Atypical Presentation of Insulinoma in a Patient With Hypoglycemia Unawareness: A Case Report
Arowa Abdelgadir, Jimmy Li Voon Chong

TL;DR
A 69-year-old man with no symptoms of low blood sugar was diagnosed with an insulinoma after a car accident revealed dangerously low glucose levels.
Contribution
This case highlights the atypical presentation of insulinoma in a patient with hypoglycemia unawareness.
Findings
The patient had abnormally high C-peptide and insulin levels during a 72-hour fast.
A CT scan identified a 1.25 cm pancreatic lesion consistent with insulinoma.
The patient underwent a successful Whipple procedure and recovered well.
Abstract
Insulinomas are uncommon tumors in the pancreas that result in the overproduction of insulin, which can cause frequent episodes of low blood sugar. While most patients present with typical symptoms such as confusion and diaphoresis, some may experience hypoglycemia unawareness. This occurs when repeated episodes of low blood glucose impair the body’s autonomic responses, making it difficult for the patient to recognize early signs of impending hypoglycemia. As a result, diagnosis can be delayed, increasing the risk of severe complications such as seizures, coma, or accidents. We present the case of a 69-year-old male diagnosed with insulinoma after a motor vehicle accident, which revealed a dangerously low blood glucose level of 2.8 mmol/L, despite the patient reporting no symptoms. Further investigations, including a supervised 72-hour fast, showed abnormally high C-peptide (1,350…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1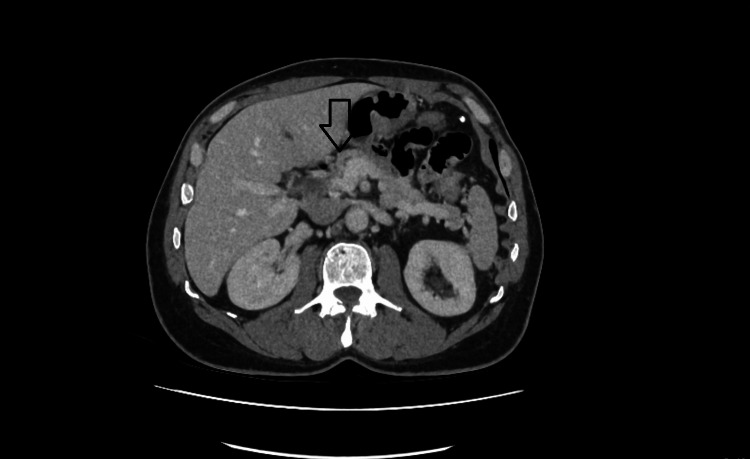 Figure 2
Figure 2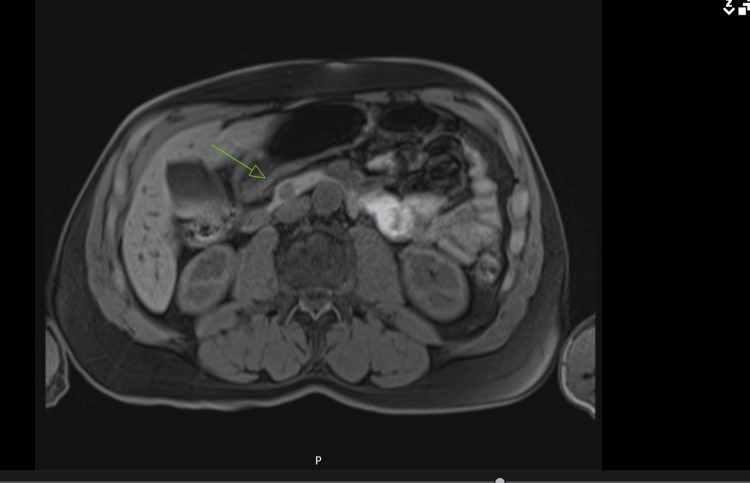 Figure 3
Figure 3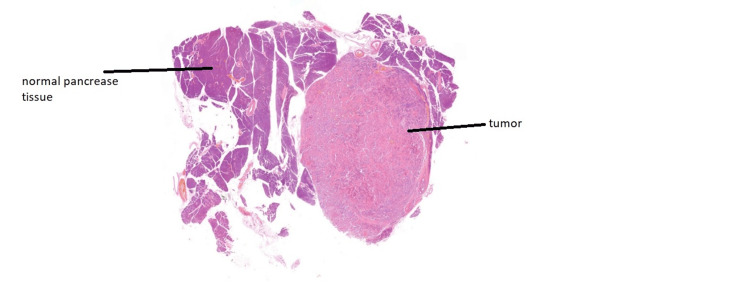 Figure 4
Figure 4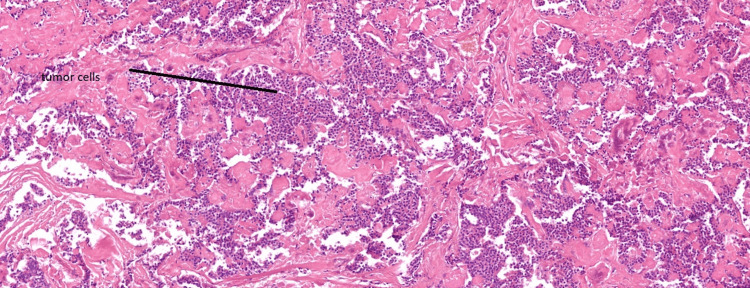 Figure 5
Figure 5| Test | Results | Reference range |
| C-reactive protein | <1 mg/L | 0-5 mg/L |
| Hemoglobin | 129 g/L | 130-180 g/L |
| White blood cell count | 7 × 10⁹/L | 4-11 × 10⁹/L |
| Platelet count | 202 × 10⁹/L | 150-500 × 10⁹/L |
| Creatinine | 71 µmol/L | 59-104 µmol/L |
| Urea | 7.3 mmol/L | 2.5-7.8 mmol/L |
| Sodium | 139 mmol/L | 133-146 mmol/L |
| Potassium | 3.6 mmol/L | 3.5-5.3 mmol/L |
| Blood glucose at the time of the incident | 2.8 mmol/L | 3.9-7.8 mmol/L |
| Interval | Cortisol level |
| 0 minutes | 299 nmol/l |
| 30 minutes | 568 nmol/l |
| Test | Results | Reference range |
| Fasting blood sugar | 2.7 mmol/L | The normal reference range for fasting blood sugar is 4.0-5.4 mmol/L. |
| C-peptide | 712 pmol/L | During a hypoglycemic episode, C-peptide >300 pmol/L is inappropriately high. |
| Insulin | 4.9 mU/L | During a hypoglycemic episode, insulin >5 mU/L is inappropriately high. |
| Test | Results | Reference range |
| Blood sugar during 72 hours of supervised fasting at 14:44; asymptomatic | 2.2 mmol/L | Reference range: 3.9-5.6 mmol/L |
| C-peptide level during low blood sugar reading in 72 hours of supervised fasting | 1,350 pmol/L | During a hypoglycemic episode, C-peptide >300 pmol/L is inappropriately high. |
| Insulin level during low blood sugar in 72 hours of supervised fasting | 14 mU/L | During a hypoglycemic episode, insulin >5 mU/L is inappropriately high. |
| HbA1c | 32 mmol/mol | Normal: 0-41 mmol/mol |
| Test | Results | Reference range |
| HbA1c | 43 mmol/mol | 0-41 mmol/mol |
| Cholesterol | 4.7 mmol/L | 0-5.2 mmol/L |
| Triglyceride | 1.24 mmol/L | 0-1.7 mmol/L |
| HDL | 1.61 mmol/L | 1.45-3 mmol/L |
| TSH | 2.49 mU/L | 0.27-4.2 mU/L |
| 25 OH vitamin D | 54 nmol/L | 50-374 nmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Neuroblastoma Research and Treatments · Lung Cancer Research Studies
Introduction
Insulinomas are rare pancreatic neuroendocrine tumors characterized by excessive insulin production, leading to a range of hypoglycemic symptoms. Most patients present with features consistent with Whipple’s triad: symptomatic hypoglycemia, documented low blood glucose, and resolution of symptoms following glucose administration. However, a subset of patients may develop hypoglycemic unawareness due to adaptive blunting of autonomic responses resulting from chronic or recurrent hypoglycemia [1].
When hypoglycemic unawareness is the presenting feature in insulinoma patients, it poses a unique diagnostic challenge, as these individuals may not recognize early warning signs such as sweating, tremors, or palpitations. This can result in delayed diagnosis and an increased risk of serious complications, including loss of consciousness, seizures, or injury from accidents [2].
Here, we report the case of a 69-year-old male diagnosed with insulinoma following a car accident, during which he was found to be hypoglycemic.
Case presentation
A 69-year-old male presented to the emergency department following a motor vehicle accident. On the day of the incident, he had consumed breakfast but skipped lunch. Pre-hospital blood glucose measurement by the ambulance crew revealed a level of 2.8 mmol/L, although the patient denied any symptoms suggestive of hypoglycemia and had no recollection of the events leading up to the accident. Notably, he has never experienced symptoms such as light-headedness, fainting, tremors, or sweating.
The patient’s medical history includes osteoarthritis of the knee and hypercholesterolemia. He was taking atorvastatin 20 mg daily and had no known drug allergies. Additionally, there is no family history of diabetes or endocrine disorders.
Initial investigations, including a brain CT scan and blood tests, yielded no significant findings aside from the documented hypoglycemia at the time of the incident (Figure 1, Table 1). Adrenal insufficiency was ruled out based on a normal response to the short Synacthen test (Table 2). Following the event, the patient notified the DVLA and refrained from driving pending further evaluation.
CT scan of the brain showing normal findings
Table 3 presents the results of the blood tests conducted while the patient’s blood glucose levels were being monitored.
The patient was referred to the endocrinology team to rule out insulinoma. He was admitted for a supervised 72-hour fast, and the results are presented in Table 4.
Additional imaging was performed to investigate the presence of a pancreatic lesion. A contrast-enhanced CT scan of the pancreas revealed a 1.25 cm hyperenhancing lesion in the proximal body, which was highly suggestive of an insulinoma (Figure 2).
CT scan of the pancreas showing a 1.25 cm enhancing lesion in the proximal body of the pancreas
He was referred for hepatobiliary surgery, and preoperative imaging included an MRI of the pancreas, which revealed a 10 mm nodule located in the inferior pancreatic head, just below the level of the ductal insertion at the ampulla (Figure 3).
MRI of the pancreas showing a 10 mm nodule located within the inferior pancreatic head, just below the level of the ductal insertion at the ampulla
The patient underwent a pylorus-preserving pancreaticoduodenectomy and cholecystectomy, collectively known as the Whipple procedure. The surgery was uncomplicated, and blood glucose levels were closely monitored throughout the perioperative period. Postoperatively, the patient was reviewed by a dietitian, and pancreatic enzyme replacement therapy was initiated to address exocrine insufficiency. Histopathological examination confirmed a grade 1, well-differentiated neuroendocrine tumor with a Ki-67 proliferation index of less than 2%, staged as pT1N0R0. The patient recovered well postoperatively and was discharged with ongoing pancreatic enzyme supplementation and regular glucose monitoring (Figure 4, Figure 5).
Histopathology slide showing normal pancreatic parenchyma adjacent to tumor tissue
Tumor cells identified on histopathological review
One month after surgery, the patient was reviewed during a follow-up appointment. He was recovering well and continued to take pancreatic enzyme supplements to support digestion, along with 40 mg of omeprazole once daily. His blood glucose levels remained stable, consistently ranging between 6 and 9 mmol/L. Several months later, he returned for a follow-up with the endocrinology team, reporting that he felt generally well. His blood sugar readings remained within normal limits, reflecting a positive outcome since his previous visit (Table 5).
The patient submitted a follow-up application to have his driving license reinstated, which was approved, and his license was reinstated.
Discussion
Insulinomas are rare tumors that develop in the pancreas. These tumors secrete excessive amounts of insulin, leading to a dangerous drop in blood sugar levels, which can result in episodes of hypoglycemia. Typically, individuals with hypoglycemia experience classic symptoms such as confusion, weakness, and sweating. However, one of the challenges associated with insulinomas is that some patients experience hypoglycemia unawareness. This condition prevents individuals from recognizing the usual bodily cues indicating low blood sugar, which increases their risk of severe hypoglycemic episodes [1,3].
Hypoglycemia unawareness occurs when individuals no longer perceive the typical warning signs of low blood sugar. Symptoms like shaking, sweating, and dizziness may be absent, even as blood glucose levels decrease to dangerous levels. This insensitivity typically develops over time due to repeated hypoglycemic episodes. As these events accumulate, they can dull the body’s natural counterregulatory responses, such as the release of adrenaline, which normally serves to alert individuals to an impending hypoglycemic crisis [1,3].
A study conducted at a single center involving 22 patients diagnosed with insulinomas found that nearly a third (seven individuals) exhibited hypoglycemia unawareness, suggesting that a significant proportion of insulinoma patients may present without the typical hypoglycemic symptoms [3].
Diagnosing insulinomas can be challenging due to several factors. One major issue is the misinterpretation of symptoms. When classic signs of hypoglycemia, like trembling and sweating, are absent, patients may instead present with nonspecific symptoms such as confusion, dizziness, or fainting. These can be mistaken for neurological or cardiovascular issues, leading to delays in proper diagnosis. Additionally, the presence of hypoglycemia unawareness can further complicate the recognition of insulinomas, as these fluctuating symptoms make it harder for healthcare providers to pinpoint the underlying cause [4,5].
Understanding the pathophysiology of hypoglycemia unawareness helps explain why these episodes occur. Several mechanisms are involved, primarily disruptions in glucose sensing in the brain, adaptations within the brain, and compromised hormonal counter-regulation. Normally, when blood sugar levels drop, hormones such as glucagon and epinephrine are released to help raise glucose levels. However, with repeated hypoglycemic episodes, the body’s response becomes impaired, leading to a cycle of unrecognized hypoglycemia. This shift increases the threshold for hormonal counter-regulation, contributing to hypoglycemia-associated autonomic failure, which characterizes hypoglycemia unawareness [6].
A significant study by Mitrakou et al. in 1993 further clarified these mechanisms. They demonstrated that patients with insulinomas typically have lower levels of counter-regulatory hormones, including plasma catecholamines, glucagon, growth hormone, and cortisol. In their study, which involved stepped hypoglycemic-clamp studies on six insulinoma patients compared to 14 age-, weight-, and sex-matched normal subjects, the researchers found substantial differences in hormone levels. Notably, the counter-regulatory hormone levels in insulinoma patients returned to normal following curative surgeries, highlighting the impact of insulinomas on hormonal regulation and suggesting that surgical intervention can restore normal physiological responses to hypoglycemia [7].
Conclusions
The connection between insulinomas and hypoglycemia unawareness presents significant diagnostic challenges, as patients may exhibit nonspecific symptoms such as confusion or fainting without the typical signs of hypoglycemia. This can result in delays in both diagnosis and treatment, ultimately increasing the risk of severe complications. Prolonged and recurrent hypoglycemia can lead to serious outcomes, including seizures, coma, or even death, particularly in the absence of the usual hypoglycemic symptoms. As demonstrated in the presented case, timely recognition of insulinomas is essential to prevent the progression of hypoglycemia unawareness and associated cognitive impairments. Early diagnosis, facilitated by biochemical testing and imaging, followed by surgical resection, is crucial in restoring normal awareness of hypoglycemic events and reducing long-term risks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mechanisms of hypoglycemia-associated autonomic failure in diabetes N Engl J Med Cryer PE 36237236920132388338110.1056/NEJ Mra 1215228 · doi ↗ · pubmed ↗
- 2Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987-2007 J Clin Endocrinol Metab Placzkowski KA Vella A Thompson GB 106910739420091914158710.1210/jc.2008-2031 · doi ↗ · pubmed ↗
- 3Phenomenon of hypoglycemia unawareness in patients with insulinoma - single center experience Neuro Endocrinol Lett Nosakova L Banovcin P Duricek M Uhrik P Bozikova J Demeter M Hyrdel R 522527422021 https://pubmed.ncbi.nlm.nih.gov/35490419/35490419 · pubmed ↗
- 4Insulinoma Surg Clin North Am Mathur A Gorden P Libutti SK 110511218920091983648710.1016/j.suc.2009.06.009PMC 3470467 · doi ↗ · pubmed ↗
- 5Insulinoma 4 2025 2025 https://www.uptodate.com/contents/insulinoma
- 6Hypoglycemia unawareness—a review on pathophysiology and clinical implications Biomedicines Hölzen L Schultes B Meyhöfer SM Meyhöfer S 3911220243839799410.3390/biomedicines 12020391 PMC 10887081 · doi ↗ · pubmed ↗
- 7Reversibility of unawareness of hypoglycemia in patients with insulinomas N Engl J Med Mitrakou A Fanelli C Veneman T 8348393291993835574110.1056/NEJM 199309163291203 · doi ↗ · pubmed ↗