Titanium Elastic Nailing Versus Hip Spica Cast in the Treatment of Femoral Shaft Fractures in Children
Habiba Ijaz, Hussain Ali, Muhammad Mannan, Muhammad Awais Iqbal, Muhammad A Hamid

TL;DR
This study compares titanium elastic nailing and hip spica casting for treating femoral fractures in children, finding that nailing allows earlier weight bearing.
Contribution
The study provides empirical evidence on treatment efficacy for older children with femoral shaft fractures.
Findings
Titanium elastic nailing allowed earlier weight bearing compared to hip spica casting.
Hospital stay was shorter in the hip spica casting group.
Surgical infrastructure availability influences treatment suitability.
Abstract
Objective The objective of this study is to compare titanium elastic nailing (TEN) to hip spica casting (HSC) in the treatment of paediatric femoral shaft fractures, focusing on hospital stay duration and time to initiation of weight bearing. Study design This was a quasi-experimental study conducted at the Department of Orthopaedic Surgery, Benazir Bhutto Hospital, Rawalpindi, over a six-month period. Duration and place of study The data for this study were collected at the Department of Orthopaedic Surgery, Benazir Bhutto Hospital, a major tertiary care and trauma referral centre, over a six-month period from 8 August 2018 to 8 February 2019. Patients and methods A total of 60 children aged 6-12 years with femoral shaft fractures were enrolled using consecutive sampling and divided into two groups based on the treatment provided by the consultant orthopaedic surgeon. Group A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
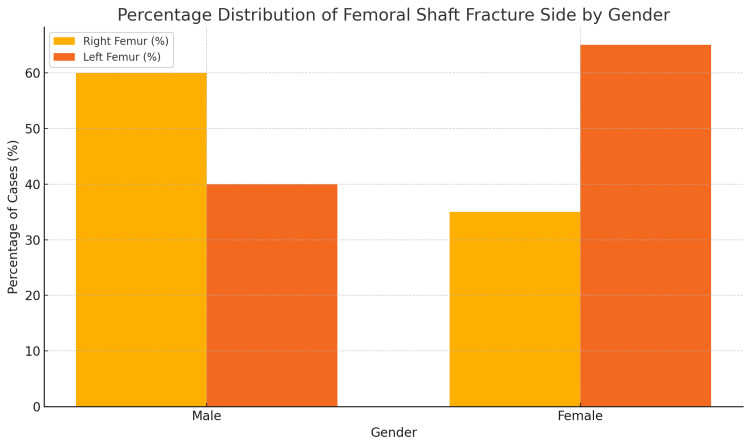 Figure 1
Figure 1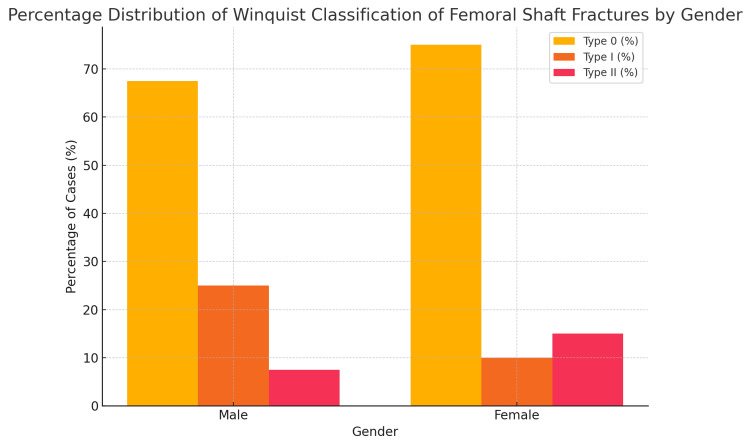 Figure 2
Figure 2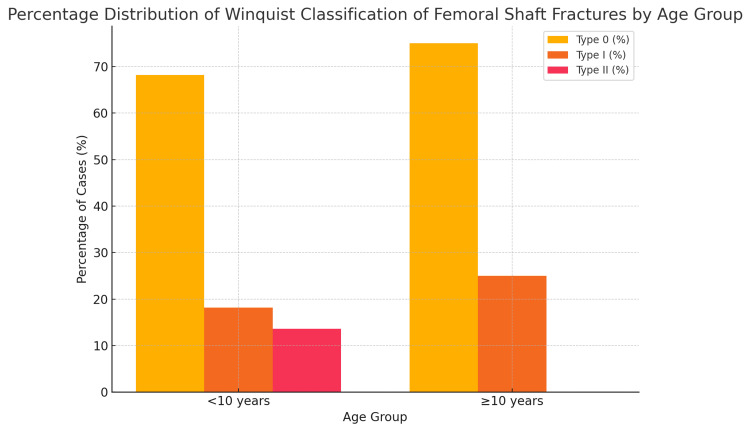 Figure 3
Figure 3| Group | Category | n (%) | Mean Age±SD (Years) |
| Group A (TEN group) | Male | 20 (66.7%) | 8.45±2.06 |
| Female | 10 (33.3%) | 8.40±1.71 | |
| Total | 30 (100%) | 8.43±1.92 | |
| Group B (hip spica group) | Male | 20 (66.7%) | 7.70±2.08 |
| Female | 10 (33.3%) | 7.70±1.34 | |
| Total | 30 (100%) | 7.70±1.84 |
| Group | Treatment Group | Time to Weight Bearing (Mean±SD, Days) | P-value |
| <10 years | Titanium elastic nailing | 28.95±6.6 | 0.032 |
| Hip spica cast | 55.29±12.1 | 0.032 | |
| ≥10 years | Titanium elastic nailing | 33.80±6.3 | 0.028 |
| Hip spica cast | 76.33±6.5 | 0.028 | |
| Male | Titanium elastic nailing | 29.40±6.6 | 0.041 |
| Hip spica cast | 60.50±14.9 | 0.041 | |
| Female | Titanium elastic nailing | 32.90±.0 | 0.039 |
| Hip spica cast | 57.50±12.6 | 0.039 | |
| Right | Titanium elastic nailing | 29.40±6.5 | 0.036 |
| Hip spica cast | 62.00±15.4 | 0.036 | |
| Left | Titanium elastic nailing | 31.73±7.1 | 0.034 |
| Hip spica cast | 56.64±12.3 | 0.034 |
| Winquist Type | Treatment Group | Duration of Hospital Stay (Mean±SD, Days) | P-value (T-test) |
| Type 0 | Titanium elastic nailing | 3.95±0.89 | 0.045 |
| Hip spica cast | 2.82±0.91 | 0.045 | |
| Type I | Titanium elastic nailing | 4.00±0.58 | 0.078 |
| Hip spica cast | 3.60±1.34 | 0.078 | |
| Type II | Titanium elastic nailing | 3.67±0.58 | 0.092 |
| Hip spica cast | 3.67±1.15 | 0.092 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone fractures and treatments · Hip and Femur Fractures · Orthopaedic implants and arthroplasty
Introduction
Children are more likely to suffer a shaft of femur fracture due to their active lifestyle, anatomical configuration and biomechanical differences from adults [1]. These injuries require hospitalisation. The healing of such injuries is very rapid due to the rich blood supply of the femoral shaft. A trend towards operative stabilisation is seen for children with femoral shaft fractures, depending on their age and the type of injury [2]. Preschool-aged children still benefit from nonsurgical treatment not just because it is cost-effective and commonly preferred but also due to their high remodelling potential, smaller size and better tolerance to immobilisation methods such as traction and spica casting. Additionally, non-operative management avoids surgical and anaesthesia-related risks in this younger age group.
In the case of a school-age child with an isolated femoral shaft fracture, surgical treatment is generally preferred due to more rapid mobilisation and the earlier resumption of daily activities. Titanium elastic nailing (TEN) has demonstrated significant benefits in children aged 6-16 years. In addition to being easy to use, it is less invasive and provides excellent functional outcomes [3,4]. Hip spica casting (HSC), however, remains a widely used treatment modality in paediatric orthopaedics, despite the growing preference for operative interventions such as TEN [5].
A study by Shemshaki et al. demonstrated that TEN results in significantly shorter hospital stays (6.9±2.9 days) and earlier mobilisation with aids (17.6±10.2 days) compared to hip spica casting (20.5±5.8 days) (p<0.001) [6]. While international studies have shown the benefits of TEN, there is comparatively limited literature on its use in the Pakistani paediatric population. However, some local studies have reported similar findings, indicating shorter recovery and earlier weight bearing with TEN compared to spica casting [7]. These findings highlight the importance of context-specific research, as ethnic, geographical and healthcare system differences may influence outcomes. Our study aimed to contribute to this limited local evidence by comparing titanium elastic nailing to hip spica casting in terms of hospital stay and time to weight bearing in children with femoral shaft fractures.
Materials and methods
A quasi-experimental prospective study targeting paediatric patients with femoral shaft fractures was conducted at the Department of Orthopaedic Surgery, Benazir Bhutto Hospital, Rawalpindi, Pakistan. The study specifically included children aged 6-12 years and was conducted following ethical approval from the Research Evaluation Unit of the College of Physicians and Surgeons Pakistan (CPSP) (approval number: CPSP/REU/OSG-2017-126-1818). The data collection period spanned from 8 August 2018 to 8 February 2019. The study aimed to compare two different treatment methods, titanium elastic nailing and hip spica casting, in terms of hospital stay and time to initiation of weight bearing.
The sample size was calculated using data from a previously published study, which reported a mean time to early weight bearing of 17.6 days in Group A and 65.6 days in Group B, with a standard deviation of 10.45. Based on these values and using a 99% power and a 5% level of significance, the required sample size was determined to be 30 patients per group. A total of 60 children, aged 6-12 years and of both genders, were enrolled using a non-probability consecutive sampling technique from the Orthopaedic Surgery Department of Benazir Bhutto Hospital, Rawalpindi. Children with open fractures, comminuted femoral shaft fractures, bleeding diathesis or pathological fractures were excluded, as these conditions required alternative management strategies.
Patients were divided into two groups based on the treatment approach decided by the consultant orthopaedic surgeon, taking into account the patient's age, fracture characteristics and overall clinical condition. Group A (titanium elastic nailing) included 30 children who underwent operative treatment with titanium elastic nails, while Group B (hip spica cast) consisted of 30 children who received early hip spica casting following initial traction. Informed written consent was obtained from the parents or guardians of all participants before their inclusion in the study.
For Group A, pre-anaesthesia workup was completed in all patients. The surgical procedure was performed under general anaesthesia by a consultant orthopaedic surgeon with over four years of experience, assisted by a trainee registrar. Titanium elastic nails were inserted retrograde through small incisions under image intensifier guidance, extending proximally to the physeal zone. Fracture reduction was confirmed by achieving proper alignment and length. Nail diameter was selected based on the width of the medullary canal at its narrowest part. Postoperative antibiotics were administered, and patients were discharged once stable. The hospital stay duration was recorded, and patients were reviewed at two weeks for wound inspection, stitch removal and postoperative X-rays. Weight bearing was typically initiated at four weeks post-surgery.
For Group B, early hip spica casts were applied following initial skin traction, typically within 72 hours of injury. The cast application was performed under monitored conditions in the operating theatre. Sedation was administered using oral midazolam (0.5 mg/kg) and syrup paracetamol (15 mg/kg) approximately 30 minutes before the procedure, under the supervision of an anaesthetist. A one-and-a-half spica cast was applied, extending from the chest to the distal tibia on the affected leg and to the distal femur on the contralateral side. Alignment was maintained using traction and fluoroscopic guidance. After the confirmation of satisfactory alignment, the patient was discharged with cast care instructions. A follow-up was conducted at two weeks to evaluate the cast condition and fracture alignment. The cast was maintained for six weeks in children under 10 years and for eight weeks in those aged 10 years or older. After cast removal, physiotherapy was initiated, and weight bearing was gradually encouraged.
Both groups were followed up at two, four, six, eight and 12 weeks post treatment. At each follow-up, assessments were performed in the outpatient clinic by a consultant orthopaedic surgeon and a trainee registrar in the presence of the child's parents. Clinical evaluation included the range of motion, pain on movement and stability at the fracture site. The timing of weight-bearing initiation was determined based on the absence of pain, the restoration of joint mobility and the treating surgeon's clinical judgement.
Data were analysed using SPSS version 22 (IBM Corp., Armonk, NY). Quantitative variables such as age, hospital stay duration and time to weight bearing were expressed as means and standard deviations. Qualitative variables such as gender and fracture side were presented as frequencies and percentages. An independent samples t-test was applied to compare mean values between the two groups. Baseline characteristics were reviewed to assess comparability, and stratification was done for variables such as age, gender, side of fracture and mode of injury. A p-value of <0.05 was considered statistically significant.
Results
The data were collected using a specially designed pro forma. In the total study population, 66.7% (n=40) of patients were men with a mean age of 8.07±2.08 years, while 33.3% (n=20) of patients were women with a mean age of 8.05±1.54 years. There were equal numbers of men (n=20) and women (n=10) in both groups, while in Group A (TEN group), the mean age was 8.43±1.92 years, and in Group B (HSC group), it was 7.70±1.84 years. A detailed demographic profile of both groups is shown in Table 1.
Out of a total of 60 children with femoral shaft fractures, 51.7% (n=31) presented with right femoral shaft fractures, and 48.3% (n=29) presented with left femoral shaft fractures. A detailed demographic profile in accordance with the side of the fractured femoral shaft is described in Figure 1.
Percentage distribution of right and left femoral shaft fractures according to gender
A total of 42 out of 60 patients (70%) presented with Winquist type 0 fracture, while Winquist type I and II fractures were present in 12 (20%) and six (10%) patients, respectively. This is presented in Figure 2.
Percentage distribution of Winquist classification types of femoral shaft fractures according to gender
Among children aged less than 10 years, Winquist type 0 fractures accounted for the majority, followed by type I and type II fractures. In children aged 10 years and older, type 0 fractures also predominated, while no cases of type II fractures were observed in this group. These findings suggest that simpler fracture patterns (type 0) were the most common in both younger and older age groups, with more complex fracture patterns (type II) occurring exclusively in children under 10 years, which is presented in Figure 3.
Percentage distribution of Winquist classification types of femoral shaft fractures according to age group
This prospective study found a statistically significant difference in both hospital stay duration and time to initiation of weight bearing between the two treatment groups. When stratified by age, gender and fracture side (Table 2), titanium elastic nailing consistently resulted in significantly earlier initiation of weight bearing compared to hip spica casting across all subgroups. In children aged less than 10 years, the mean time to weight bearing was 28.95±6.6 days in the TEN group versus 55.29±12.1 days in the HSC group (p=0.032), while in those aged 10 years or older, it was 33.80±6.3 days and 76.33±6.5 days, respectively (p=0.028). Among male patients, weight bearing was initiated at 29.40±6.6 days in the TEN group compared to 60.50±14.9 days in the HSC group (p=0.041), and among female patients, weight bearing was initiated at 32.90±7.0 days versus 57.50±12.6 days, respectively (p=0.039). Similarly, for right-sided femoral fractures, weight bearing commenced at 29.40±6.5 days in the TEN group and 62.00±15.4 days in the HSC group (p=0.036), while for left-sided fractures, it began at 31.73±7.1 days compared to 56.64±12.3 days, respectively (p=0.034). The analysis of hospital stay stratified by Winquist fracture type (Table 3) showed that in patients with type 0 fractures, the TEN group had a significantly longer hospital stay (3.95±0.89 days) compared to the HSC group (2.82±0.91 days) (p=0.045), while no statistically significant differences in hospital stay were observed in type I or type II fractures (p>0.05). These findings confirm that titanium elastic nailing consistently promoted earlier weight bearing across all age groups, genders and fracture sides, while hospital stay was slightly longer in TEN-treated simple fractures (type 0) as detailed in Table 2 and Table 3.
Discussion
The malunion or maltreatment of a femoral fracture may result in complications such as shortening, deformity, delayed healing, nonunion and infections. Traditionally, spica casting or traction, followed by casting, has been the standard treatment for paediatric diaphyseal femur fractures, as recommended by the American Academy of Orthopaedic Surgeons (AAOS), particularly for children aged six months to five years [8]. However, a shift towards operative approaches has occurred in older children, with flexible intramedullary nails such as titanium elastic nails (TEN) gaining preference due to their minimally invasive nature, biomechanical stability and effectiveness in promoting rapid healing [9,10]. Unlike more invasive techniques such as external fixation or plate fixation, TEN preserves the femoral blood supply and facilitates early mobilisation, reducing complications associated with prolonged immobilisation, such as limb length discrepancies. Additionally, early discharge associated with TEN can reduce the economic burden on families due to decreased hospital stays.
Our study aims to compare two commonly used treatment modalities, titanium elastic nailing and early hip spica casting, in terms of hospital stay and time to weight bearing in children aged 6-12 years. The findings support the hypothesis that TEN offers functional advantages over hip spica casting. Specifically, patients in the TEN group began weight bearing significantly earlier and had a slightly longer hospital stay, largely attributable to the surgical nature of the intervention. These results directly address the research objective and demonstrate clinically relevant benefits of TEN in terms of early mobilisation and return to daily activities.
Our findings are consistent with both national and international literature. Verma et al. [11] and Saseendar et al. [12] also reported shorter time to weight bearing and lower complication rates in patients treated with TEN compared to hip spica casts [13,14]. Saseendar et al. found that fracture union occurred earlier in the surgical group (six weeks) than in the spica group (eight weeks), with a p-value of 0.001. Spica castings resulted in significant coronal plane angulation (p<0.001), prolonged immobilisation (p<0.001) and later full weight bearing (p<0.001). Compared to hip spica casting, titanium elastic nailing resulted in better Flynn scores and earlier functional recovery [12].
A study conducted by Mehdinasab et al. evaluated and compared the short-term results of hip spica casts and intramedullary pin fixations in children aged 6-12 years [15]. The average treatment duration from admission to independent walking was 75.3 days for the spica cast group and 61.2 days for the TEN group (p<0.05). Hossain et al. also found that intramedullary fixation by TEN was effective in properly selected patients aged 5-15 years in Bangladesh [16]. A retrospective comparative study by Nascimento et al. reported a mean hospital stay of nine days for the TEN group and 20 days for the HSC group (p<0.005) [17]. Patients in the TEN group began weight bearing after 3.5 weeks, compared to 9.6 weeks in the HSC group. Similarly, Khan et al. demonstrated that retrograde flexible intramedullary nails were more effective than immediate hip spica casts in treating paediatric diaphyseal fractures in Pakistani patients, with earlier functional recovery and earlier weight bearing (p<0.005) [18].
The consistent advantage of TEN across various studies, including ours, highlights its effectiveness across diverse patient profiles such as age, gender, fracture side and Winquist classification. Nonetheless, we acknowledge that the non-randomised nature of our study may introduce selection bias, as treatment allocation was based on the attending surgeon's clinical judgement. Factors such as fracture stability, patient nutritional status and socioeconomic considerations may have influenced the decision to opt for TEN or spica casting, potentially impacting the comparability between groups.
No major complications such as infection, reoperation, neurovascular injury or skin-related issues associated with spica casting were observed in either group during the follow-up period of this study. Some patients did experience minor complications, including malunion and leg length discrepancy; however, these did not result in any significant functional limitations and did not necessitate additional intervention. While these findings are encouraging, the formal documentation and analysis of such complications were not part of the study protocol. Future research should include a comprehensive evaluation of both clinical and radiographic outcomes to ensure a more complete comparison of surgical to conservative management strategies in paediatric femoral shaft fractures.
It is important to note that while TEN offers the benefit of earlier functional recovery, it is not without drawbacks. TEN requires general anaesthesia, intraoperative imaging, surgical expertise and access to hospital infrastructure, factors that may not be readily available in all healthcare settings, particularly in resource-constrained environments. Moreover, TEN usually necessitates a second surgery for implant removal, which may increase costs and expose the child to additional anaesthesia-related risks. In contrast, hip spica casting remains a non-operative, low-cost alternative that avoids surgical risks and is more feasible in many low-resource settings.
These differences in invasiveness, cost, anaesthetic requirements and parental preference were not the focus of the current study but are critical factors in treatment planning and should be carefully weighed when choosing the most appropriate management strategy. Future studies should incorporate these dimensions to offer a more holistic assessment of both treatment modalities.
While our study was strengthened by prospective data collection and standardised follow-ups, limitations include a relatively small sample size, short duration of follow-up and single-centre design. Additionally, a few patients were lost to follow-up, reducing the overall cohort. Larger, multicentre randomised controlled trials are needed to validate these results and provide more robust evidence to guide treatment decisions.
Conclusions
This study observed that titanium elastic nailing was associated with the earlier initiation of weight bearing compared to hip spica casting in children aged 6-12 years with femoral shaft fractures. As hip spica casting is more commonly recommended for younger children under the age of five, our findings suggest that titanium elastic nailing may represent a more appropriate option in older paediatric patients, particularly in settings where surgical infrastructure is available. While TEN demonstrated potential advantages in facilitating earlier functional recovery, these results should be interpreted within the specific context of the study's focus on time to weight bearing and hospital stay.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Treatment of closed diaphyseal fractures of femur in children comparative study between hip spica & initial traction followed by hip spica cast Orthop Muscular Syst Memon FA Soomro H Baloch S Devrajani BR 1752016
- 2Functional outcome of treatment of paediatric diaphysial femur fractures operated using titanium elastic nailing Int J Orthop Sci Panchal D Rathod D Rao D 21622032017
- 3Treatment of closed femoral shaft fractures in children aged 2-10 years: a systematic review and meta-analysis Eur J Trauma Emerg Surg van Cruchten S Warmerdam EC Kempink DR de Ridder VA 340934274820223433881910.1007/s 00068-021-01752-7PMC 9532337 · doi ↗ · pubmed ↗
- 4Results of titanium elastic nailing in paediatric femoral diaphyseal fractures— report of 30 cases Chinese J Traumatol Jalan D Chandra R Sharma V 778316201323540894 · pubmed ↗
- 5Systematic review of spica casting for the treatment of paediatric diaphyseal femur fractures J Child Orthop Tisherman RT Hoellwarth JS Mendelson SA 13614412201810.1302/1863-2548.12.170201 PMC 590274729707052 · doi ↗ · pubmed ↗
- 6Titanium elastic nailing versus hip spica cast in treatment of femoral-shaft fractures in children J Orthop Traumatol Shemshaki HR Mousavi H Salehi G Eshaghi MA 45481220112134054410.1007/s 10195-011-0128-0PMC 3052430 · doi ↗ · pubmed ↗
- 7Comparison of titanium elastic nailing vs hip spica cast in treatment of femoral shaft fractures in children between 6-12 years of age Pak J Med Health Sci Ahmad I Gilani HR Rasool K Rasool A 71771992015 https://pjmhsonline.com/2015/apr_june/pdf/717%20%20%20Comparison%20of%20Titanium%20Elastic%20Nailing%20vs%20Hip%20Spica%20Cast%20in%20Treatment%20of%20Femoral%20Shaft%20Fractures%20in%20Children%20between%206-12.pdf
- 8Incidence of secondary interventions after early spica casting for diaphyseal femur fractures in young children Can J Surg TrottierÉR Hatcher L Feng J Camp M Bouchard M 02465202210.1503/cjs.006521 PMC 933786635790240 · doi ↗ · pubmed ↗