Multiple Mucous Cysts on the Hands of a Patient With Systemic Sclerosis Treated With Collagen Sheets for Scar Healing
Takano Hobo, Hiroshi Kato, Shinji Kano, Yukiko Yasui, Maki Yoshimitsu, Motoki Nakamura, Akimichi Morita

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
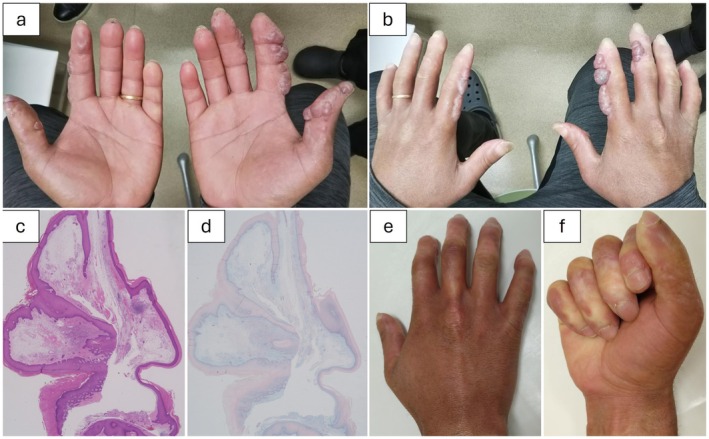 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatologic Treatments and Research · Cancer and Skin Lesions · Skin Diseases and Diabetes
Dear Editor,
A 20‐year‐old man was referred to our clinic after developing multiple blisters on his fingers 2 years ago. He was diagnosed with systemic sclerosis 7 years ago and treated by a local physician. At his initial visit, he presented with multiple tense blisters measuring 1–2 cm in diameter on his fingers, accompanied by sclerosis (Figure 1a,b). Laboratory tests revealed positive anti‐Scl‐70 antibodies, while pemphigoid antibodies were negative.
(a) Clinical photograph of the palm displaying blisters. (b) Clinical photograph showing multiple blisters on the dorsal side of the right first, second, and third fingers, as well as the left first and second fingers. (c) Hematoxylin and eosin (HE) staining of the excised specimen, revealing areas lacking defined structure and exhibiting edema in the interstitial tissue of the subcutaneous layer. (×20) (d) Immunostaining of the excised specimen with Alcian blue (pH 2.5), demonstrating positive staining in the interstitial tissue. (×20) (e) Clinical photograph of the dorsal hand 1 year postoperatively, demonstrating no recurrence of lesions. (f) Clinical photograph of the palm 1 year postoperatively, showing no contracture and preserved grasping function.
For diagnosis, a blister was completely excised under local anesthesia, which contained a viscous fluid. Histopathological examination revealed a cystic lesion with an indistinct wall structure, and Alcian blue staining demonstrated mucin deposition in the interstitial tissue, confirming mucinous cysts (Figure 1c,d). Following excisional biopsy, a collagen sheet was applied to promote scar healing. As no recurrence was observed at the biopsy site, all other lesions were excised and allowed to heal with collagen sheets. No recurrence was observed in the past year (Figure 1e,f).
Mucous cysts are generally classified into two types: the ganglion type, which arises from the distal interphalangeal joint, and the myxomatous type, which results from skin degeneration. The myxomatous type is caused by excessive hyaluronic acid production due to dermal fibroblast transformation into myxoma cells following mechanical stimulation. In systemic sclerosis, mucin deposition occurs due to excessive extracellular matrix protein production by activated fibroblasts, resulting in mucinous edema [1]. Similar to previous case reports [2], the lesions in this case were primarily concentrated in easily irritated areas rather than regions with severe skin sclerosis. This suggests that the cysts were caused by irritation combined with the existing scleroderma‐type skin sclerosis.
In this case, mucin deposition in sclerotic skin associated with systemic sclerosis likely contributed to the formation of mucinous cysts with a distinctive appearance. Mucin deposition in scleroderma is driven by fibroblast stimulation via inflammatory cytokines, including IL‐1 and IL‐6 [1]. As the lesions were localized to the fingers and the patient worked as a welder, mechanical stimulation may have triggered IL‐1 and IL‐6 production. Oxidative stress plays a key role in scleroderma, and low oxygen levels promote fibrogenic activities, including fibroblast proliferation and collagen production [3]. Recent studies have suggested that hypoxia contributes to dermal mucin deposition by increasing fibroblast biosynthetic activity and hyaluronic acid production [4].
The patient had undergone multiple aspiration procedures before visiting our clinic; however, the cysts recurred rapidly. Given the large number of lesions, we opted for excision therapy. The excision of small mucous cysts is followed by suturing or skin flap reconstruction. However, due to the extent of the lesions, direct suturing or flap reconstruction was challenging, and scar healing with collagen sheets was chosen instead. Collagen sheets increase HGF production by fibroblasts and consequently reduce TGFβ, which is believed to mitigate scleroderma‐like skin changes and prevent recurrence [5].
A previous case reported that excision followed by full‐thickness skin grafting resulted in recurrence several months later [2]. Our patient has remained free of recurrence for 1 year postoperatively, suggesting that using collagen sheets for scar healing helps prevent cyst recurrence.
Ethics Statement
We obtained written informed consent from the patient to publish his clinical details.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1F. Rongioletti , C. Gambini , C. Micalizzi , A. Pastorino , and A. Rebora , “Mucin Deposits in Morphea and Systemic Scleroderma,” Dermatology 189 (1994): 157–158.8075444 10.1159/000246821 · doi ↗ · pubmed ↗
- 2A. V. Marzano , E. Berti , G. Gasparini , A. Vespasiani , R. Scorza , and R. Caputo , “Unique Digital Skin Lesions Associated With Systemic Sclerosis,” British Journal of Dermatology 136 (1997): 598–600.9155967 · pubmed ↗
- 3V. Falanga , T. A. Martin , H. Takagi , et al., “Low Oxygen Tension Increases m RNA Levels of Alpha 1 (I) Procollagen in Human Dermal Fibroblasts,” Journal of Cellular Physiology 157 (1993): 408–412.8227170 10.1002/jcp.1041570225 · doi ↗ · pubmed ↗
- 4R. Pugashetti , D. C. Zedek , E. V. Seiverling , P. Rajendran , and T. Berger , “Dermal Mucinosis as a Sign of Venous Insufficiency,” Journal of Cutaneous Pathology 37 (2010): 292–296.19614999 10.1111/j.1600-0560.2009.01306.x · doi ↗ · pubmed ↗
- 5I. Rodriguez , T. Conti , and N. Bionda , “A Preliminary Direct Comparison of the Inflammatory Reduction and Growth Factor Production Capabilities of Three Commercially Available Wound Products: Collagen Sheet, Manuka Honey Sheet, and a Novel Bioengineered Collagen Derivative + Manuka Honey + Hydroxyapatite Sheet,” International Journal of Molecular Sciences 23 (2022): 10670.36142583 10.3390/ijms 231810670 PMC 9503338 · doi ↗ · pubmed ↗