Retrospective epidemiological analysis of pulmonary tuberculosis in the older adult and characterization of rifampicin resistance-associated rpoB mutations in Nantong City, China (2014–2023)
Huiming Zhu, Shouwei Wang, Xiaofang Zhao, Peipei Wu, Ji Chen, Feng Li

TL;DR
This study examines the decline in older adult pulmonary tuberculosis cases and analyzes rifampicin resistance mutations in Nantong, China, from 2014 to 2023.
Contribution
The study provides new insights into the epidemiological trends and rpoB mutation patterns in older adults with rifampicin-resistant tuberculosis in Nantong.
Findings
The standardized incidence of older adult pulmonary tuberculosis in Nantong declined rapidly and stabilized from 2014 to 2023.
Single-gene rpoB mutations were the most common in rifampicin-resistant older adult patients.
Treatment outcomes were significantly associated with rifampicin resistance and initial diagnostic test results.
Abstract
To analyze the prevalence trend of older adult pulmonary tuberculosis (ETB) and the distribution and outcome of rifampicin-resistant rpoB gene mutation in ETB patients in Nantong. The pulmonary tuberculosis patients’ data in Nantong from 2014 to 2023 were from Tuberculosis Information Management Syste and ETB and rifampicin-resistant rpoB mutation patients were retrospectively analyzed. From 2014 to 2023, the overall standardized incidence of ETB in Nantong showed a trend of rapid decline and tended to a stable trend stabilized. A total of 140 older adult patients with rifampin resistance, aged 60–69 years, 87 cases (62.1%). single-gene mutation Probe E mutations were the most frequent, observed in 39 cases (60.0%). Specifically, 52 cases (80.00%) were resistant to rifampicin, and Probe E of 31 cases (59.62%) showed the most mutations. The outcome of ETB patients with rifampicin…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
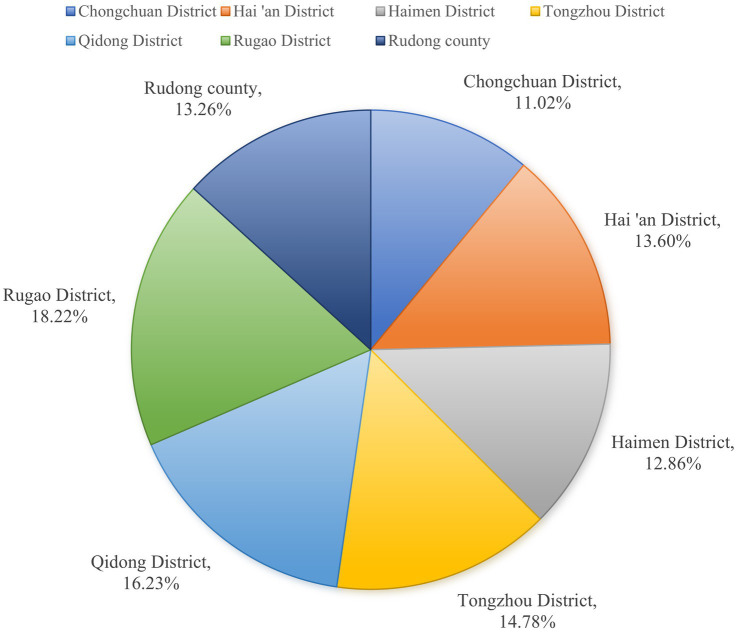 Figure 1
Figure 1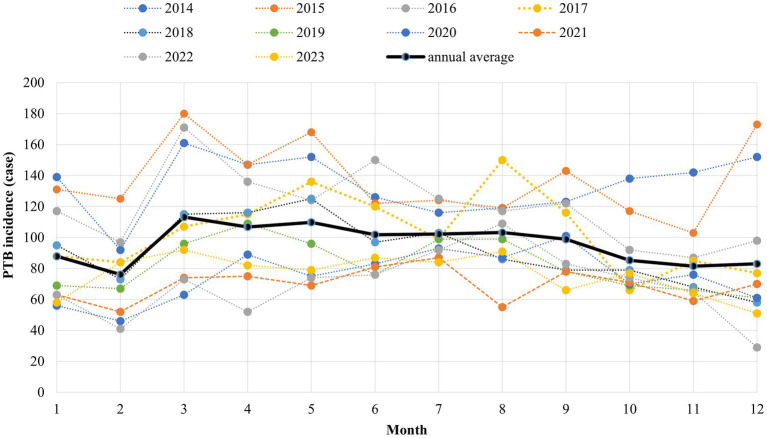 Figure 2
Figure 2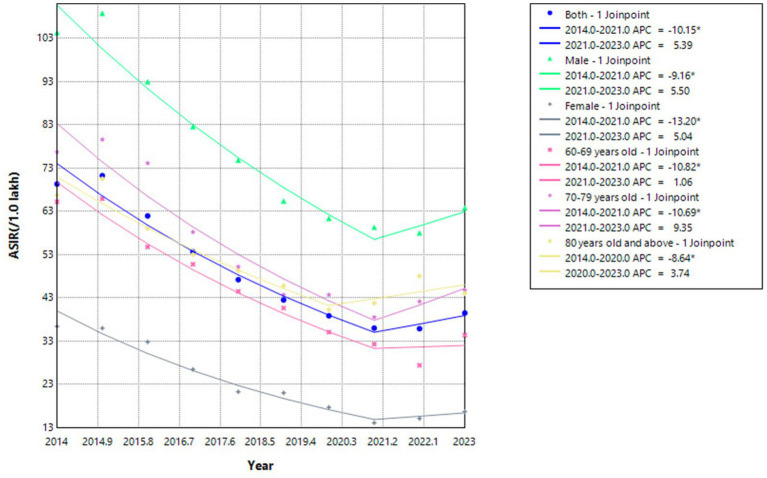 Figure 3
Figure 3| Year | Total | Gender | Age | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 60–69 | 70–79 | ≥80 | ||||||||
| NC | ASIR (/lakh) | NC | ASIR (/lakh) | NC | ASIR (/lakh) | NC | ASIR (/lakh) | NC | ASIR (/lakh) | NC | ASIR (/lakh) | |
| 2014 | 1,607 | 69.31 | 1,172 | 104.39 | 435 | 36.37 | 748 | 65.20 | 592 | 76.73 | 267 | 66.75 |
| 2015 | 1,652 | 71.25 | 1,222 | 108.84 | 430 | 35.95 | 756 | 65.90 | 614 | 79.59 | 282 | 70.50 |
| 2016 | 1,436 | 61.93 | 1,044 | 92.99 | 392 | 32.78 | 628 | 54.74 | 572 | 74.14 | 236 | 59.00 |
| 2017 | 1,243 | 53.61 | 927 | 82.57 | 316 | 26.42 | 582 | 50.73 | 449 | 58.20 | 212 | 53.00 |
| 2018 | 1,094 | 47.18 | 840 | 74.82 | 254 | 21.24 | 510 | 44.46 | 387 | 50.16 | 197 | 49.25 |
| 2019 | 985 | 42.48 | 734 | 65.38 | 251 | 20.99 | 466 | 40.62 | 337 | 43.68 | 183 | 45.75 |
| 2020 | 900 | 38.81 | 689 | 61.37 | 211 | 17.64 | 402 | 35.04 | 337 | 43.68 | 161 | 40.25 |
| 2021 | 834 | 35.97 | 666 | 59.32 | 168 | 14.05 | 370 | 32.25 | 297 | 38.50 | 167 | 41.75 |
| 2022 | 831 | 35.84 | 651 | 57.99 | 180 | 15.05 | 314 | 27.37 | 325 | 42.13 | 192 | 48.00 |
| 2023 | 915 | 39.46 | 716 | 63.77 | 199 | 16.64 | 394 | 34.34 | 345 | 44.72 | 176 | 44.00 |
| Characteristic | Year | APC (95%CI) | AAPC (95%CI) | ||||
|---|---|---|---|---|---|---|---|
| Total | 2014–2021 | −10.15* (−12.19, − 8.06) | 8.06 | <0.001 | −6.91* (−9.85, −3.87) | −4.37 | <0.001 |
| 2021–2023 | 5.39 (−11.24, 25.14) | 0.79 | 0.47 | ||||
| Gender | |||||||
| Male | 2014–2021 | −9.16* (−11.26, −7.02) | −10.58 | <0.001 | −6.09* (−9.11, −2.97) | −3.77 | <0.001 |
| 2021–2023 | 5.50 (−11.41, 25.65) | 0.79 | 0.47 | ||||
| Female | 2014–2021 | −13.20* (−16.04, −10.27) | −10.95 | <0.001 | −9.44* (−13.56, −5.13) | −4.18 | <0.001 |
| 2021–2023 | 5.04 (−18.09, 34.70) | 0.51 | 0.63 | ||||
| Age | |||||||
| 60–69 | 2014–2021 | −10.82* (−12.59, −9.01) | −14.66 | <0.001 | −8.31* (−10.85, −5.69) | −6.05 | <0.001 |
| 2021–2023 | 1.06 (−13.04, 17.43) | 0.18 | 0.86 | ||||
| 70–79 | 2014–2021 | −10.69* (−14.18, −7.05) | −7.29 | <0.001 | −6.58* (−11.65, −1.21) | −2.39 | 0.017 |
| 2021–2023 | 9.35 (−18.85, −47.36) | 47.36 | 0.77 | ||||
| ≥80 | 2014–2020 | −8.64* (−12.11, −5.04) | −6.01 | 0.002 | −4.69* (−7.98, −1.28) | −2.68 | 0.007 |
| 2020–2023 | 3.74 (−7.48, 16.32) | 0.82 | 0.45 | ||||
| Classification | Drug-resistance | Non-drug resistance | t/x2 | |
|---|---|---|---|---|
| Age | 22.471 | <0.001 | ||
| 60–69 | 87 (62.10) | 1821 (43.70) | ||
| 70–79 | 44 (31.40) | 1,585 (38.10) | ||
| ≥80 | 9 (6.40) | 758 (18.20) | ||
| Gender | 3.647 | 0.060 | ||
| Male | 105 (75.00) | 3,399 (81.60) | ||
| emale | 35 (25.00) | 765 (18.40) | ||
| Classification | 16.090 | 0.003 | ||
| Worker | 4 (2.86) | 30 (0.72) | ||
| Unemployed | 4 (2.86) | 41 (0.98) | ||
| Retirement | 14 (10.00) | 567 (13.62) | ||
| Farmer | 116 (82.86) | 3,506 (84.20) | ||
| Other | 2 (1.42) | 20 (0.48) | ||
| Diabetes | 4.104 | 0.128 | ||
| Yes | 3 (2.30) | 85 (2.00) | ||
| No | 94 (73.40) | 3,354 (80.50) | ||
| Uncertainty | 31 (4.10) | 725 (17.40) | ||
| Census register | 4.496 | 0.034 | ||
| Local population | 130 (92.90) | 4,024 (96.60) | ||
| Floating population | 10 (7.10) | 140 (3.40) | ||
| Patient source | 19.418 | <0.001 | ||
| Direct visit | 29 (20.70) | 933 (22.40) | ||
| Transfer treatment | 62 (44.30) | 1892 (45.40) | ||
| Trace | 44 (31.40) | 1,316 (31.60) | ||
| Referrals | 2 (1.40) | 8 (0.20) | ||
| Physical examination | 3 (2.10) | 15 (0.40) | ||
| Treatment classification | 103.595 | <0.001 | ||
| Initial treatment | 60 (42.90) | 3,422 (82.20) | ||
| Retreatment case | 80 (57.10) | 742 (17.80) | ||
| Using FDC | 0.636 | 0.425 | ||
| Yes | 58 (41.40) | 1867 (44.80) | ||
| No | 82 (58.60) | 2,297 (55.20) |
| Classification of patients | Type of probe | ||||||
|---|---|---|---|---|---|---|---|
| ProbeA | ProbeB | ProbeC | ProbeD | ProbeE | ProbeA+B | ProbeA+E | |
| Older adult ( | 6 (9.23) | 5 (7.69) | 0 | 14 (21.54) | 39 (60.00) | 1 (1.54) | 0 |
| Non-older adult ( | 5 (4.95) | 2 (1.98) | 2 (1.98) | 14 (13.86) | 76 (75.25) | 1 (0.99) | 1 (0.99) |
| 0.242 | 1.937 | 3.250 | 4.320 | ||||
|
| 0.623b | 0.164b | 0.521a | 0.071 | 0.038 | 1.000a | 1.000a |
| Classification of patients | Type of probe | ||||||
|---|---|---|---|---|---|---|---|
| ProbeA | ProbeB | ProbeC | ProbeD | ProbeE | ProbeA+B | ProbeA+E | |
| Initial treatment | 2 (7.14) | 2 (7.14) | 0 | 8 (28.57) | 12 (42.86) | 0 | 0 |
| Retreatment | 4 (10.81) | 3 (8.11) | 0 | 6 (16.22) | 27 (72.97) | 1 (2.70) | 0 |
| 0.005 | 0.000 | 1.440 | 6.023 | ||||
|
| 0.942b | 1.000b | – | 0.230 | 0.014 | 1.000a | – |
| Classification of patients | Type of probe | ||||||
|---|---|---|---|---|---|---|---|
| ProbeA | ProbeB | ProbeC | ProbeD | ProbeE | ProbeA+B | ProbeA+E | |
| Rifampin-resistance | 5 (9.62) | 4 (7.69) | 0 | 11 (21.15) | 31 (59.62) | 1 (1.92) | 0 |
| Multi drug resistance ( | 1 (7.69) | 1 (7.69) | 0 | 3 (23.08) | 8 (61.54) | 0 | 0 |
| 0.000 | 0.000 | 0.000 | 0.016 | ||||
|
| 1.000b | 1.000b | – | 1.000b | 0.899 | 1.000a | – |
| Classification of patients | Successful treatment | Unsuccessful treatment | t/x2 | |
|---|---|---|---|---|
| Age | 70.39 ± 7.25 | 68.94 ± 6.41 | 1.080 | 0.282 |
| Gender | 0.080 | 0.930 | ||
| Male | 23 (74.20) | 63 (75.00) | ||
| Female | 8 (25.80) | 21 (25.00) | ||
| Classification | 4.153 | 0.245 | ||
| Worker | 0 (0) | 2 (2.40) | ||
| Unemployed | 0 (0) | 2 (2.40) | ||
| Retirement | 1 (3.20) | 11 (13.10) | ||
| Farmer | 30 (96.80) | 69 (82.10) | ||
| Census register | 1.707 | 0.191 | ||
| Local population | 28 (90.30) | 81 (96.40) | ||
| Floating population | 3 (9.70) | 3 (3.60) | ||
| Patient source | 0.962 | 0.916 | ||
| Direct visit | 7 (22.60) | 17 (20.20) | ||
| Transfer treatment | 13 (41.90) | 38 (45.20) | ||
| Trace | 10 (32.30) | 25 (29.80) | ||
| Referrals | 0 (0) | 2 (2.40) | ||
| Physical examination | 1 (3.2) | 2 (2.40) | ||
| Treatment classification | 10.749 | 0.001 | ||
| Initial treatment | 5 (16.10) | 42 (50.00) | ||
| Retreatment case | 26 (83.90) | 42 (50.00) | ||
| Rifampin alone | 5.898 | 0.015 | ||
| Yes | 25 (80.60) | 47 (56.00) | ||
| No | 6 (19.40) | 37 (44.00) | ||
| Xpert MTB first test | 4.968 | 0.026 | ||
| Yes | 9 (29.00) | 44 (52.40) | ||
| No | 22 (71.00) | 40 (47.60) | ||
| 0-month sequential sputum | 8.550 | 0.003 | ||
| Positive | 30 (96.80) | 60 (71.40) | ||
| Negative | 1 (3.20) | 24 (28.60) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Mycobacterium research and diagnosis · Diagnosis and treatment of tuberculosis
Introduction
Tuberculosis (TB), which is one of the top ten causes of death in the world, has caused a major public health problem, with its morbidity and mortality showing a significant upward trend (1). TB is a chronic infectious disease (class B infectious disease) caused by Mycobacterium tuberculosis (MTB) complex group infection of the body. MTB can infect various organs of the body, the most common of which is to invade the lung, which is called pulmonary tuberculosis (PTB) (2–4). The important source of tuberculosis infection is bacterial-positive patients (bacterial-discharging patients), and the body may not become sick after being infected by the tuberculosis bacteria. However, the incidence will be greatly increased when the immunity is reduced.
Drug-resistant tuberculosis poses a serious threat to human health and has become a difficult and key issue in TB control (5). According to the World Health Organization’s Global Tuberculosis Report 2020, there were an estimated 10 million new cases of tuberculosis worldwide in 2019, and about 3.3% (465,000 cases) of newly treated patients and 18% of retreated patients were resistant to rifampicin, of which about 78% (363,000 cases) were multidrug-resistant tuberculosis (MDR-TB) patients (6).
According to relevant studies at home and abroad, the mutation of the rifampin resistance determining region (RRDR) in the rpoB gene of MTB is closely related to 95% of rifampicin-resistant cases (7–9). Rifampicin cannot be firmly bound to the β subunit of DNA-dependent RNA polymerase, and cannot inhibit the synthesis of mycobacterium tuberculosis RNA, so it loses its bactericidal effect (10, 11).
Studies have shown that older adult patients with tuberculosis are characterized by low immune function, irregular medication and delayed medical treatment, etc., and have become a population with a high incidence of tuberculosis (12, 13), which has brought severe tests to the prevention and control of tuberculosis (14). At present, there is a lack of research on the distribution and outcome of rpoB mutations in older adult rifampicin-resistant patients in Nantong City. In this study, we aimed to provide a basis for the prevention and treatment of older adult pulmonary tuberculosis (ETB) and rifampicin-resistant patients in Nantong city by analyzing the prevalence trend of tuberculosis in the older adult aged 60 years and above, and the distribution characteristics and outcome of rifampicin-resistant rpoB gene mutations.
Materials and methods
Data source
The research content of older adult patients with rifampicin resistance in this study has been approved by the Medical Ethics Committee of the Sixth People’s Hospital of Nantong (approval No.: NTLYLL2024019). Written informed consent for the use of samples was obtained from all participants. The data were from Tuberculosis Information Management System, the subsystem of the China Information System for Disease Control and Prevention, which collects the registration of tuberculosis patients in Nantong from 2014 to 2023, focusing on screening the case information of ETB patients aged 60 and above, and the older adult population data come from the official website of the Nantong Municipal Bureau of Statistics. From 2019 to 2023, the distribution of rifampicin-resistant rpoB gene mutations in patients with rifampicin resistance was sourced from Nantong Tuberculosis Designated Treatment Hospital.
Related definitions
The patients with tuberculosis refer to the suspected tuberculosis patients reported and registered by each county and district. The symptoms, imaging characteristics and epidemiological history of the patients are judged by the experienced specialists in the designated tuberculosis hospitals. Only when the laboratory results are highly consistent with the clinical diagnosis, the patients who are finally confirmed to be effective and entered into the system.
Tuberculosis pathogen positive refers to tuberculosis patients found by tuberculosis smear, culture and molecular biology methods. The source of patients refers to the way of tracing the patient ‘s treatment through direct treatment, referral, tracking, physical examination and promotion. The definition of tuberculosis resistance and rifampicin resistance refers to the “Guidelines for the Management of Drug-resistant Tuberculosis Planning “issued by the World Health Organization (WHO) (15).
In this study, probe A-E corresponded to a specific codon region in the rpoB gene, in which probe E targeted the 531st codon (ATC) in the 81 bp core region of the rpoB gene, which is a key mutation site related to rifampicin resistance. By specifically binding to this region, it is used to detect the base variation of rpoB gene at this site. Joinpoint regression is a statistical method commonly used in time series data analysis. It is mainly used to identify the time point (i.e., turning point) where the data trend changes, and to quantitatively analyze the trend of different stages. In terms of model selection, we use Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) to determine the optimal number and location of Joinpoints to ensure the goodness of fit of the model. By calculating indicators such as Annual Percentage Change (APC) and Average Annual Percentage Change (AAPC), the trend changes at different stages are quantitatively analyzed, which provides objective indicators for trend comparison and evaluation.
Instruments and reagents
Real-time fluorescence PCR detector (Xpert MTB/RIF, Cepheid, United States) and supporting reagents, mycobacterial antimicrobial susceptibility Roche culture tubes are provided by Zhuhai Besso Biotechnology Co., Ltd. Results determination and interpretation were as follows:
Xpert MTB check: The sputum or lavage samples were transferred to the sample management tube, and 4%NaOH of 1–2 times the volume was added. The samples were shaken for 1 min, then fully liquefied and left for 15 min at room temperature. 2 mL of liquid was absorbed and added to the reaction box for ultrasound, lysis, fluorescence amplification, polymerase chain and DNA reflection. The device automatically interprets the results of the TB test, whether it is resistant to rifampicin, and the mutation of the rifampicin-resistant rpoB gene. In this study, the Xpert MTB / RIF detection system was used to detect the rpoB gene mutation, and the interpretation criteria of the “Guidelines for the Management of Drug-resistant Tuberculosis Planning “issued by the World Health Organization (WHO) were strictly followed. The specific decision rule is: when the detection cycle threshold (Ct value) ≤ 38 and the rpoB gene detection result is positive, combined with the fluorescence signal intensity of the 531 codon region where the probe E is located, if the signal is abnormal, it indicates that there is a mutation at this site; at the same time, all positive results were reviewed twice, and the mutation sites were verified by pyrosequencing technology to ensure the accuracy of the test results.
Roche ratio method: The fresh colonies were selected by inoculation, ground in the fungus mill bottle, and compared with the Machelloway turbidimetric tube to produce 1 mg /mL bacterial suspension, then diluted 100 times to obtain 10–2 mg /mL bacterial solution, and then diluted to 10–4 mg /mL to obtain two concentrations of working bacterial solution. The two bacterial liquids were inoculated on the incline of the drug-containing medium, and the drug-sensitive results were observed after incubation at 37°C for 1 month: if the drug resistance detection result exceeded 1%, it was drug-resistant; if the number of colonies in the high-dilution blank control medium was less than 20, the test should be repeated.
Observation indicators
The results of the seventh census of Nantong City in 2020 were used as the standard population, the standardized incidence of tuberculosis in the older adult aged 60 years and above was analyzed, and the trend of gender composition and age segment of the older adult in each year was analyzed and observed. Meanwhile, rifampicin resistance and rpoB gene mutation of rifampicin resistance in the older adult were analyzed.
Statistical analysis
Excel 2017 and SPSS27.0 software were used for data processing and data analysis. Joinpiont 5.0.1 software was used to analyze the trend of registration rate of older adult patients with time, and the annual percentage change (APC) and average annual percentage change (AAPC) were calculated. The normally distributed continuous data were used ^−^x ± s, and the t-test was used between the two groups, and p < 0.05 was considered statistically significant.
Results
Basic situation of incidence registration and standardized incidence of ETB patients
From 2014 to 2023, a total of 11,498 patients aged 60 and above with PTB were registered in Nantong City, and the number of reported cases decreased from 1,607 in 2014 to 915 cases in 2023, the highest in 2015 (1,652 cases) and the lowest in 2022 (831 cases). The standardized incidence showed a trend of decreasing first and then stabilizing, with the highest standardized incidence rate in 2015(71.25/100,000) and the lowest in 2022 (35.84/100,000) (Table 1).
Trend of reported standardized incidence in ETB patients
The results of Joinpoint regression model analysis showed that the average annual standardized incidence of ETB in Nantong decreased by 6.91% (95%CI, −9.85 ~ −3.87; t = −4.37, p < 0.001), and presented different trends in the two periods. From 2014 to 2021, this segmentation showed it decreased by 10.15%, a significant decline, while from 2021 to 2023, it showed an increase by 5.39%, tending to be stable.
The average annual decline in male patients was 6.09% (95%CI: −9.11 ~ −2.97; t = −3.77, p < 0.001), Among them, the sub-segment showed a significant decline of 9.16%from 2014 to 2021, and while increased by5.50% from 2021 to 2023, tending to be stable. The average annual decrease in female patients was 9.44% (95%CI: −13.56 ~ −5.13; t = −4.18, p < 0.001), the segmentation showed also a significant decline by 15.59% from 2014 to 2021, and while increased by 5.04% from 2021 to 2023, tending to be stable.
Patients aged 60–69 years decreased by an average of 8.31%per year (95%CI: −10.85 ~ −5.69; t = −6.05, p < 0.001). Among them, the sub-segment showed a significant decline of 10.82% from 2014 to 2021, with a significant decline, and increased by 1.06% from 2021 to 2023, which tends to be stable. Patients aged 70–79 years decreased by an average of 6.58% per year (95%CI: −11.65 ~ −1.21; t = −2.39, p = 0.017). the segmentation showed that it decreased by 10.69% from 2014 to 2021, with a significant decline, with a significant decline, and increased by 9.35% from 2021 to 2023, tending to be stable. Patients aged 80 years and older decreased by an average of 4.69% per year (95%CI: −7.98 ~ −1.28; t = −2.68, p = 0.007), the segmentation shows that it decreased by 8.64%from 2014 to 2021, with a significant decline, and increased by 3.74% from 2021 to 2023, tending to be stable (Table 2; Figure 1).
Trend chart of reported incidence rate of ETB patients in Nantong City.
Distribution of ETB patients
From 2014 to 2023, the ETB patients in Nantong were mainly gathered in Rugao, Qidong and Tongzhou county, accounting for 18.22, 16.23 and 14.78%, respectively. The peak incidence of patients was mainly concentrated from March to September every year, and the incidence trough appeared in February (Figures 2, 3).
Monthly distribution of ETB patients in Nantong City (2014–2023).
Proportion of ETB patients in each county and district of Nantong City (2014–2023).
Comparison of the characteristics of ETB patients resistant to rifampicin and non-drug resistance
From 2014 to 2023, there were a total of 4,304 ETB patients, including 140 rifampicin-resistant patients and 4,164 non-resistant patients, who were divided into drug-resistant group and non-drug-resistant group, all of whom were aged 60–69 years, male, farmers, local household registration and referred patients, The age of 60–69 years old (t/x2 = 22.471, p < 0.05), population classification (t/x2 = 16.090, p < 0.05), floating population (t/x2 = 4.496, p < 0.05), referral (t/x2 = 19.418, p < 0.05), retreatment patients (t/x2 = 103.595, p < 0.05) in the rifampicin-resistant group were significantly higher than those in the non-resistant group, and the differences were statistically significant. There was no significant difference in gender (t/x2 = 3.647, p > 0.05), diabetes mellitus (t/x2 = 4.104, p > 0.05) and the use of fixed-dose procedure (FDC) (t/x2 = 0.425, p > 0.05) between the two groups (Table 3).
Distribution of rpoB gene mutations of rifampicin resistance in ETB patients
Among the 65 older adult rifampicin-resistant patients, 64 (98.46%) had a single gene mutation and 1 (1.54%) had a double gene mutation. The highest single gene mutation was Probe E, with 39 cases (60.00%), followed by Probe D, with 14 cases (13.86%). The double gene mutation was Probe A + B, 1 case (1.54%); In the older adult group and non-older adult group (t/x2 = 4.320, p < 0.05), initial treatment and retreatment group (t/x2 = 16.023, p < 0.05), Probe E was statistically significant, and the rest were not statistically significant Tables 4, 5.
Of the 65 drug-resistant patients, 52 (80.00%) were resistant to rifampicin only, and Probe E was the most mutated site, accounting for 31 cases (59.62%), followed by Probe D, 11 (21.15%). There were 13 cases (20.00%) of multidrug resistance, and the most mutation was Probe E, 8 cases (61.54%), followed by Probe D, 3 cases (23.08%). There was no significant difference in mutation sites between single rifampicin resistance and polydrug resistance (p > 0.05) (Table 6).
Treating outcomes of rifampicin-resistant ETB patients
Of 140 ETB rifampicin-resistant patients, 25 patients were excluded, 115 patients were analyzed, 31 cases were successfully treated, 84 cases were not successfully treated, The patients were mainly about 70 years old (t/x2 = 1.080, p > 0.05), male (t/x2 = 0.08, p > 0.05), farmers (t/x2 = 4.153, p > 0.05), local (t/x2 = 1.707, p > 0.05), referral patients (t/x2 = 0.962, p > 0.05), and the differences were not statistically significant. Whether the patient was retreated (t/x2 = 10.749, p < 0.05), multi-drug resistance (t/x2 = 5.898, p < 0.05), Xpert MTB first test (t/x2 = 4.968, p < 0.05), 0 month sputum sequence results (t/x2 = 8.550, p < 0.05) were statistically significant for the patient ‘s outcome (Table 7).
Discussion
In recent years, great achievements have been achieved in the prevention and control of tuberculosis in China, and it has been effectively controlled (16). However, rifampicin-resistant and multidrug-resistant tuberculosis have become major problems that harm public health due to their difficult treatment, low cure rate and great harm (17–19).
Nantong, a southeast coastal located open city in Jiangsu, China, has always taken TB prevention and control as an important object of public health prevention and control, and has implemented a series of measures in recent years to improve the discovery, diagnosis and treatment of rifampicin and MDR patients. At the end of 2018, Gene-Xpert molecular testing equipment was equipped in Nantong designated tuberculosis hospital, which greatly improved the detection capability and screening intensity of rifampicin-resistant tuberculosis in the city, and provided a strong technical guarantee for early detection and treatment of rifampicin-resistant tuberculosis (20).
Our retrospective study found that from 2014 to 2023, Nantong City has made remarkable achievements in TB prevention and control. The overall annual standardized incidence of tuberculosis patients showed a rapid decline and then tended to be stable. The ETB patients mainly had a higher reported rate of tuberculosis in males over 60 to 69 years old. The positive rate of retreatment and etiology was significantly higher than that of non-older adult people. According to the seventh census, the aging rate of Nantong City is 30.01%, ranking first in the country, and the older adult have many basic diseases, low immunity, irregular medication, and delayed medical treatment, becoming a high incidence of tuberculosis. The patients were mainly gathered in Rugao, Qidong and Tongzhou county, accounting for 18.82, 16.23 and 14.78%, respectively, which may be due to the large population base and serious aging in these three areas. Among them, the peak of the incidence of patients is mainly concentrated in March to September every year, and the incidence of low incidence cases in February accounted for 6.62% of the whole year, which may be related to the annual Lunar New Year, the change of floating population, and the routine physical examination of older adult people over 60 years old carried out from April to October every year, promoting more TB patients to be found.
In Nantong City, the ETB rifampicin-resistant patients were mainly male patients aged 60–69 years old, farmers, local household registration, and referred patients, with a ratio of 3:1, which may be related to male bad habits, high job mobility, and low income, reminding us that future prevention and control work should strengthen detection and publicity of older adult male population, especially in their 60–69 years old. Among the 65 ETB rifampicin-resistant patients from 2019 to 2023, single gene mutation was the dominant, with 64 cases (98.46%) of single gene mutations. The highest single gene mutation was Probe E, 39 cases (60.00%), followed by Probe D,14 cases (13.86%). The results of this study were similar to those of Ethiopia and Tanzania. These similarities indicated that frequent population movements and intensive contacts in a large number of low-income countries have significantly accelerated the mixed transmission of strains and led to the spread of mutant strains within the community. However, our findings were different from those in northeastern India, which showed that the most common mutations were at probes A and D, respectively. The frequency and pattern of rpoB mutations may vary geographically, and some mutations are more common in specific regions or Mycobacterium tuberculosis lineages (7, 9, 21). Probe E had statistical significance between the older adult group and the non-older adult group, and between the initial treatment and the re-treatment group, while the others had no statistical significance. There was no significant difference in mutation sites between rifampicin resistance and multidrug resistance. The ETB rifampicin-resistant patients in Nantong were mainly about 70 years old, male, farmer, local and referred patients, and the outcomes of them were not ideal, and the outcome of patients had statistical significance with initial retreatment, multi-drug resistance, Xpert MTB first test and 0-month sequential sputum smear results.
In summary, from 2014 to 2023, the ETB patients in Nantong City showed a rapid decline and then tended to be stable. They were mainly concentrated in 60–69 years old, males, farmers and patients with retreatment, and had the characteristics of poor treatment outcomes. Attention should be more paid to the patients with retreatment. The rpoB gene mutation was mainly a single gene mutation, with the highest is Probe E, which showed no difference with the mutation site of multi-drug resistant rpoB gene. Patients should take into account the epidemic characteristics of ETB rifampicin-resistant patients, and effectively develop prevention and control measures. In addition, there are still also some shortcomings in this study. For example, Xpert test was only carried out in Nantong at the end of 2018, resulting in a gap between the mutation data of rifampicin resistance in older adult people and the data of real older adult people, and the analysis conclusion may not be rigorous enough.
Conclusion
The prevention and treatment effect of ETB patients in Nantong City was significant, and the older adult patients with rifampicin resistance were a problem that needed attention. However, it still has some deficiencies in this study. For example, Nantong has only carried out Xpert testing since the end of 2018, which led to a gap between the mutation data of rifampicin resistance in the older adult and the drug resistance data of the real older adult, and the analysis conclusion may not be rigorous enough.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bagcchi S. WHO's global tuberculosis report 2022. Lancet Microbe. (2023) 4:e 20. doi: 10.1016/S 2666-5247(22)00359-7, PMID: 36521512 · doi ↗ · pubmed ↗
- 2Fathizadeh H Hayat SMG Dao S Ganbarov K Tanomand A Asgharzadeh M. Long non-coding RNA molecules in tuberculosis. Int J Biol Macromol. (2020) 156:340–6. doi: 10.1016/j.ijbiomac.2020.04.03032283111 · doi ↗ · pubmed ↗
- 3Lin J Jiang Y Liu D Dai X Wang M Dai Y. Early secreted antigenic target of 6-k Da of Mycobacterium tuberculosis induces transition of macrophages into epithelioid macrophages by downregulating i NOS / NO-mediated H 3K 27 trimethylation in macrophages. Mol Immunol. (2020) 117:189–200. doi: 10.1016/j.molimm.2019.11.013, PMID: 31816492 · doi ↗ · pubmed ↗
- 4Dornelas Moreira J Rodrigues Silva Hde Paulo Coelho Vde Toledo P Dabes TMP. Guimaraes: microparticles in the pathogenesis of TB: novel perspectives for diagnostic and therapy management of Mycobacterium tuberculosis infection. Microb Pathog. (2020) 144:104176. doi: 10.1016/j.micpath.2020.104176, PMID: 32244042 · doi ↗ · pubmed ↗
- 5Lohiya A Suliankatchi Abdulkader R Rath RS Jacob O Chinnakali P Goel AD. Prevalence and patterns of drug resistant pulmonary tuberculosis in India-a systematic review and meta-analysis. J Glob Antimicrob Resist. (2020) 22:308–16. doi: 10.1016/j.jgar.2020.03.008, PMID: 32247079 · doi ↗ · pubmed ↗
- 6Chakaya J Khan M Ntoumi F Aklillu E Fatima R Mwaba P. Global tuberculosis report 2020 - reflections on the global TB burden, treatment and prevention efforts. Int J Infect Dis. (2021) 113:S 7–S 12. doi: 10.1016/j.ijid.2021.02.107, PMID: 33716195 PMC 8433257 · doi ↗ · pubmed ↗
- 7Akalu GT Tessema B Petros B. High proportion of RR-TB and mutations conferring RR outside of the RRDR of the rpo B gene detected in Gene Xpert MTB/RIF assay positive pulmonary tuberculosis cases, in Addis Ababa, Ethiopia. P Lo S One. (2022) 17:e 0277145. doi: 10.1371/journal.pone.0277145, PMID: 36584037 PMC 9803184 · doi ↗ · pubmed ↗
- 8Isakova J Sovkhozova N Vinnikov D Goncharova Z Talaibekova E Aldasheva N. Mutations of rpo B, kat G, inh A and ahp genes in rifampicin and isoniazid-resistant Mycobacterium tuberculosis in Kyrgyz Republic. BMC Microbiol. (2018) 18:22. doi: 10.1186/s 12866-018-1168-x, PMID: 29566660 PMC 5863813 · doi ↗ · pubmed ↗