be a limiting factor for these technologies. Determining optimal scanning protocols to generate adequate XR images should be a focus for future research.
The literature on XR use in plastic and reconstructive microsurgery is limited by the quality assessment findings in this systematic review, indicating risk of bias and low-quality studies with low level of evidence. Therefore, high-quality, comparative, and prospective studies are needed to fully determine the clinical value of these technologies in plastic and reconstructive surgical procedures. Furthermore, the studies are limited by the lack of objective measures on different clinical outcomes. Therefore, we suggest that future studies on this topic should standardize outcome measures including preoperative time spent on perforator mapping, intraoperative times, accuracy of perforator localization measured as preoperative markings compared with intraoperative localization of the perforator, and postoperative complications.
Conclusion
Extended reality technologies, including VR and AR, show promise as tools for preoperative perforator localization in plastic and reconstructive surgery. These systems can realistically present patient-specific anatomy to the surgeon and potentially offer greater time efficiency compared to conventional imaging modalities. However, the clinical value of XR in this field remains uncertain due to the limitations in the current literature, including potential biases and low levels of evidence. Therefore, we recommend conducting further high-quality studies with standardized and objective outcome measures.
Conflicts of interest
PSK was co-author on one of the included articles in this review.
KHR, MBA, NK, and MR declare that they have no competing interests associated with the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Geddes C.R.Morris S.F.Neligan P.C.Perforator flaps: Evolution, classification, and applications Ann Plast Surg 501200390991254511610.1097/00000637-200301000-00016 · doi ↗ · pubmed ↗
- 2Ireton J.E.Lakhiani C.Saint-Cyr M.Vascular anatomy of the deep inferior epigastric artery perforator flap: a systematic review Plast Reconstr Surg 13452014810 e 821e 10.1097/PRS.000000000000062525347657 · doi ↗ · pubmed ↗
- 3Taylor G.I.Palmer J.H.The vascular territories (angiosomes) of the body: Experimental study and clinical applications Br J Plast Surg 4021987113141356744510.1016/0007-1226(87)90185-8 · doi ↗ · pubmed ↗
- 4Taylor G.I.Doyle M.Mc Carten G.The Doppler probe for planning flaps: Anatomical study and clinical applications Br J Plast Surg 4311990116217871710.1016/0007-1226(90)90039-3 · doi ↗ · pubmed ↗
- 5Blondeel P.N.Beyens G.Verhaeghe R.Doppler flowmetry in the planning of perforator flaps Br J Plast Surg 5131998202209966487910.1016/s 0007-1226(98)80010-6 · doi ↗ · pubmed ↗
- 6Masia J.Clavero J.A.Larrañaga J.R.Alomar X.Pons G.Serret P.Multidetector-row computed tomography in the planning of abdominal perforator flaps J Plast Reconstr Aesthet Surg 59620065945991671695210.1016/j.bjps.2005.10.024 · doi ↗ · pubmed ↗
- 7Alonso-Burgos A.García-Tutor E.Bastarrika G.Cano D.Martínez-Cuesta A.Pina L.J.Preoperative planning of deep inferior epigastric artery perforator flap reconstruction with multislice-CT angiography: Imaging findings and initial experience J Plast Reconstr Aesthet Surg 59620065855931671695110.1016/j.bjps.2005.12.011 · doi ↗ · pubmed ↗
- 8Rosson G.D.Williams C.G.Fishman E.K.Singh N.K.3D CT angiography of abdominal wall vascular perforators to plan DIEAP flaps Microsurgery 27820076416461794110510.1002/micr.20423 · doi ↗ · pubmed ↗