The Impact of Gender, Training Year, Medical Specialty and the COVID‐19 Pandemic on Resident Wellness
Sara Beachy, Jessica Luzier, Chantel Weisenmuller, Kathleen Bors, Mary Ann Maurer, Amna Anees, Tiffany Lasky, Lisa Calderwood

TL;DR
This study explores how factors like gender, training year, and the pandemic affect medical trainees' wellness, using data from 2019 to 2022.
Contribution
The study uses a person-centered statistical approach to identify distinct resident wellness profiles influenced by intersecting identities and the pandemic.
Findings
Female residents and those in medical/pharmacy programs had lower wellness scores.
The impact of the pandemic on wellness varied by residency year and program type.
Advanced medical residents experienced lower wellness in the latter part of the pandemic.
Abstract
Data are limited as to which factors most strongly impact medical trainees' well‐being, and few studies have assessed trainee's wellness at multiple time points during the COVID‐19 pandemic. Additionally, much research has not taken an intersectional approach to understanding the ways in which different facets of a resident's identity impact their wellness. Thus, more person‐centred, probability‐driven statistical approaches that can produce distinct heterogenous groups of individuals are warranted to understand the way in which different identities are associated with resident wellness scores. A latent profile analysis was conducted using institutional data from resident surveys administered from 2019 to 2022. We had a 78.8% response rates for a total of 1101 surveys completed and 1033 retained for data analysis (i.e., 662 medical residents, 204 surgical residents, 48 pharmacy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
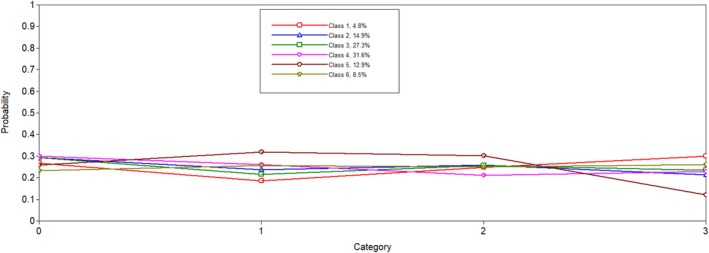 FIGURE 1
FIGURE 1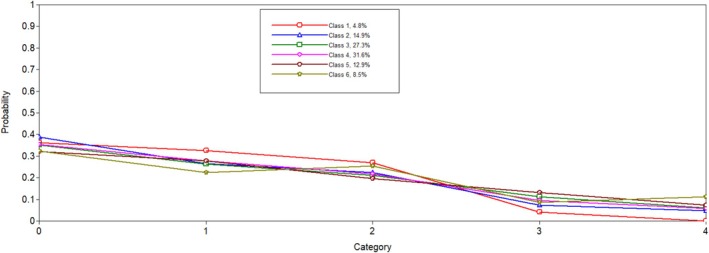 FIGURE 2
FIGURE 2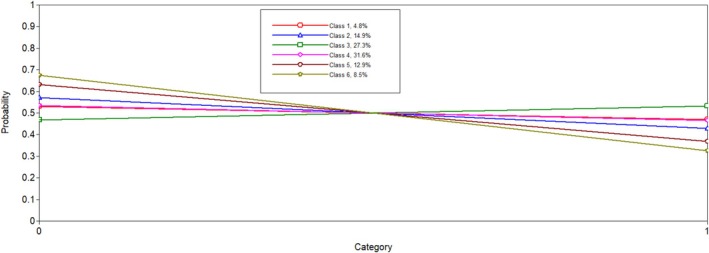 FIGURE 3
FIGURE 3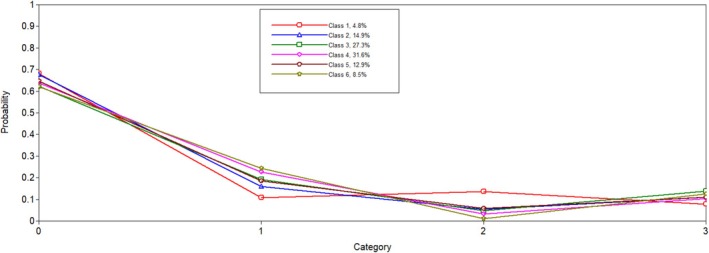 FIGURE 4
FIGURE 4| Latent class | AIC | SABIC | ENTROPY |
|---|---|---|---|
| 2 | 14878.16 | 14934.61 | 0.79 |
| 3 | 14176.68 | 14259.59 | 0.86 |
| 4 | 13599.15 | 13708.52 | 0.90 |
| 5 | 13343.19 | 13479.02 | 0.90 |
| 6 | 13186.18 | 13348.47 | 0.89 |
| Advanced Medical and Pharmacy Residents | First Year Wellness | Average Wellness in Females | Average Majority Pre‐COVID | Transitioning Through COVID | Doing Well | |
|---|---|---|---|---|---|---|
| Pre‐COVID | 0.267 | 0.292 | 0.294 |
| 0.259 | 0. |
| Early COVID |
| 0.236 | 0.215 | 0.260 |
| 0.256 |
| COVID MID I | 0.248 | 0.258 | 0.256 |
|
| 0.250 |
| COVID MID II |
| 0.213 | 0.236 | 0.229 |
| 0.261 |
| PGY1 | 0.362 |
| 0.351 | 0.353 |
| 0.324 |
| PGY2 |
| 0.265 | 0.264 | 0.279 | 0.278 |
|
| PGY3 |
| 0.224 | 0.212 | 0.217 |
| 0.255 |
| PGY4 | 0. | 0.074 | 0.112 | 0.094 | 0. | 0.086 |
| PGY5 |
| 0.048 | 0.061 | 0.058 | 0.072 |
|
| Male | 0.530 | 0.571 |
| 0.535 | 0.632 |
|
| Medical |
| 0.676 | 0.622 | 0.638 | 0.647 |
|
| Surgical |
| 0.160 | 0.193 | 0.226 | 0.186 |
|
| Pharmacy |
| 0.054 | 0.048 | 0.033 | 0.058 |
|
| Unspecified |
| 0.110 |
| 0.104 | 0.109 | 0.126 |
| Meaning |
| 2.82 | 3.37 | 3.87 | 4.28 |
|
| Human Connection |
| 3.08 | 3.51 | 3.96 | 4.41 |
|
| Overall |
| 2.94 | 3.45 | 3.92 | 4.34 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · Diversity and Career in Medicine · COVID-19 and Mental Health
Introduction
1
Medical accrediting bodies include trainee wellness as a core competency in programming while striving to advance and improve the quality of education. Whereas many factors influence resident wellness, few studies examine resident wellness from an intersectional lens; however, programmes often implement broad institutional‐level wellness programming without consideration of nuances in residents' experiences. To complicate scholarship further, wellness and well‐being are frequently used interchangeably, which has led to a lack of theoretically grounded research and wellness programmes. The authors of a recent review proposed that wellness should include mental, social and physical health in addition to well‐being, which includes deriving meaning from life and work [1]. Therefore, wellness will be used in this manuscript as an umbrella term for well‐being.
Research demonstrates that resident identities may impact wellness. Female residents report higher levels of perceived stress, burnout and gender‐based discrimination and lower life security and overall wellness as compared with their male peers [2, 3, 4, 5]. Generally, residents who are farther along in training are more likely to report feeling their work is meaningful, greater life security and more institutional support than residents earlier in their training [3]. Unfortunately, there is more limited research to delineate differences in resident wellness across specialty areas and throughout the COVID‐19 pandemic. Broadly, COVID‐19 has been associated with increased distress, depression, anxiety and burnout among physicians, but little is known about its impact on resident wellness [6, 7, 8]. However, studies have found an initial spike in residents' concerns for their own wellness early in COVID‐19 with hospital‐based residents experiencing increased loneliness when compared to surgical residents [9, 10]. These findings suggest that COVID‐19 influenced resident wellness but that the pandemic's influence may depend on resident factors.
Present Study
1.1
The present study analysed factors that contribute to resident wellness using surveys administered from 2019 to 2022. As the scholarship is mixed on which factors influence wellness, we employed an intersectionality lens to help identify unique patterns in the data. Intersectionality was first introduced by Kimberlé Crenshaw and can be useful to identify the ways intersecting identities influence a person's lived experiences [11]. We conceptualised programme specialty, gender and year in programme as identities that influence the amount of power residents have in their respective institution and department and hypothesised that wellness scores would be lower in female and residents earlier in training.
Methods
2
Settings and Participants
2.1
Residents across all departments in a university‐affiliated hospital in the United States located in Appalachia were administered surveys between May 2019 and December 2022 by our institution's GME Office in cooperation with Wayne State University. Retrospective use of the data was approved by the hospital's Institutional Review Board (IRB) for the Protection of Human Subjects. We received 1101 completed surveys. Sixty‐three surveys were excluded as the individuals indicated they were not residents or respondents did not identify a gender. We chose to exclude these surveys because a response other than male or female could indicate (a) a non‐binary or gender non‐conforming identity, (b) the desire to remain anonymous in certain programmes or (c) missing data. Of note, we recognise the differences between gender and biological sex; however, as this was a retrospective study, we could not control for the way gender was asked in the demographics survey.
Outcomes
2.2
Resident Wellness Scale
2.2.1
The Wayne State Resident Wellness Scale (RWS) is used by the Accreditation Council for Graduate Medical Education [3, 12]. This 10‐item, self‐report measure uses a 5‐point Likert scale to capture residents' experiences over a 3‐week period [3]. The RWS is based on Ryff and Keyes' theory of wellness and provides an overall score and four subscale scores: meaningful work/ability, life security, institutional support and social support/personal growth [3, 13]. We previously conducted a confirmatory factor analysis on the RWS using data from this same institute [14]. We found a factor structure similar to the 2‐factor structure identified by Appelbaum et al. sans item 3 [14, 15]. Therefore, two factors labelled as meaning (i.e., items 1, 2, 4, 5, 6 and 10) and human connections (i.e., items 7, 8 and 9) were used in the analysis. Reliability statistics for this study were acceptable for the total score (α = 0.89) and subscales (α = 0.74–0.87).
Programme Type
2.2.2
Residency programmes were categorised as medical (i.e., paediatrics, behavioural medicine/psychiatry, emergency medicine, family medicine, internal medicine and cardiology), surgical (i.e., obstetrics/gynaecology, general surgery, vascular surgery and urology), pharmacy and unspecified.
COVID‐19 Timeframe
2.2.3
Responses were categorised into four time periods based on survey completion: pre‐COVID‐19, prior to the first detected US case of COVID‐19; early COVID‐19, first US case until the first vaccine received emergency approval (1/30/2020–12/10/2020); Mid I COVID‐19, after the first vaccine was approved until omicron (12/11/2020–12/1/2021); and Mid II COVID‐19 (12/2/2021 to end of study).
Other Demographics
2.2.4
Residents were coded as male (0) or female (1). Residents indicated their year (i.e., PGY1–PGY5).
Statistical Analyses
2.3
Latent Profile Analysis
2.3.1
Mplus v. 8.9 was utilised for the latent profile analysis (LPA), whereas SPSS v. 29 was utilised for descriptive statistics. LPA is a person‐centred, probability‐based statistical analysis that groups participants together based on pattern of responses to items [16]. This analysis has been used to analyse intersecting identities and experiences on outcomes, thereby assessing intersectionality [17]. LPA assumes that people who score similarly on measures (e.g., wellness) have similar profiles (e.g., gender, year of residency, residency subtype and environmental factors—COVID time points) and groups people by calculating the probability for each person within each group [18]. In this analysis, an intersectionality lens would suggest that residents with differing levels of social power based on intersecting identities would have differing levels of wellness. Per best practices, LPA is iterative where multiple models with varying numbers of profiles are compared to one another. Multiple indices must be used to identify which model is the best fit for the data [16].
Fit indices (i.e., Akaike Information Criterion [AIC] and sample‐sized adjusted Bayesian Information Criterion [SABIC]), entropy, average latent profile probabilities, class size proportion and the bootstrapped likelihood ratio test were all simultaneously evaluated for each model [16]. The AIC and SABIC are information criteria fit indices that consider sample size and model complexity to help identify the ideal number of classes (i.e., highest quality model) where values closer to 0 indicate better fitting models [16, 19]. The parametric bootstrapped likelihood ratio test (BLRT) was evaluated with a significant result, indicating a meaningful difference between two solutions [16]. Entropy and diagonal probability values greater than 0.80 and 0.70, respectfully, indicated that individuals are classified appropriately into their respective class, which are well separated and well defined [16, 20]. Classes should be no less than 5%–8% of the sample and should be theoretically driven [20]. Conceptually, we anticipated smaller class sizes given the gender disparity in certain specialties. For example, female residents comprise only 18% of orthopaedic surgery residents [21]. Furthermore, 73% of these residents are European‐American, whereas number of Black, Latinx and Indigenous residents ranges between 0.2% and 7.2% [21]. Although we did not have access to racial makeup, we anticipated small classes based on shared gender and racial experiences related to power and positionality.
Results
3
Sample Demographics
3.1
Twenty‐eight per cent of the surveys (n = 294) were administered pre‐COVID‐19, 25% completed during early COVID‐19, 25% completed at COVID‐19 Mid I, and 22% completed at COVID‐19 Mid II. Most residents (n = 366) indicated that they were PGY1 (35%). Approximately 55% of respondents indicated they were male. Most residents were in medical (n = 662, 64%) and surgical programmes (n = 204, 20%). The remainder did not specify a programme (12%) or were in pharmacy residency (5%).
Latent Profile Modelling
3.2
Six latent profiles analyses were conducted and compared to one another to determine the best solution. Notably, when the five and six latent profile analyses were conducted, a message on Mplus indicated that at least one logit threshold approached a 0 or 1, indicating a perfect prediction. Results were reviewed to ensure plausibility, and only one extreme logit threshold was identified. In both solutions, the probability of PGY5 residents in Latent Class 1 was 0. We determined this result was plausible given the low probability of individuals in this class being in surgical programmes, which are longer in length. When examining all fit indicators (i.e., entropy, AIC, SABIC, size of each class and average latent class probabilities; see Table 1), the six‐class model was favoured. The BLRT test for five classes versus six classes was significant (p < 0.001), which indicated that the six‐class solution fit better than the five‐class solution. The results of the latent class analysis are presented in Table 2. Additionally, Figures 1, 2, 3, 4 depict probabilities of each variable input (i.e., COVID time point, PGY, biological sex and programme type) by latent class.
COVID‐19 time point.
PGY.
Biological sex.
Programme type.
Class 1, Advanced Pharmacy and Medical Residents Wellness (n = 48, 5%), was the smallest group and composed of individuals who had the lowest wellness scores. This class had the highest probability of having individuals who are in a medical programme (0.681) and pharmacy programme (0.135). This class also had the lowest probability of having been surveyed in early‐COVID‐19 (0.19) but had the highest probability of being surveyed in COVID‐19 Mid II (0.30). This group had the highest probabilities of individuals who were in their second and third years (0.33 and 0.27).
Class 2, First Year Wellness (n = 156, 15%), was characterised by having the second poorest scores on the wellness measure. This class had the second highest probability of individuals who were in a medical programme (0.676) but had the highest probability of individuals in their first year (0.389). This class was more likely to be male (0.571).
Class 3, Average Wellness in Females, was the second largest group (n = 278, 27%) and was characterised by the highest probability of being female (0.532). This class had the third lowest scores on the overall wellness measure and each subscale but had the highest probability of individuals who did not specify a programme type (0.138).
Class 4, Average Majority Pre‐COVID (n = 332, 32%), was characterised by being the largest class and having the third highest wellness scores. This class had the highest probability of being surveyed pre‐COVID‐19 (0.30) and had a higher probability of being male (0.535). Additionally, this class had the second highest probability of having surgical residents (0.236).
Class 5, Transitioning Through COVID (n = 131, 13%), was characterised by the lowest probability of individuals being surveyed during the last part of COVID‐19 (0.120) but had the highest probability of individuals being surveyed during the early part of COVID‐19 (0.319) and COVID‐19 Mid I (0.301). This class had the second highest scores on the wellness measure. Additionally, this class had the second highest probability of being male (0.632). Lastly, this class had the lowest probabilities of having PGY1 and PGY3 residents (0.321 and 0.196, respectively) but had the highest probability of having PGY4 residents (0.132).
Class 6, Doing Well, was the second smallest group (n = 88, 9%) and was characterised by having the highest scores on the wellness measure. This class had the highest probability of having individuals in a surgical programme (0.243) but had the lowest probability of individuals in a medical programme (0.620). Individuals in this class had the highest probability of being male (0.674). This class had the highest probability of having individuals in their fifth year (0.112).
Discussion
4
In this study, a LPA was utilised to identify whether residents' intersecting positionalities and timeframes throughout COVID‐19 impacted scores on wellness. Broadly, classes that had higher probabilities of being male, in surgical programmes, and were in Years 4 and 5 of their residencies had higher scores on the wellness measure. In terms of the influence of COVID‐19 on wellness scores, it was more difficult to ascertain a particular pattern. However, one class that had higher probabilities of residents being surveyed in 2022 had the lowest wellness scores.
Biological Sex
4.1
The two classes with the highest wellness scores had the highest probabilities of being male (i.e., Wellness Transition during COVID‐19 and Doing Well). The class with the highest probability of being female, Average Female Wellness, had the third lowest wellness scores, meaning that of the six classes, this class ranked in the bottom half in terms of wellness scores. These findings align with previous results that found that, generally, female residents had poorer subjective wellness ratings when compared to male residents [2, 3, 4]. This may indicate that the average female, regardless of residency type, year and COVID‐19 timeframe, have lower wellness scores than males. However, classes that were more mixed in terms of biological sex were more nuanced on their scores, which may be explained by residents' intersecting positionality.
Intersecting Identities
4.2
The two lowest scoring classes, Advanced Pharmacy and Medical Residents Wellness and First Year Wellness, were heterogenous in terms of biological sex but had the highest probabilities of individuals in a medical or pharmacy programme and who were early to midway through their training. This may indicate that medical and pharmacy residents early to midway through training tend to have lower scores on wellness measures when compared to surgical residents, particularly male surgical residents. Though intersectional research regarding residents is limited, Felton et al. found that surgery residents in PGY1 and PGY2 rated their wellness more poorly, which was further influenced by sex as male residents were more likely to perceive an increase in wellness when their PGY level changes [22]. Although this finding is specific to surgical residents, it aligns with theoretical implications—residents earlier in their training undoubtedly have less power and influence, which may be further exacerbated by being female. This may be especially true for frontline medical residents who experienced increased demands during COVID‐19.
COVID‐19
4.3
Broadly, we found it difficult to ascertain meaningful patterns based on COVID‐19 in several classes. Most classes' probabilities related to COVID‐19 time points ranged between 0.21 and 0.29. Whereas previous studies have found that COVID‐19 had an initial impact on residents' perceptions of wellness, other studies indicated that COVID‐19 did not contribute to meaningful changes pre‐ and post‐pandemic [9, 23, 24]. Findings from this study suggest reasons for this varying results—the pandemic may have uniquely impacted residents based on their intersecting identities.
The largest class, Average Majority Pre‐COVID‐19, most likely had the largest raw number of individuals surveyed pre‐COVID‐19 and therefore may represent what ‘average’ wellness looked like pre‐COVID‐19. However, the range of probabilities across time points was relatively narrow (0.21–0.30), which makes interpretation difficult. The Advanced Pharmacy and Medical Residents Wellness class had the lowest probability of being surveyed in early 2020 but had the highest probability of being surveyed in 2022. The Transitioning Through COVID‐19 class had the highest probabilities of being surveyed early in the pandemic but had the lowest probability of being surveyed in 2022. This may indicate that some residents (i.e., male and advanced surgical) had increased wellness throughout the first parts of COVID‐19, but a small subset (i.e., advanced pharmacy and medical) experienced a decrease in wellness during the later parts. These findings are partially aligned with previous results, which found that advanced medical students had increased mental health concerns during COVID‐19 [25]. However, our findings extend the research by indicating that programme type, not just year in training, directly influences wellness in periods of extended crisis, possibly due to increased stress of being on the frontlines. Indeed, previous research showed general decreases in sense of belonging in addition to significant differences in loneliness between surgical and medical residents during the latter part of 2020 [9, 26]. Further, other research found decreased wellness in students during the latter part of COVID‐19 than the first, particularly among females, which reinforces the temporal impact COVID‐19 may have had on certain groups of individuals [27].
Recommendations
4.4
Many resident wellness initiatives have been described in the literature, such as restrictions on duty hours, stress management treatments and mindfulness trainings, which are often initiated broadly across departments. However, our data suggest that wellness programming needs to be tailored by gender, programme type and year in programme, given that female, medical and pharmacy and early‐ to mid‐level residents consistently demonstrate more vulnerability. Broadly, these groups may benefit from wellness initiatives that focus on building social cohesion among and between cohorts (e.g., first years across all programmes), skills to navigate the power dynamics within the medical system and increased focus on diversity and equity considerations, despite political pressure to not do so. Given the political climate, fostering belongingness may be especially imperative for residents who are minorities and subsequently do not have as much power across systems of influence.
In this study, the Advanced Medical and Pharmacy Residents group may have benefited from continued emphasis on wellness that may have been present early during the pandemic, increased support as residents transitioned from PGY1 to PGY2, reminders of how their work aligned with their values and increased wellness initiatives across specialties (e.g., combining pharmacy and internal medicine residents) to increase belongingness and decrease loneliness. In addition to these suggestions, First Year Medical Residents may have benefited from increased support and understanding of policies to mitigate uncertainty and stress. The Average Female group may have benefited from increased mentorship and a thorough examination of institutional policy and resources to identify and mitigate gender bias. Regardless of these suggestions, future qualitative research should be used to elicit resident feedback to design more tailored wellness interventions.
Limitations
4.5
Unfortunately, we were unable to capture the experiences of people who are transgender or gender nonconforming. We were hesitant to code missing data as someone being a gender minority as some females may have been hesitant to share their sex if they were in a subspecialty or year that was male‐dominated and vice versa. Therefore, we were unable to accurately identify which missing response was due to missing data or actual non‐response. Future studies should include more expansive options for gender, race, sexual orientation and disabilities; however, programme directors and researchers should seriously weigh the unintended consequences of asking people to disclose certain identities. Studies from a single institution exponentially increase the potential for someone identifying a minority resident as being part of a study, which may impact safety. One way that researchers and programme directors could increase safety is by grouping data from across institutions, which will increase future studies' sample sizes while providing more safety for minority residents. Additionally, further study is necessary to better understand the construct validity of the RWS. Finally, these results are based on residents from a single institution in Appalachia, which may limit generalisability.
Conclusions
5
Gender, programme type and year in programme affect resident wellness, whereas COVID‐19 time point had a moderate impact on wellness.
Author Contributions
Sara Beachy: software, methodology, formal analysis, visualisation, writing – original draft, writing – review and editing, conceptualisation. Jessica Luzier: conceptualisation, data curation, investigation, supervision, resources, project administration, writing – original draft, writing – review and editing. Chantel Weisenmuller: conceptualisation, writing – original draft, writing – review and editing, methodology. Kathleen Bors: conceptualisation, resources, project administration, investigation, writing – original draft, writing – review and editing. Mary Ann Maurer: conceptualisation, project administration, writing – original draft, writing – review and editing. Amna Anees: conceptualisation, investigation, writing – original draft, writing – review and editing, project administration. Tiffany Lasky: conceptualisation, writing – original draft, writing – review and editing. Lisa Calderwood: conceptualisation, project administration, writing – original draft, writing – review and editing.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1K. J. S. Brady , M. T. Trockel , C. T. Khan , et al., “What Do We Mean by Physician Wellness? A Systematic Review of Its Definition and Measurement,” Academic Psychiatry 42, no. 1 (2018): 94–108.28913621 10.1007/s 40596-017-0781-6 · doi ↗ · pubmed ↗
- 2Wayne State University Medical School and A. Messman , “Can We Actually Improve Resident Wellness? Pilot Data From a Longitudinal Wellness Curriculum for Emergency Medicine Residents,” Journal of Wellness 1, no. 1 (2019): 1–6.
- 3R. B. Stansfield , D. Giang , and T. Markova , “Development of the Resident Wellness Scale for Measuring Resident Wellness,” Journal of Patient Centered Research and Reviews 6, no. 1 (2019): 17–27.31414020 10.17294/2330-0698.1653 PMC 6676753 · doi ↗ · pubmed ↗
- 4M. D. Nguyen , A. M. Stocks , H. N. Anksorus , and S. C. Harris , “Assessing the Mental Health, Physical Health, and Well‐Being of Doctor of Pharmacy Students,” Currents in Pharmacy Teaching & Learning 15, no. 2 (2023): 170–177.36922330 10.1016/j.cptl.2023.02.023 · doi ↗ · pubmed ↗
- 5A. Espaillat , D. K. Panna , D. L. Goede , M. J. Gurka , M. A. Novak , and Z. Zaidi , “An Exploratory Study on Microaggressions in Medical School: What Are They and Why Should We Care?,” Perspectives on Medical Education 8, no. 3 (2019): 143–151.31161479 10.1007/s 40037-019-0516-3PMC 6565651 · doi ↗ · pubmed ↗
- 6K. Cohan , J. Nghiem , R. Mital , L. Willis , and L. Jiang , “Emergency Medicine Physician Stressors, Needs, and Wellness Resources During the Acute Phase of the COVID‐19 Pandemic in New York City,” Physician Leadership Journal 9, no. 6 (2022): 16–21.
- 7H. Kelker , K. Yoder , P. Musey , et al., “Prospective Study of Emergency Medicine Provider Wellness Across Ten Academic and Community Hospitals During the Initial Surge of the COVID‐19 Pandemic,” BMC Emergency Medicine 21, no. 1 (2021): 36.33761876 10.1186/s 12873-021-00425-3PMC 7988634 · doi ↗ · pubmed ↗
- 8R. M. Rodriguez , A. J. Medak , B. M. Baumann , et al., “Academic Emergency Medicine Physicians' Anxiety Levels, Stressors, and Potential Stress Mitigation Measures During the Acceleration Phase of the COVID‐19 Pandemic,” Academic Emergency Medicine 27, no. 8 (2020): 700–707.32569419 10.1111/acem.14065 PMC 7361565 · doi ↗ · pubmed ↗