BCR::ABL1‐Positive Acute Myeloid Leukemia
Alban Canali, Jean‐Baptiste Rieu, Leopoldine Lapierre, Barbara J. Bain

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
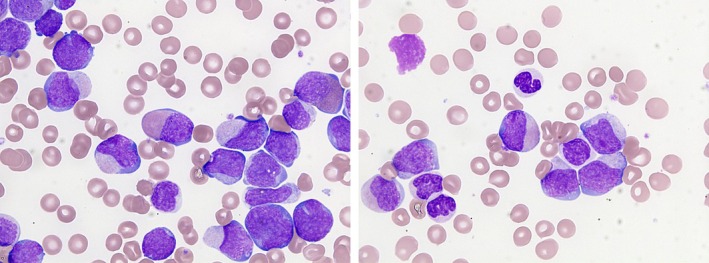 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Myeloid Leukemia Treatments · Acute Myeloid Leukemia Research · Protein Degradation and Inhibitors
1
Morphology Update has recently discussed a patient with chronic myeloid leukemia (CML) presenting in blast crisis [1]. For comparison, we present here a patient with BCR::ABL1‐positive acute myeloid leukemia (AML). The patient was a 48‐year‐old man with no known history of CML, presenting with hepatomegaly and neurological abnormalities (headaches, agitation, and behavioral disturbance). His blood count showed hemoglobin concentration 64 g/L, white cell count 457.6 × 10^9^/L, and platelet count 31 × 10^9^/L. His blood film (images × 100 objective) showed 95% blast cells; these were large, with an intermediate nuclear‐cytoplasmic ratio, irregular nuclei, sometimes nucleoli, and cytoplasm containing atypical pink to lilac granules and occasional inclusions. Promyelocytes were present but myelocytes, eosinophils, and basophils were infrequent. Neutrophils were dysplastic with hypogranular cytoplasm and abnormal nuclear forms (right image). A bone marrow aspirate was hypercellular with 84% blast cells, without prominence of eosinophils or basophils. Cytogenetic analysis showed 46,XY,t(9;22)(q34;q11)[21]. A BCR::ABL1 transcript, identified as BCR_E13::ABL1_E2, b2a2, p210, was detected on molecular analysis, together with mutations of SMC3 and WT1. In view of the molecular findings and the lack of prominent basophilia, a diagnosis of BCR::ABL1‐positive AML appeared most likely but post‐treatment follow‐up was needed for confirmation.
The patient was treated with cytarabine, idarubicin, and imatinib as induction treatment (preceded by cytoreduction with hydroxycarbamide), followed by cytarabine and imatinib for consolidation. Additionally, cytarabine, methotrexate, and methylprednisolone were administered intrathecally to treat demonstrated central nervous system infiltration. Complete remission was achieved with the marrow being morphologically normal without neutrophilic, eosinophilic or basophilic hyperplasia. Cytogenetic analysis was normal at 2 months from diagnosis and a deep molecular remission was demonstrated at 4 months.
Diagnosis of BCR::ABL1‐positive AML requires the features of AML and demonstration of BCR::ABL1. However an essential diagnostic criterion is that there should be “a lack of features of CML before or at diagnosis and after therapy” [2]. The diagnosis is thus provisional until post‐treatment follow‐up excludes an alternative diagnosis of blastic presentation of CML. De novo AML cases have less frequent splenomegaly, a higher blast percentage and lower basophil numbers [2]. The precise BCR::ABL1 transcript that is detected is not helpful because p210 is most often observed in both CML and BCR::ABL1‐positive AML [2].
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1B. Hazarika and B. J. Bain , “Presentation of Chronic Myeloid Leukemia in Basophilic Blast Crisis,” American Journal of Hematology 100, no. 1 (2025): 131–132.39177203 10.1002/ajh.27464 PMC 11625970 · doi ↗ · pubmed ↗
- 2S. Hu , T. Haferlach , K. C. Hodge , et al., “Acute Myeloid Leukaemia With BCR::ABL 1 Fusion,” 2024. In WHO Classification of Tumours Editorial Board, eds. Haematolymphoid Tumours. IARC: 125–126.