Genotyping of Clinical Samples of Methicillin-Resistant Staphylococcus aureus Isolates in Isfahan Using Multilocus Sequence Typing (MLST)
Yasaman Ahmadi, Farnoosh Shekarchizadeh, Farnood Khajavirad, Afrouz Shekarchizadeh, Dariush Shokri

TL;DR
This study analyzed MRSA isolates in Isfahan, Iran, using genotyping to understand their genetic diversity and antibiotic resistance patterns.
Contribution
The study provides new insights into the genetic diversity and antibiotic resistance profiles of MRSA isolates in Isfahan using MLST.
Findings
MRSA isolates showed high resistance to tetracycline, ciprofloxacin, and clindamycin.
Six sequence types (STs) were identified, including ST74, ST239, ST805, ST531, ST859, and ST5.
Clonal complexes CC5, CC8, and CC30 were detected, indicating clonal spread of MRSA.
Abstract
Effective management of hospital-acquired infections caused by Staphylococcus aureus necessitates a comprehensive understanding of bacterial characteristics. The genotyping of clinical samples of methicillin-resistant S. aureus (MRSA) isolates plays a crucial role in understanding the pathogen's epidemiology, etiology, and antibiotic resistance patterns. This study investigated the genotyping and antibiotic resistance profiles of clinically isolated S. aureus strains from different hospitals in Isfahan, Iran. Sixty-three MRSA isolates were analyzed using the disc diffusion method. After DNA extraction, multilocus sequence typing (MLST) was performed using seven housekeeping genes, revealing genetic diversity. Six isolates were selected based on their resistance patterns for MLST. The most frequent isolates were detected from wounds (41.3%), and the lowest frequency was from synovial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
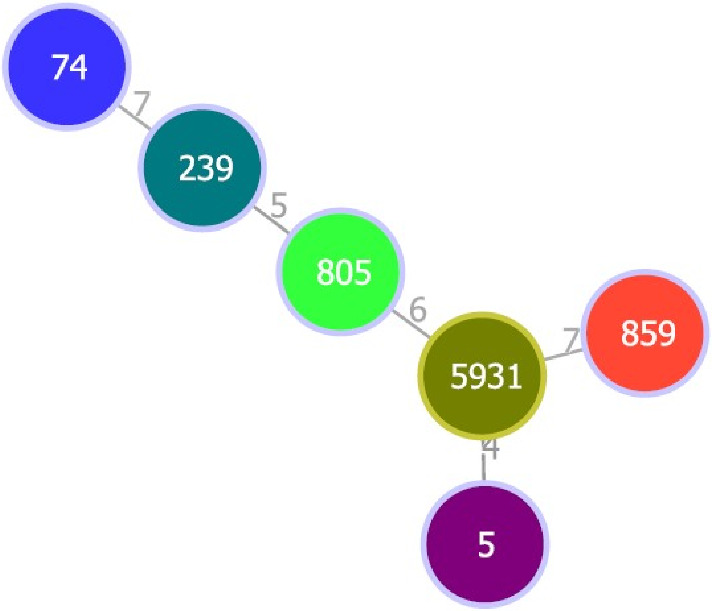 Figure 1
Figure 1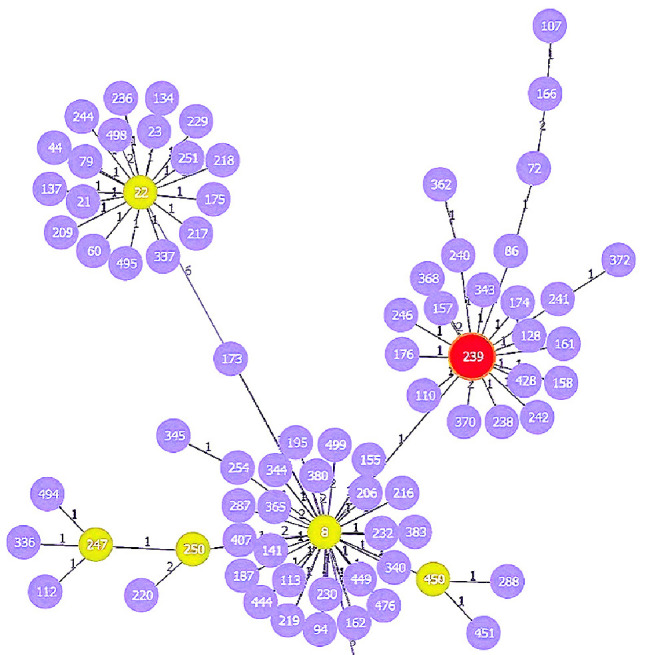 Figure 2
Figure 2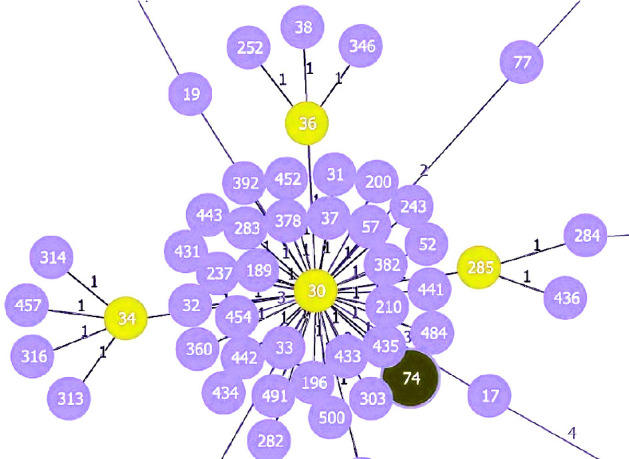 Figure 3
Figure 3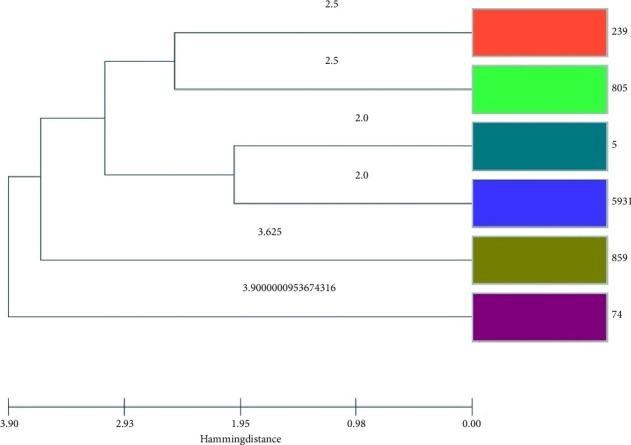 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Bacterial Identification and Susceptibility Testing · Bacterial biofilms and quorum sensing
1. Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) is a major public health concern due to its high prevalence, virulence, and resistance to multiple antibiotics, including methicillin. MRSA infections are associated with significant morbidity, mortality, and healthcare costs, particularly in clinical settings [1–3]. The pathogenicity of S. aureus is attributed to various virulence factors, such as adhesins that facilitate tissue adherence and biofilm formation on medical devices, toxins that damage host cells, and enzymes that promote tissue invasion and immune evasion. These factors, combined with its resistance to β-lactam antibiotics conferred by the mecA gene, make MRSA a formidable challenge in the treatment of nosocomial infections [4, 5].
The detection and diagnosis of MRSA rely on both phenotypic and genotypic methods. Phenotypic methods, such as antibiotic susceptibility testing and culture-based techniques, are widely used but often limited by their time-consuming nature and lower accuracy. In contrast, genotypic methods, including polymerase chain reaction (PCR), pulsed-field gel electrophoresis (PFGE), and whole-genome sequencing (WGS), offer higher specificity and speed by directly targeting resistance genes and genetic markers [6]. Among these, multilocus sequence typing (MLST) has emerged as a powerful tool for genotyping MRSA isolates. MLST involves sequencing specific housekeeping genes to assign sequence types (STs), enabling detailed epidemiological investigations and the identification of high-risk pandemic clones, such as ST239, which are associated with increased transmissibility and resistance patterns [7]. Despite advancements in diagnostic techniques, the continuous evolution of MRSA strains necessitates ongoing research to improve detection methods and understand their genetic diversity and resistance profiles [8, 9]. This study aims to genotype clinical MRSA isolates from Isfahan, Iran, using the MLST method to investigate their genetic diversity and antibiotic resistance patterns. The findings will contribute to a better understanding of MRSA epidemiology in the region and inform strategies for infection control and treatment.
2. Materials and Methods
2.1. Study Design and Samples
This cross-sectional study has been conducted on 63 MRSA isolated from different hospitalized patients in Isfahan, Iran, from 2020 to 2021. The study was confirmed by the Shahid Ashrafi Esfahani University, Isfahan, Iran. These samples were collected as part of standard patient care, and no additional samples were required.
Inclusion Criteria: Clinical samples must be confirmed as S. aureus through standard microbiological methods. Moreover, samples must be obtained from clinical settings, such as hospitals or healthcare facilities, to ensure relevance to nosocomial infection. Furthermore, isolates that do not exhibit methicillin resistance (i.e., MRSA or MSSA) were excluded and nonclinical or environmental samples were not included in this study.
The primary identification of collected isolates was applied using culture and biochemical tests such as colony morphology, Gram staining, catalase test, coagulase test, mannitol fermentation, and DNase test [8].
2.2. Antibiotic Susceptibility Profile
Using cefoxitin disks, MRSA isolates were evaluated for antibiotic susceptibility profiles based on CLSI 2022 guidelines [10]. Selected antibiotic discs were tetracycline, ciprofloxacin, clindamycin, gentamycin, doxycycline, rifampin, cotrimoxazole, linezolid, and nitrofurantoin, respectively. MRSA strains were differentiated from MSSA based on the diameter of the observed halos and strains with a diameter of no growth halo ≤ 21 mm were considered MRSA, and strains with a halo diameter ≥ 22 were considered MSSA [10, 11].
2.3. PCR for MLST
Genomic DNA was isolated from fresh colonies using a modified previously established method [18]. The purity and concentration of the extracted DNA were measured using a NanoDrop spectrophotometer (Thermo Scientific, Wilmington, USA) [12]. PCR was performed according to the Pasteur profile from https://www.pubmlst.net website to confirm S. aureus genome identification using the reference strain of ATCC 25923 running ABI 3730xl (Country) on 12.5 μL Master Mix (Amplicon, Denmark), 1.4 μL forward and reverse primers (Table 1), 10.5 μL DNA, and 2 μL extracted DNase-free-water. The amplification was carried out over 33 cycles, with the following steps: 2 cycles of 94°C for 5 min; 30 cycles of 94°C for 1 min, 52°C–56°C for 30 s, and 72°C for 2 min; and one cycle of 72°C for 2 min) [13]. Selected internal (housekeeping) genes were arc (Carbamate kinase), aroE (Shikimate dehydrogenase), glpF (Glycerol kinase), gmk (Guanylate kinase), pta (Phosphate acetyltransferase), tpi (Triosephosphate isomerase), and yqi (Acetyle coenzyme A acetyltransferase). The purity of DNAs was confirmed by NanoDrop spectrophotometer and agarose gel electrophoresis (sharp single band) [14–16].
PCR products of genes were sequenced using Sanger sequencing by Gene Fanavaran Co. (Tehran, Iran). The sequences were submitted for analysis using the Genetics Analysis 11 software (MEGA 11). The data was analyzed using the PHYLOViZ software and employing the Neighbour-Joining (NJ) method with 1000 bootstrap replicates. The goeBURST algorithm was applied, and the clonal relationships of the strains were analyzed about specific clonal complexes (CCs) present in the databases, based on the identified STs using the software https://www.phyloviz.net/ (PHYLOViZ Online) [17].
3. Results
Among 63 MRSA isolates, 41.3%, 34.9%, 11.1%, 7.9%, 3.2%, and 1.6% were isolated from the wound, urine, pulmonary, blood, abscess, and synovial samples. Based on the antibiotic resistance pattern, the highest resistance S. aureus isolates were reported against tetracycline, ciprofloxacin, clindamycin, gentamycin, doxycycline, rifampin, and cotrimoxazole as 68.3%, 44.4%, 44.4%, 27%, 23.8%, 22.2%, and 19%, respectively. However, 95.2% and 96.8% of the isolates were sensitive to linezolid and nitrofurantoin, respectively.
This study selected six isolates for MLST typing based on their resistance patterns. The MLST typing results of the selected isolates, along with the antibiotic resistance pattern, MRSA, and clinical sample type, are presented in Table 2. The STs identified one isolate of each ST74, ST239, ST805, ST5931, ST859, and ST5. The clonal relationship analysis revealed that ST5 and ST5931 belong to the same CC of CC5; ST239 belongs to CC8, ST74 belongs to CC30, and ST859 was identified as a singleton, which does not belong to any CC (Figures 1, 2, 3).
The phylogenetic tree results indicate a high genetic relatedness among the examined isolates, suggesting genetic diversity. Based on the phylogenetic tree, ST239 and ST805 shared genetic relatedness, while ST5 and ST5931 also exhibited genetic relatedness (Figure 4).
4. Discussion
4.1. Overview of MRSA and Its Clinical Impact
S. aureus can produce a wide range of infections that vary in severity, from mild skin infections to life-threatening necrotizing pneumonia. MRSA is of great concern due to its continuous and increasing occurrence of hospital-acquired infections and significant community-acquired infections. Its high prevalence in most regions has significantly increased mortality and treatment costs [13, 18]. Although efforts to control and prevent the spread of this pathogen through patients, health care staff, and environmental screening constitute a significant priority in infection control programs, relying on classification methods as important tools for describing the specific genetic characteristics of isolates can be beneficial for epidemiological investigations to trace the source and identify transmission routes of MRSA [19, 20]. These methods help trace the source and identify transmission routes of MRSA, which is essential for understanding the epidemiology, origin, and spread of MRSA infections [21].
4.2. Clinical Sample Analysis
In our study, the most frequently isolated clinical samples were from wounds (41%) and urine (35%). This finding is in line with previous studies, such as Van An et al., who reported 64.6% of MRSA isolates from wound samples [22]. These findings underscore the prevalence of MRSA in wound infections, highlighting its clinical importance [23].
4.3. Antibiotic Resistance Profile
The S. aureus isolates in this study showed the highest resistance to tetracycline, ciprofloxacin, and clindamycin. A meta-analysis by Dadashi et al. found that the rate of MRSA in Iran ranged from 36% to 50% across four periods over 16 years, with the prevalence observed in blood, wound, and respiratory tract samples [24]. The variation in MRSA prevalence among hospitals can be attributed to differences in sample sizes, sampling methods, culturing techniques, and infection control policies [25]. For example, Goudarzi et al. reported a 71% prevalence of MRSA in Tehran, with the highest resistance to penicillin, kanamycin, gentamicin, and ciprofloxacin, while all MRSA isolates remained sensitive to vancomycin, linezolid, and teicoplanin [26]. On the other hand, Hajimohammadi et al. represented that the highest levels of resistance among MRSA isolates were against erythromycin (80%) and ciprofloxacin (67%) [27]. A similar study found that over 80% of MRSA isolates were resistant to erythromycin, tetracycline, and gentamicin [28]. In a study by Zarkesh et al., the highest resistance was observed against penicillin (100%), followed by erythromycin and ciprofloxacin (92%), while the lowest resistance was observed against chloramphenicol [29]. The widespread use of these antibiotics may contribute to the emergence of resistance, which is further reinforced by the role of clinical isolates in transferring resistance to MRSA strains [30].
4.4. Molecular Characterization of MRSA Isolates
In this study, we identified six MRSA genotypes: ST74, ST239, ST805, ST5931, ST859, and ST5. ST239, in particular, is one of the most frequently detected genotypes in S. aureus isolates worldwide. Goudarzi et al. reported that ST239, along with ST15, ST182, ST22, ST585, and ST123, was predominant in Iranian hospitals [26].
Additionally, a molecular epidemiology study by Zamani et al. showed similar results, with ST22, ST239, and ST5 being the most common genotypes [31]. Our analysis demonstrated that the prevalent CC circulating in Isfahan's hospitals were CC30, CC1, CC5, and CC8. Notably, ST239, which belongs to CC8, was found in a multidrug-resistant isolate from a wound sample, remaining sensitive only to linezolid.
ST239 is the oldest pandemic clone and is considered one of the most successful MRSA lineages in many regions worldwide. This clone is recognized as the predominant clone in Iranian hospitals, European countries, the United States, and some Asian countries [32, 33]. Studies have shown that most MRSA strains in Korea and Japan are associated with ST5, while ST239 is predominant in countries such as China, Indonesia, Singapore, Sri Lanka, and Vietnam. Faraji et al. reported in their meta-analysis that the ST239-MRSA clone is prevalent among Iranian patients, suggesting that the circulation of this clone within the country may serve as a predictor of treatment failure, increased morbidity, and higher mortality rates among hospitalized individuals [9].
Havaei et al. reported that out of 83 isolated S. aureus strains from clinical samples, ST239 was the main epidemic MRSA clone (EMRSA). They also demonstrated that ST859 was only resistant to tetracycline with a negative PVL phenotype [34]. In the present study, we have identified a single isolate with the ST859 genotype from blood samples belonging to the CC88 group. This particular isolate showed resistance exclusively to tetracycline and cefoxitin. Similar to our findings, in another study to determine the characteristics of MRSA strains in Iran, it was shown that the ST859 was resistant to tetracycline and fusidic acid and known as a PVL-negative HA-MRSA clone in Iran, which is consistent with our findings [28]. In a study by Najafi Olya et al., 28 S. aureus isolates were sequenced using MLST, and the results showed that the isolates belonged to 21 unique STs and the majority of isolates belonged to CC30 [35]. Our findings genotyped ST74 from CC30 for the first time in clinical samples in Isfahan, Iran.
4.5. Clinical Implications and the Importance of Molecular Methods
The emergence of MRSA types with multidrug resistance, some of which carry important virulence genes, can seriously threaten healthcare providers and infection control personnel [36]. Given the high diversity of Staphylococcal strains, the role of the hospital environment in the formation of hospital outbreaks should be considered. Due to the importance of the spread of MRSA strains, the use of molecular methods for epidemiological investigations of these strains appears necessary [37].
4.6. Limitations
One of the primary limitations of this study is the relatively small number of isolates chosen for MLST analysis. Although this sample provides valuable initial insights into the genetic diversity of MRSA in Isfahan, it may not comprehensively reflect the broader genetic diversity of MRSA strains circulating within the region.
5. Conclusion
This study highlights the prevalence, antibiotic resistance, and genetic diversity of MRSA isolates in Isfahan, Iran. High resistance to tetracycline, ciprofloxacin, and clindamycin underscores the need for rational antibiotic use and infection control measures. The identification of CCs (e.g., CC5, CC8, CC30) suggests clonal spread, emphasizing the importance of surveillance and prevention strategies. Isolates remained highly sensitive to linezolid and nitrofurantoin, offering effective treatment options. These findings call for enhanced antimicrobial stewardship and targeted interventions to combat MRSA's clinical and economic impact, improving patient outcomes and reducing its spread in healthcare settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Algammal A. M. Hetta H. F. Elkelish A. Staphylococcus aureus Infection and Drug Resistance 2020133255326510.2147/idr.s 27273333061472 PMC 7519829 · doi ↗ · pubmed ↗
- 2Cheung G. Y. C. Bae J. S. Otto M. Pathogenicity and Virulence of Staphylococcus aureus Virulence 202112154756910.1080/21505594.2021.187868833522395 PMC 7872022 · doi ↗ · pubmed ↗
- 3Hasannejad-Bibalan M. Mojtahedi A. Biglari H. Halaji M. Sedigh Ebrahim-Saraie H. Antibacterial Activity of Tedizolid, a Novel Oxazolidinone against Methicillin-Resistant Staphylococcus aureus: A Systematic Review and Meta-Analysis Microbial Drug Resistance 20192591330133710.1089/mdr.2018.045731290721 · doi ↗ · pubmed ↗
- 4Hoveida L. Halaji M. Rostami S. Mobasherizadeh S. Biofilm-producing Ability of Staphylococcus Spp Isolated from Different Foodstuff Products Annali di Igiene: Medicina Preventiva e di Comunita 201931214014710.7416/ai.2019.22630714611 · doi ↗ · pubmed ↗
- 5Karimi M. Esfahani B. N. Halaji M. Molecular Characteristics and Antibiotic Resistance Pattern of Staphylococcus aureus Nasal Carriage in Tertiary Care Hospitals of Isfahan, Iran Infezioni in Medicina, Le 201725323424028956540 · pubmed ↗
- 6Lim K. T. Hanifah Y. A. Yusof M. Y. M. Goering R. V. Thong K. L. Temporal Changes in the Genotypes of Methicillin-Resistant Staphylococcus aureus Strains Isolated from a Tertiary Malaysian Hospital Based on MLST, Spa, and Mec-Associated Dru Typing Diagnostic Microbiology and Infectious Disease 201274210611210.1016/j.diagmicrobio.2012.05.0332-s 2.0-8486618086522770652 · doi ↗ · pubmed ↗
- 7Hajihashemi B. Abbasi A. Shokri D. Emergence of Colistin Resistant Acinetobacter Baumannii Clonal Complex 2 (CC 2) Among Hospitalized Patients in Iran Acta Microbiologica et Immunologica Hungarica 202370321321910.1556/030.2023.0205737486821 · doi ↗ · pubmed ↗
- 8Sedaghat H. Esfahani B. N. Halaji M. Genetic Diversity of Staphylococcus aureus Strains from a Teaching Hospital in Isfahan, Iran: The Emergence of MRSA ST 639- SC Cmec III and ST 343- SC Cmec III Iranian Journal of Microbiology 2018102828929997747 PMC 6039457 · pubmed ↗