The Choice of Hip Arthroplasty: HRA or THA? Revealed by Meta‐Analysis
Xiao Fan, Yimin Zhou, Tianyu Zhou, Justin P. Cobb, Tengbo Yu

TL;DR
This study compares hip resurfacing and total hip replacement surgeries, finding both safe but with different benefits like less blood loss and longer operation time.
Contribution
A meta-analysis comparing HRA and THA, revealing HRA's safety and efficacy with less blood loss and fewer complications.
Findings
HRA and THA have similar revision rates and functional outcomes.
HRA results in less blood loss and fewer complications but longer operation time.
HRA is suitable for young male patients needing high-level activity.
Abstract
Total hip arthroplasty (THA) is the gold standard for end‐stage hip arthrosis, while hip resurfacing arthroplasty (HRA) is considered a more bone‐conserving alternative. This meta‐analysis aimed to compare the safety and clinical efficacy of HRA and THA. The databases of PubMed, EMBASE, Cochrane Library, and CNKI were searched for RCTs comparing HRA and THA in treating hip arthrosis from database initiation to April 2024. Inclusion and exclusion criteria were defined, and data extraction, quality evaluation, and risk bias assessment were performed. A meta‐analysis was conducted using appropriate RevManv5.4 and Stata v14.0 software. Twenty RCTs from six countries were included. HRA had a similar revision rate, function scores (WOMAC, HSS, OHS, UCLA activity score, EQ‐D, EQ‐5D VAS), and blood levels of cobalt and chromium compared to THA. HRA had fewer complications and less blood loss…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
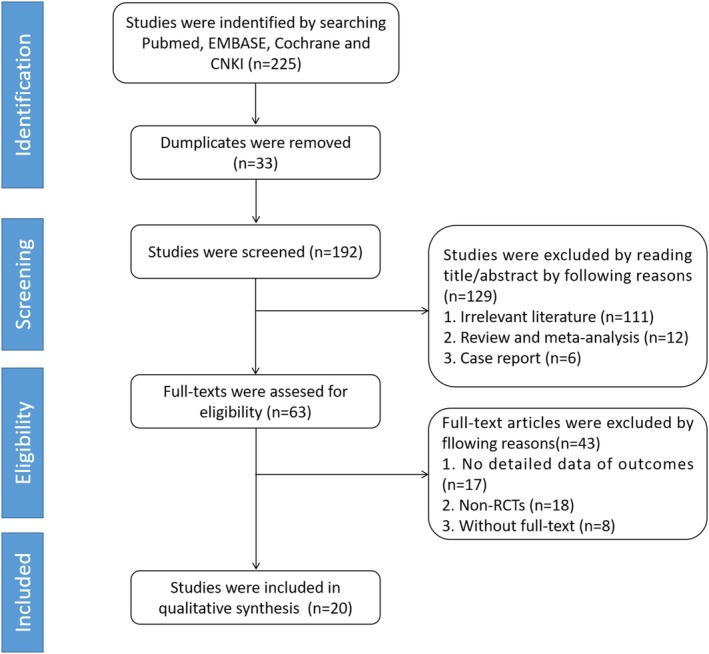 FIGURE 1
FIGURE 1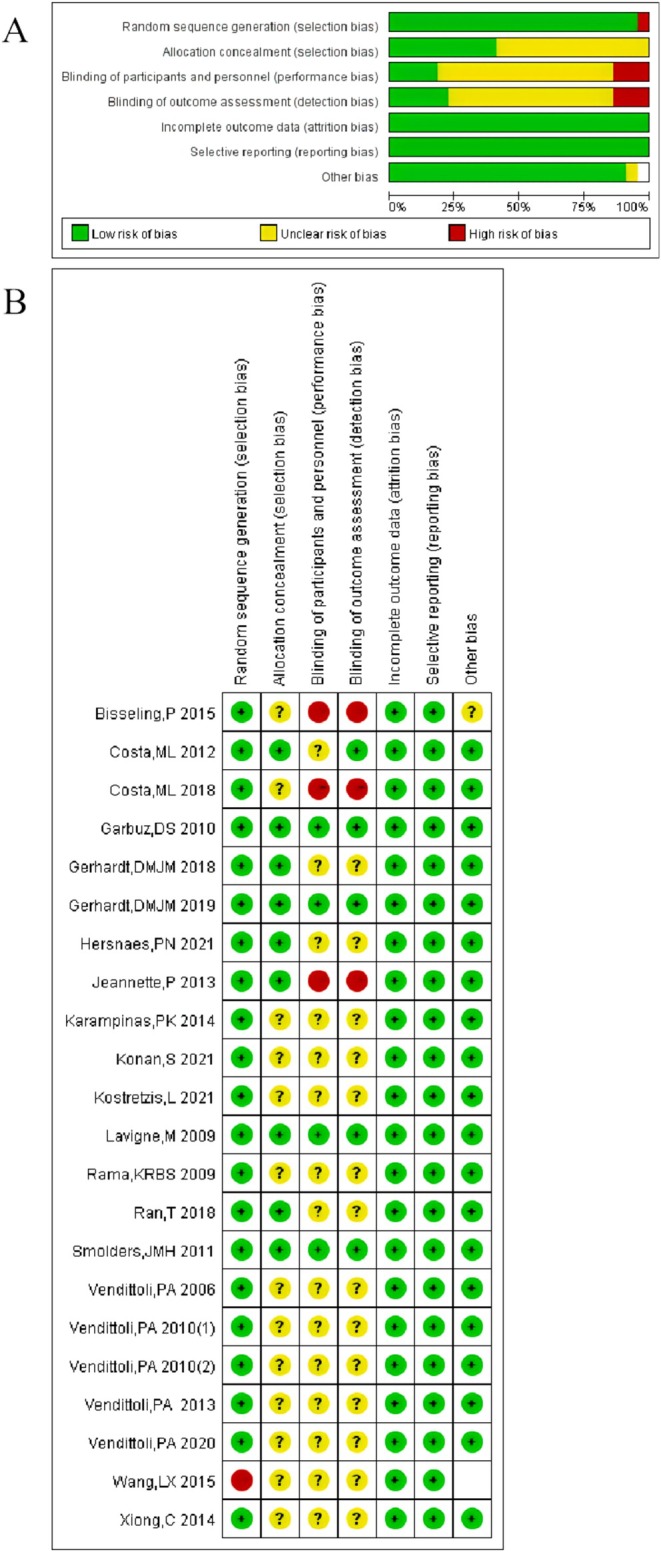 FIGURE 2
FIGURE 2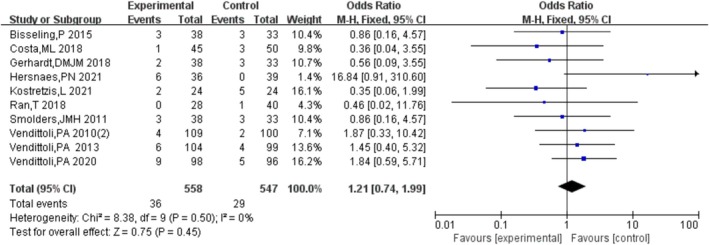 FIGURE 3
FIGURE 3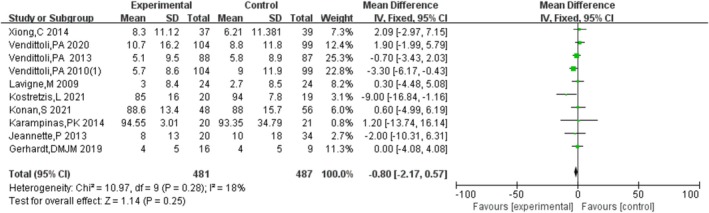 FIGURE 4
FIGURE 4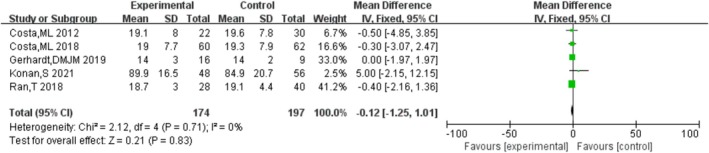 FIGURE 5
FIGURE 5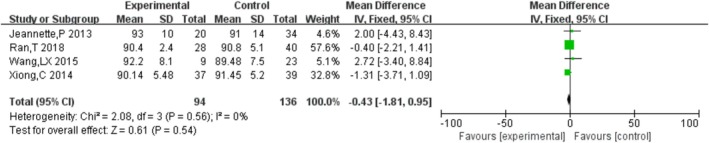 FIGURE 6
FIGURE 6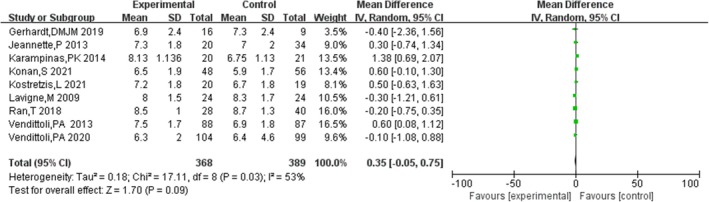 FIGURE 7
FIGURE 7 FIGURE 8
FIGURE 8 FIGURE 9
FIGURE 9 FIGURE 10
FIGURE 10 FIGURE 11
FIGURE 11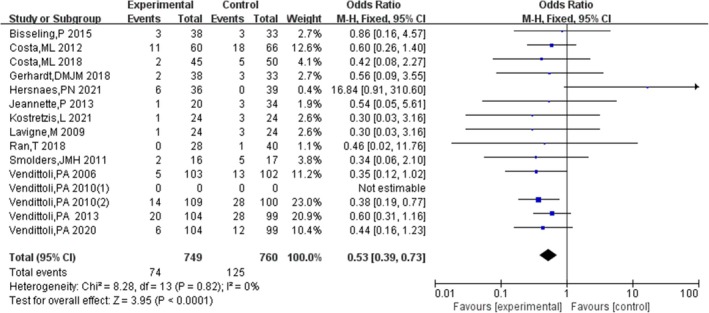 FIGURE 12
FIGURE 12 FIGURE 13
FIGURE 13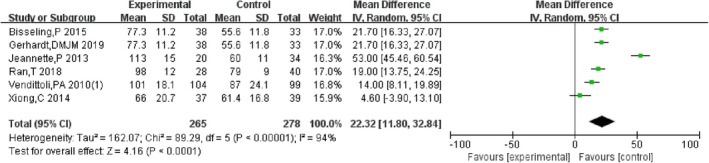 FIGURE 14
FIGURE 14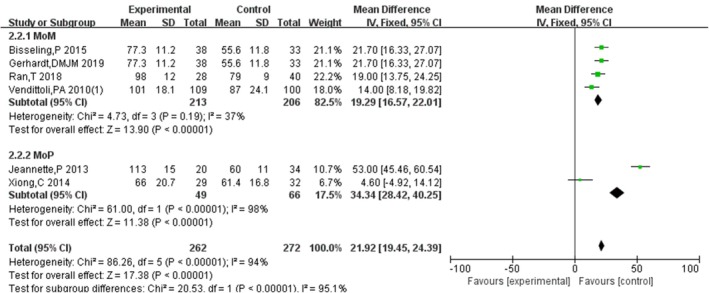 FIGURE 15
FIGURE 15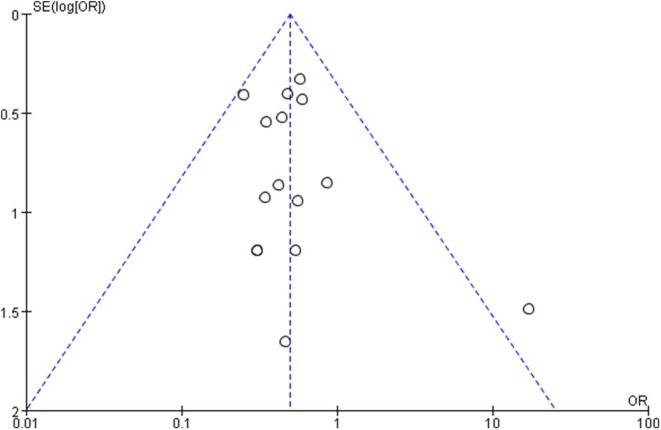 FIGURE 16
FIGURE 16| Study | Group |
| Age (years) | Diagnose (OA/AVN/other) | Height (m) | BMI (kg/m2) | Follow‐up (years) | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Bisseling (2015) |
HRA THA |
38, 21/17 33, 21/12 |
57.5 (50–61) 59.2 (51–61) |
35/1/2 31/0/2 | NR |
26.1 (3.1) 28 (5.1) |
≥ 3 ≥ 3 | ①⑨⑪ |
| Costa (2012) |
HRA THA |
60, 38/22 66, 36/30 |
56.3 (7.3) 56.6 (6.6) |
58/0/2 61/0/5 | NR |
28.6 (6.3) 28.7 (4.6) |
≥ 3 ≥ 3 | ③⑥⑦⑨ |
| Costa (2018) |
HRA THA |
60, 36/24 62, 35/27 |
56.5 (6.9) 56.7 (7.0) | NR | NR |
28.4 (6.2) 28.9 (4.8) |
≥ 3 ≥ 3 | ①③⑥⑦⑨⑩⑪ |
| Gerhardt (2018) |
HRA THA |
38, 21/17 33, 21/12 |
54.4 (9.5) 56.5 (7.3) |
35/1/2 31/0/2 | NR |
26.1 (3.1) 28 (5.1) |
≥ 3 ≥ 3 | ①⑨ |
| Gerhardt (2019) |
HRA THA |
16, 11/5 9, 8/1 |
52 (10) 57 (8) | NR |
1.77 1.80 |
26 (3) 28 (5) |
≥ 5 ≥ 5 | ③⑦⑪ |
| Hersnaes (2021) |
HRA THA |
36, 26/10 39, 26/13 |
59.4 (51.2–63.58) 61.9 (56.5–63.2) | NR | NR |
27.45 28.4 |
≥ 5 ≥ 5 | ①⑨ |
| Jeannette (2013) |
HRA THA |
20, 12/8 34, 24/10 |
57 (54–61) 56 (52–62) | NR | NR |
28 (24–31) 27 (25–29) |
≥ 2 ≥ 2 | ②⑤⑥⑨⑩⑪ |
| Karampinas (2014) |
HRA THA |
15, 7/8 16, 11/5 |
50.47 (9.68) 56 (52–62) |
11/0/4 11/0/5 | NR |
31 (4.14) 31.6 (3.71) |
≥ 2 ≥ 2 | ②⑤ |
| Konan (2021) |
HRA THA |
48, 43/5 56, 50/6 |
51.5 52 | NR | NR |
28.3 28.2 |
≥ 8 ≥ 8 | ②③⑤ |
| Kostretzis (2021) |
HRA THA |
24, 14/10 24, 15/9 |
50 (7.1) 50 (7.8) |
18/1/5 19/2/3 | NR |
28 (5.9) 28 (4.1) |
≥ 12 ≥ 12 | ①②⑤⑧⑨ |
| Lavigne (2009) |
HRA THA |
24, 14/10 24, 15/9 |
49.6 (38–63) 49.8 (33–62) | NR | NR |
27.9 (20.2–36.9) 27.8 (20.2–35.6) |
≥ 1 ≥ 1 | ②⑤⑨ |
| Ran (2018) |
HRA THA |
28, 19/9 40, 28/12 |
43 (23–64) 47 (22–64) |
7/18/3 5/32/3 | NR |
21.5 (17.8–25.7) 21.8 (17.2–26.2) |
≥ 5 ≥ 5 | ①③④⑤⑨⑩⑪ |
| Smolders (2011) |
HRA THA |
38, 21/17 33, 21/12 |
58 (24–65) 59 (37–65) |
35/1/2 31/0/2 | NR |
26 (3.1) 28 (5.1) |
≥ 2 ≥ 2 | ①⑨ |
| Vendittoli (2006) |
HRA THA |
107, 67/40 103, 70/33 |
49.1 (23–64) 50.6 (24–65) |
81/3/26 78/2/17 |
1.72 1.72 |
27.2 (17.6–44.9) 29.6 (17.4–49.1) |
≥ 1 ≥ 1 | ⑨ |
| Vendittoli (2010) (1) |
HRA THA |
109, 69/40 100, 68/32 |
49.2 (9.0) 51 (8.6) |
84/3/22 78/2/20 |
1.72 1.72 |
27 (5.3) 30 (6.1) |
≥ 2 ≥ 2 | ②⑨⑪ |
| Vendittoli (2010) (2) |
HRA THA |
64, 42/22 53, 33/20 |
49.3 (25–64) 51 (30–65) |
45/1/18 41/1/11 |
1.71 (1.50–188) 1.71 (1.51–188) |
27.1 (17.6–44.9) 29.2 (21.3–48.1) |
≥ 2 ≥ 2 | ①⑨ |
| Vendittoli (2013) |
HRA THA |
109, 72/37 100, 68/32 |
49.2 (23–64) 51 (24–65) |
80/3/26 80/3/17 |
1.72 (10.1) 1.72 (9.6) |
27 (5.3) 30 (6.1) |
≥ 5 ≥ 5 | ①②⑤⑧⑨ |
| Vendittoli (2020) |
HRA THA |
104, 67/37 99, 67/32 |
48.9 (9.0) 50.7 (8.4) |
81/3/26 78/2/17 |
1.71 (151–192) 1.71 (150–195) |
26.6 (4.9) 30.0 (6.8) |
≥ 15 ≥ 15 | ①⑤⑨⑩ |
| Wang (2015) |
HRA THA |
9, 32/8 23, 32/8 | 35.3 (8.8) | 12/6/14 | NR | NR |
≥ 3 ≥ 3 | ④ |
| Xiong (2014) |
HRA THA |
29, 12/17 32, 15/17 |
47.8 (18–64) 56.1 (25–88) |
1/5/23 4/13/15 | NR | NR |
≥ 0.75 ≥ 0.6 | ②④⑩⑪ |
- —Qingdao Excellent Young Medical Talents Project, Youth Talent Program of Shandong Medical Association
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes · Orthopedic Infections and Treatments
Introduction
1
Despite complications such as dislocation and periprosthetic fractures, total hip arthroplasty (THA) has always been considered the gold standard treatment for patients with end‐stage hip arthrosis, including osteoarthrosis, developmental dysplasia of the hip (DDH), and avascular necrosis of the femoral head (ANFH) [1]. Recently, advancements in materials, design, and surgical technique have led to the gradual recognition of hip resurfacing arthroplasty (HRA) as a more bone‐conserving alternative to THA, especially suitable for young and active patients with end‐stage hip arthrosis [2, 3]. The Birmingham HRA system, a classical prosthesis of HRA, has demonstrated superior 10‐year survivorship with acceptable functional outcomes and low rates of complications.
Study has been shown [4] that both THA and HRA offer excellent clinical outcomes for patients with hip arthrosis. While HRA is particularly beneficial for young people, it also provides comparable pain relief and improves hip function for other patients, restoring biomechanics characteristic of the hip and facilitating an earlier return to sports activities [5, 6]. Moreover, some researchers have found that, compared to THA, HRA allows patients to resume sports activities sooner and at higher activity levels. However, concerns [7, 8] have been raised about HRA, including a higher risk of femoral neck fractures and adverse reactions to metal debris (ARMD), among others. To date [9], the incidence of femoral neck fractures, prosthesis loosening or cracking, and ARMD is about 39%, 29%, and 6% respectively. Besides, HRA has a low fault tolerance, which makes it a technical challenge for surgeons.
Currently, there is no clear answer regarding the clinical safety and effectiveness of HRA in treating end‐stage hip arthrosis with high‐level evidence. Meanwhile, there is an undecided debate about whether THA or HRA is the better choice for patients with arthrosis. This study aims to resolve the ongoing debate between THA and HRA through a meta‐analysis and systematic review of their safety and clinical efficacy, providing evidence‐based medical evidence to guide the clinical application and promotion of HRA in treating end‐stage hip arthrosis, which is significantly helpful for surgeons to choose optimal treatments for end‐stage hip arthrosis.
Materials and Methods
2
Search Strategy
2.1
The databases of PubMed, EMBASE, Cochrane Library, and CNKI were searched by computer for the randomized controlled trials comparing HRA and THA on treating hip arthrosis, which were published between each database initiation and April 2024, without language restriction. The MeSH, such as hip arthrosis, hip arthroplasty, hip replacement, Randomized Controlled Trial, and Emtree, like hip osteoarthritis, ANFH, DDH, THA, total hip replacement, THA, hip HRA, hip resurfacing replacement, and HRA, were searched for related studies (Figure 1).
Flow chart of document retrieval process.
Inclusion and Exclusion Criteria
2.2
Inclusion Criteria
2.2.1
(i) Randomized controlled trials of patients with hip arthrosis. (ii) Patients diagnosed as hip arthrosis, including hip osteoarthrosis, traumatic arthritis, DDH, ANFH, cam hip, and so forth. (iii) Studies compared HRA and THA. (iv) Outcomes reported as follows: blood loss, operating time, revision rate, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Oxford Hip Score (OHS), Hip Harris Score (HHS), University of California at Los Angeles (UCLA) activity score, EuroQol 5D (EQ‐5D), EQ‐5D VAS, blood levels of cobalt and chromium, complications.
Exclusion Criteria
2.2.2
(i) Nonhuman studies. (ii) Review, meta‐analysis, and case report. (iii) Patients accompanied by other hip diseases or other joint dysfunctions. (iv) Without full text.
Study Selection and Data Extraction
2.3
Two researchers (X.F., Y.Z.) screened the titles and abstracts of identified studies independently. If a study met the inclusion criteria, it would be included, and the full text would be reviewed by the two researchers for further analysis independently.
Two researchers (X.F., Y.Z.) independently extracted the data of the included studies as follows: first author, year of publication, age of patients, gender ratio, diagnosis, interventions, follow‐up time, blood loss, operating time, revision rate, WOMAC, OHS, HSS, UCLA activity score, EQ‐5D, EQ‐5D VAS, blood levels of cobalt and chromium, and complications. If there were some divergences about the extracted data between the two researchers, the third researcher made a final decision.
Literature Quality Evaluation and Risk Bias Assessment
2.4
Two researchers assessed the quality and risk of bias of the included studies according to the Cochrane risk of bias assessment tool [10] and any disagreement was discussed and resolved by the third researcher.
Outcomes
2.5
In the study, the primary outcomes include revision rate, WOMAC, OHS, HSS, UCLA activity score, EQ‐5D, EQ‐5D VAS, blood levels of cobalt and chromium, and complications, and the secondary outcomes include blood loss and operating time.
Statistical Analysis
2.6
These data were analyzed using RevManv5.4 and Stata v14.0 software. Disomy and continuous variables were assessed using risk ratio (OR) and mean difference (MD) with 95% confidence intervals (CI) for weighted MD, respectively. Cochran's Q and I2 tests were used to determine heterogeneity. When the I ^2^ > 50% or the Q statistic p‐value is < 0.05, the random‐effects model is used; otherwise, the fixed‐effect model is used. Funnel charts were used to investigate occurrence bias.
Results
3
Literature Selection
3.1
A total of 225 studies were initially identified by database searching. After removing duplications (n = 33), reviews and meta‐analyses (n = 12), case reports (n = 6), non‐RCTs (n = 18), studies without detailed data (n = 17), studies without full text (n = 8), and other unrelated studies (n = 111), a total of 20 studies were included finally.
Study Characteristics
3.2
Among the included 20 studies, there were 4 studies from the Netherlands, 8 studies from Canada, 3 studies from Denmark, 3 studies from the United Kingdom, 1 study from Greece, and 3 studies from China (Table 1).
Risk of Bias
3.3
Risk of bias assessment of RCT was assessed using the Cochrane Manual for Systematic Reviews, as shown in Figure 2.
Risk of bias assessment results included in RCTs (Cochrane Manual of Systematic Reviews).
Results of the Meta‐Analysis
3.4
Revision Rate
3.4.1
Ten studies [11, 12, 13, 14, 15, 16, 17, 18, 19, 20] compared the revision rate of HRA and THA, indicating that there was no significant difference in the revision rate between HRA and THA [OR = 1.18, 95% CI = (0.72, 1.94), p = 0.52], without heterogeneity (p = 0.51, I ^2^ = 0%). The results are shown in Figure 3.
Revision rate.
WOMAC
3.4.2
Ten studies [6, 15, 19, 20, 21, 22, 23, 24, 25, 26] compared the WOMAC of HRA and THA, indicating that there was no significant difference in WOMAC between HRA and THA [MD = −0.97, 95% CI = (−2.33, 0.38), p = 0.16], without heterogeneity (p = 0.26, I ^2^ = 19%). The results are shown in Figure 4.
WOMAC.
OHS
3.4.3
Five studies [6, 12, 16, 26, 27] compared the OHS of HRA and THA, indicating that there was no significant difference in OHS between HRA and THA [MD = −0.16, 95% CI = (−1.23, 0.92), p = 0.77], without heterogeneity (p = 0.71, I ^2^ = 0%). The results are shown in Figure 5.
OHS.
HHS
3.4.4
Four studies [16, 21, 25, 28] compared the HHS of HRA and THA, indicating that there was no significant difference in HHS between HRA and THA [MD = −0.37, 95% CI = (−1.79, 1.05), p = 0.61], without heterogeneity (p = 0.58, I ^2^ = 0%). The results are shown in Figure 6.
HHS.
UCLA Activity Score
3.4.5
Nine studies [6, 15, 16, 19, 20, 23, 24, 25, 26] compared the UCLA activity score of HRA and THA, with moderate heterogeneity (p = 0.05, I ^2^ = 48%). The results showed that there was no significant difference in UCLA activity score between HRA and THA [MD = 0.34, 95% CI = (−0.04, 0.71), p = 0.08]. The results are shown in Figure 7.
UCLA activity score.
EQ‐5D
3.4.6
Three studies [12, 25, 27] compared the EQ‐5D of HRA and THA, indicating that there was no significant difference in EQ‐5D between HRA and THA [MD = −0.05, 95% CI = (−0.13, 0.02), p = 0.15], without heterogeneity (p = 0.76, I ^2^ = 0%). The results are shown in Figure 8.
EQ‐5D.
EQ‐5D VAS
3.4.7
Three studies [12, 26, 27] compared the EQ‐5D VAS of HRA and THA, indicating that there was no significant difference in EQ‐5D VAS between HRA and THA [MD = −0.01, 95% CI = (−4.62, 4.60), p = 1.00], without heterogeneity (p = 0.79, I ^2^ = 0%). The results are shown in Figure 9.
EQ‐5D VAS.
Blood Levels of Cobalt and Chromium
3.4.8
Two studies [15, 19] compared the blood levels of cobalt and chromium of HRA and THA, indicating that there was no significant difference in the blood levels of cobalt and chromium between HRA and THA [cobalt: MD = −0.84, 95% CI = (−3.04, 1.36), p = 0.45; chromium: MD = 0.11, 95% CI = (−1.04, 1.26), p = 0.85], with high heterogeneity (cobalt: p = 0.45, I ^2^ = 88%; chromium: p = 0.85, I ^2^ = 90%). The results are shown in Figures 10 and 11.
Blood levels of cobalt.
Blood levels of chromium.
Complications
3.4.9
Fifteen studies [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 22, 23, 25, 27, 29] compared the complications of HRA and THA, indicating that the complications of HRA were significantly lesser than those of THA [OR = 0.50, 95% CI = (0.39, 0.73), p < 0.00001], without heterogeneity (p = 0.74, I ^2^ = 0%). The results are shown in Figure 12.
Complications.
Blood Loss
3.4.10
Four studies [16, 20, 21, 25] compared the blood loss of HRA and THA, indicating that the blood loss of HRA was significantly less than that of THA [MD = −89.31, 95% CI = (−142.08, −36.55), p = 0.16], with low heterogeneity (p = 0.0009, I ^2^ 2 = 42%). The results are shown in Figure 13.
Blood loss.
Operating Time
3.4.11
Six studies [11, 16, 21, 22, 25, 26] compared the operating time of HRA and THA, indicating that the operating time of HRA was significantly longer than that of THA [MD = 22.39, 95% CI = (11.00, 33.78), p = 0.0001], with high heterogeneity (p < 0.00001, I ^2^ = 94%). So, subgroup analysis was performed according to the type of prosthesis, and the result showed that compared to metal‐on‐metal THA, the operating time of HRA was significantly longer with low heterogeneity (p < 0.00001, I ^2^ = 37%) and compared to metal‐onon‐poly THA, the operating time of HRA was significantly longer with high heterogeneity (p < 0.00001, I ^2^ = 98%). The results are shown in Figures 14 and 15.
Operating time.
Operation time subgroup.
Publishing Bias Test
3.5
All outcomes were tested using a funnel plot. Taking the funnel plot of complications as an example, except for the study by Hersnaes, PN 2021, which deviates from the central axis, the overall distribution is symmetrical, indicating that there is no obvious bias in the included studies. However, in the study by Hersnaes, PN 2021, 16.7% (6 cases) and 15.4% (6 cases) of patients in the THA group and the HRA group were lost to follow‐up, respectively, which may lead to incomplete data and affect the accuracy of the results (Figure 16).
Complications funnel plot.
Discussion
4
Both HRA and THA Are Safe and Reliable Operations for End‐Stage Hip Arthrosis
4.1
Revision rate and complications are important indicators for assessing the safety, reliability, and survivorship of prostheses. In this meta‐analysis, loosening, periprosthetic fractures, and unexplained pain were the main complications of HAR, while dislocation, loosening, and infection were common after THA. The incidence of complications in the HRA group is significantly lower than in the THA group (9.88% vs. 16.44%). They may be due to the characteristics of HRA. HRA preserves more proximal femur bone and maintains the structural and biomechanical characteristics of the hip, which helps prevent dislocation and improve recovery of hip function. On the other hand, the insertion of the femoral component into the femoral neck in HRA can cause local stress concentration, closely related to femoral neck fractures post‐operation [30]. Therefore, precise surgical techniques for positioning the femoral component of HRA are critical for reducing complications.
It is well known that the survivorship of prostheses is influenced by complications notably. This meta‐analysis showed that although complications associated with HRA are significantly fewer than those of THA, the revision rates for HRA and THA are similar (6.45% vs. 5.3%), which is consistent with previous studies [31, 32]. The main reason for revision in HRA and THA is loosening and dislocation, respectively. Dislocation has been considered the most common cause of revision following THA, followed by periprosthetic joint infection and loosening [33]. Factors such as age, body mass index, surgical techniques, and femoral head size have been shown to influence the incidence of dislocation post‐THA [32, 34, 35]. Many studies [36, 37] have reported that males treated with HRA exhibit higher survivorship than females. The reasons may be related to differences in femoral head size and bone mineral density, which are generally lower in females. It has been confirmed that the revision rate for HRA decreases as femoral head size increases [38]. Factors such as gender, bone mineral density, femoral head size, material and type of prosthesis, and complications are crucial in influencing the need for revision and overall survivorship after HRA. Therefore, selecting ideal candidates for THA and HRA is critical. In this meta‐analysis, most included studies used large‐head prostheses for THA as the control group, which somewhat helped to reduce the revision rate post‐surgery, despite the lack of strict inclusion criteria for HRA. This might explain why HRA shows fewer complications, yet the revision rate is comparable to THA. Optimal candidate selection for HRA could potentially lower the revision rate even further. So, it is important to choose suitable patients and prevent prosthesis loosening to reduce the revision rate of HRA, and the results also indicate that HRA is a safe and reliable treatment for hip arthroplasty. Function scores are important for assessing the clinical effects of prostheses.
Both HRA and THA Are Effective for End‐Stage Hip Arthrosis
4.2
In this meta‐analysis, we used WOMAC, HSS, OHS, UCLA activity score, EQ‐5D, and ED‐5D VAS as primary outcomes to comprehensively assess the clinical effects of HRA and THA, including locomotion, daily activities, and pain. The results showed no difference in these function scores between HRA and THA, implicating that both procedures are similarly effective in restoring joint function and relieving pain after operation. Although some studies [39, 40] reported that HRA had potential advantages over THA in promoting patients to return to sport and high‐level activities early, and some studies [41] found that HRA had better function scores than those of THA, findings show that overall outcomes for HRA are comparable to THA. Additionally, because HRA preserves more bone of the femur and maintains hip joint morphology, being helpful in restoring native hip biomechanics and improving local stress, we think patients receiving HRA treatment will achieve better long‐term effects. Therefore, future prospective RCTs should focus on the long‐term effects of HRA and THA.
Metal wear after arthroplasty and debris have a close relationship with unexplained pain and adverse local tissue reactions [42]. Some scholars [43] reported a higher blood level of cobalt and chromium in patients with HRA compared to patients with THA. However, other studies indicate that blood levels of cobalt in patients treated by HRA were significantly lower than those of patients treated by MoM‐THA, with no significant differences in chromium levels. Theoretically, patients with THA should have higher debris and metal ion blood levels due to the junction of the femoral shaft and large femoral head (trunnion/taper junction), which may produce most of the metal ions, contributing to elevated levels of cobalt and chromium [44]. However, this meta‐analysis found no difference in blood levels of cobalt and chromium between HRA and THA. This discrepancy may be attributed to the high heterogeneity among the prostheses used in the included studies, such as metal‐on‐metal THA, metal‐on‐polyethylene THA, metal‐on‐metal HRA, which leads to high heterogeneity and influences the results of blood levels of cobalt and chromium. But among the included studies, there are only two studies reporting blood levels of cobalt and chromium. So, subgroup analysis is not available for further analysis. With the development of ceramic‐on‐ceramic and metal‐on‐polyethylene HRAs [45], the blood levels of cobalt and chromium in patients with HRA have the potential to decrease further. Currently, clinical outcomes from RCTs of typical ceramic‐on‐ceramic HRA like H1 [46] and ReCerf [47] have not been published. Besides, surgical technique, especially the position of the prosthesis, is an important factor influencing prosthesis wear and debris generation. In one of our pilot experiments about the biomechanical study of the location of the HRA prosthesis, neutral and varus positions of the femoral prosthesis in HRA may increase contact pressure, causing extra wear and debris, which may increase blood levels of cobalt and chromium. So, a valgus of 10°–15° of the femoral prosthesis may be an ideal position for HRA.
HRA and THA Have Their Own Advantages and Disadvantages in Terms of Surgical Techniques
4.3
Operating time and blood loss are secondary outcomes used to evaluate surgical techniques, which are related to approaches, surgical manners, skill, and experience of surgeons, etc. This meta‐analysis showed that compared to THA, HRA required more operating time but resulted in less blood loss, consistent with a previous study [48]. Although there is a high heterogeneity between studies reporting operating time, subgroup analysis according to the type of prosthesis showed that no matter compared to metal‐on‐metal THA or metal on poly THA, the operating time of HRA was longer and the main heterogeneity is related not only to the type of prosthesis but also to factors such as surgical techniques, the experience and cooperation of the medical team, individual characteristics of patients, and so on, in our opinion. On one hand, the surgical difficulty, accuracy, and learning curve of HRA are higher than those of THA, which may increase the operating time. On the other hand, since osteotomy of the femoral neck and enlargement of the medullary cavity are not needed during HRA, this may reduce blood loss. Thus, both HRA and THA have their own advantages and disadvantages in terms of surgical techniques.
Strengths and Limitations
4.4
Although some studies [41, 48, 49] have conducted comparative analyses of HRA and THA, this meta‐analysis includes the largest number of RCTs, which are from six countries, and evaluates 11 outcomes. The results reveal that compared to THA, HRA has a similar revision rate, functional scores, and blood levels of cobalt and chromium. Additionally, HRA results in fewer complications and less blood loss, indicating its effectiveness and safety as a treatment option for hip replacement.
Obviously, there also are some limitations in the study. (i) Some results, especially operating time and blood levels of cobalt and chromium, show high heterogeneity among included studies, which cannot be resolved by subgroup analysis because there are only two papers reporting this result. This affects the reliability and accuracy of results. (ii) The follow‐up period for most included studies is short, requiring more prospective RCTs with long‐time follow‐up to analyze the long‐term effects of HRA compared to THA. (iii) No included studies have used ceramic‐on‐ceramic HRA; thus, additional prospective RCTs analyzing HRA are needed in the future.
Prospects of Clinical Application
4.5
For patients with end‐stage hip arthrosis, especially active men under 60 years of age and male manual laborers for whom squatting is often required but typically restricted after THA, HRA is a safe and effective alternative.
Conclusion
5
Both HRA and THA are safe and effective for end‐stage hip arthrosis with similar revision rates, complications incidence, and effects on functional recovery. Considering the advantages of HRA in minimally invasive procedures and preserving more bone, it is particularly suited for active men under 60 years of age and male manual laborers, for whom squatting is often required but typically restricted after THA.
Author Contributions
X.F. and Y.Z. contributed equally to this work. J.P.C. and T.Y. took part in the design of the study. X.F. and Y.Z. performed the literature survey, and drafted the manuscript. T.Z. took part in the data management implementation of the study. All authors contributed to the article and approved the submitted version.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. Okafor and A. F. Chen , “Patient Satisfaction and Total Hip Arthroplasty: A Review,” Arthroplasty 1, no. 1 (2019): 6.35240763 10.1186/s 42836-019-0007-3PMC 8787874 · doi ↗ · pubmed ↗
- 2M. A. Alagha , K. Logishetty , C. O'Hanlon , A. D. Liddle , and J. Cobb , “Three‐Dimensional Preoperative Planning Software for Hip Resurfacing Arthroplasty,” Bioengineering 10, no. 8 (2023): 939, 10.3390/bioengineering 10080939.37627824 PMC 10451941 · doi ↗ · pubmed ↗
- 3T. Al‐Jabri , M. Ridha , R. A. Mc Culloch , et al., “Hip Resurfacing Arthroplasty: Past, Present and Future,” Orthopedic Reviews 15 (2023): 77745, 10.52965/001c.77745.37405271 PMC 10317512 · doi ↗ · pubmed ↗
- 4D. G. Le Brun , T. S. Shen , P. Bovonratwet , R. Morgenstern , and E. P. Su , “Hip Resurfacing vs Total Hip Arthroplasty in Patients Younger Than 35 Years: A Comparison of Revision Rates and Patient‐Reported Outcomes,” Arthroplast Today 11 (2021): 229–233.34692960 10.1016/j.artd.2021.09.004PMC 8516816 · doi ↗ · pubmed ↗
- 5K. Rueckl , A. Liebich , U. Bechler , B. Springer , M. Rudert , and F. Boettner , “Return to Sports After Hip Resurfacing Versus Total Hip Arthroplasty: A Mid‐Term Case Control Study,” Archives of Orthopaedic and Trauma Surgery 140, no. 7 (2020): 957–962.32296965 10.1007/s 00402-020-03414-6 · doi ↗ · pubmed ↗
- 6S. Konan , C. Waugh , N. Ohly , C. P. Duncan , B. A. Masri , and D. S. Garbuz , “Mid‐Term Results of a Prospective Randomised Controlled Trial Comparing Large‐Head Metal‐on‐Metal Hip Replacement to Hip Resurfacing Using Patient‐Reported Outcome Measures and Objective Functional Task‐Based Outcomes,” Hip International 31, no. 5 (2021): 637–643.32390475 10.1177/1120700020919671 · doi ↗ · pubmed ↗
- 7J. O. Penny , K. Brixen , J. E. Varmarken , O. Ovesen , and S. Overgaard , “Changes in Bone Mineral Density of the Acetabulum, Femoral Neck and Femoral Shaft, After Hip Resurfacing and Total Hip Replacement: Two‐Year Results From a Randomised Study,” Journal of Bone and Joint Surgery. British Volume 94, no. 8 (2012): 1036–1044.22844043 10.1302/0301-620X.94B 8.28222 · doi ↗ · pubmed ↗
- 8L. Savarino , M. Cadossi , E. Chiarello , N. Baldini , and S. Giannini , “Do Ion Levels in Metal‐on‐Metal Hip Resurfacing Differ From Those in Metal‐on‐Metal THA at Long‐Term Followup?,” Clinical Orthopaedics and Related Research 471, no. 9 (2013): 2964–2971.23572350 10.1007/s 11999-013-2981-z PMC 3734417 · doi ↗ · pubmed ↗