Juvenile Fibroadenoma in a Prepubertal Girl With Idiopathic Precocious Puberty: A Case Report Challenging Hormonal Paradigms
Hamza Bensaghir, Asma Abbassi, Chaimae Ben Driss, Mohamed Rami, Mohamed El Amine Bouhafs

TL;DR
A rare case of juvenile fibroadenoma in a six-year-old girl with early puberty challenges existing understanding of hormonal breast tumor development in children.
Contribution
Reports a rare case of JF in a prepubertal girl, expanding the known age range for this condition.
Findings
Juvenile fibroadenoma can occur in very young children, even before puberty.
The case emphasizes the need to consider JF in the differential diagnosis of pediatric breast masses.
Literature review supports the rarity of JF in prepubertal girls.
Abstract
Juvenile fibroadenoma (JF) is a rare benign breast tumor that predominantly occurs in adolescent and young adult females. However, its occurrence in prepubertal girls is exceedingly rare and poses diagnostic and therapeutic challenges. We present a case of a six-year-old girl with a rapidly growing breast mass, ultimately diagnosed as juvenile fibroadenoma. This case highlights the importance of considering JF in the differential diagnosis of breast masses in pediatric patients, even in very young children. The clinical presentation, diagnostic workup, and management of JF are discussed, along with a review of the literature to provide insights into this rare condition.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
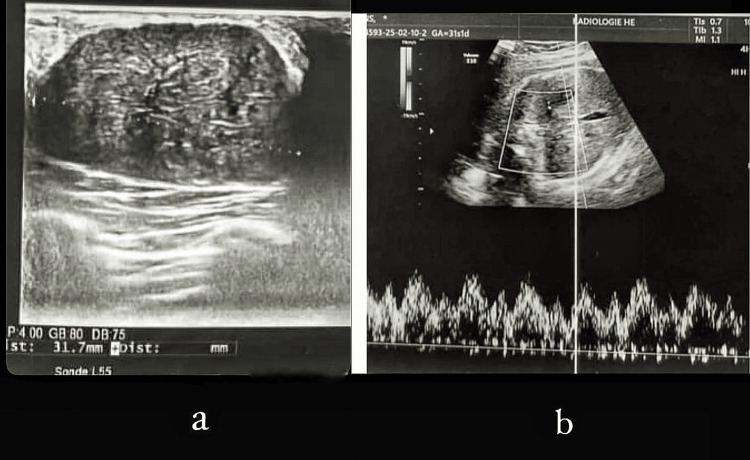 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3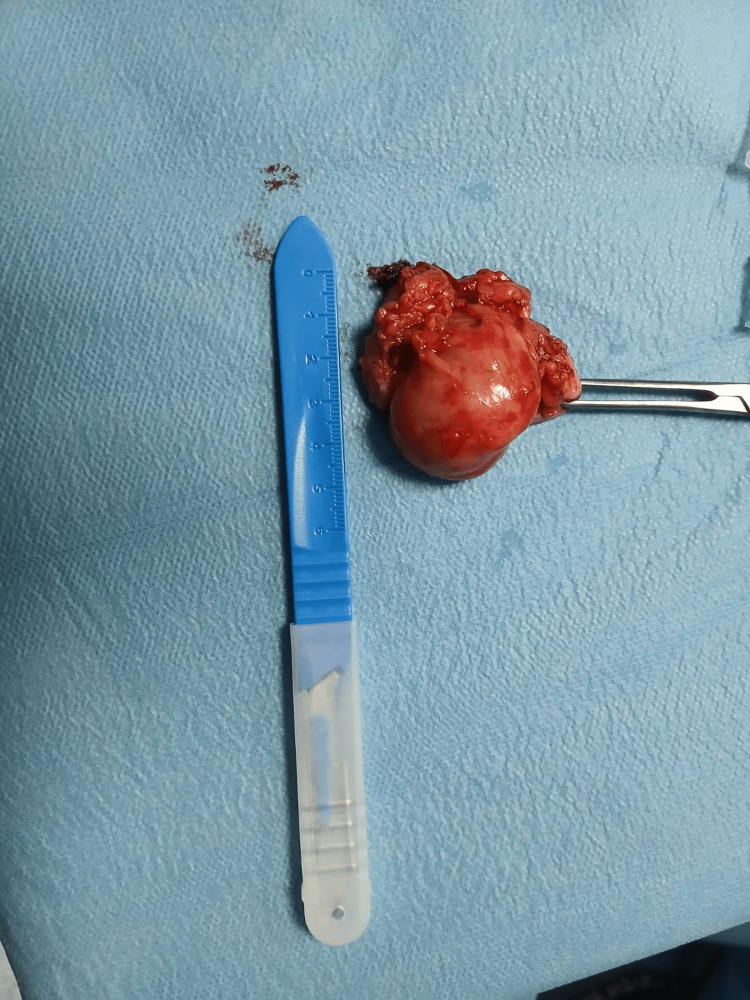 Figure 4
Figure 4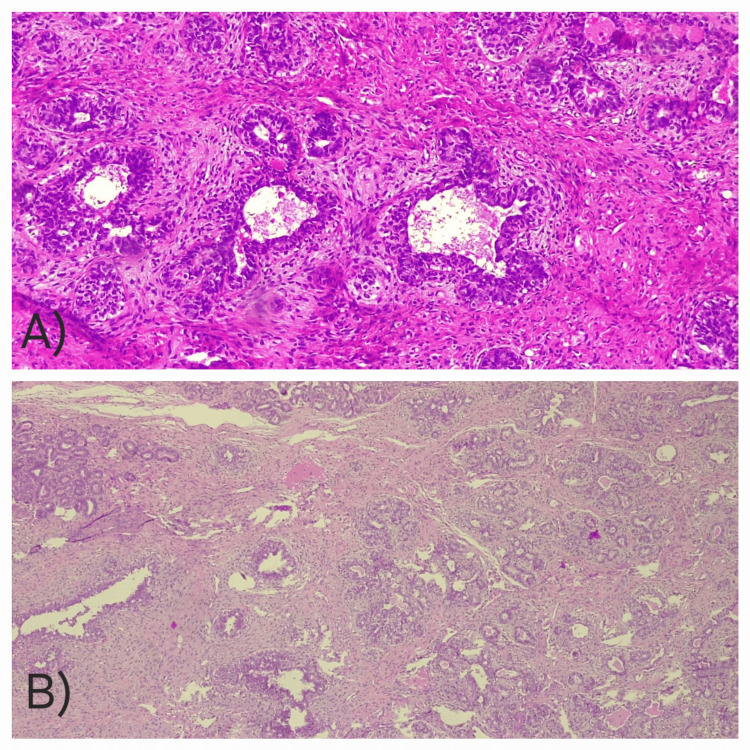 Figure 5
Figure 5| Parameter | Patient Value | Reference Range (Prepubertal) | Interpretation |
| LH | 6.57 IU/L | <0.3–4.9 IU/L | Elevated |
| FSH | 7.89 IU/L | <0.3–4.1 IU/L | Elevated |
| Estradiol | 24.1 pg/mL | <10–20 pg/mL | Mildly elevated |
| β-hCG | Normal | <2–5 IU/L (age-dependent) | Rules out germ cell tumor |
| α-Fetoprotein | Normal | <10 ng/mL | Rules out hepatoma |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · Urologic and reproductive health conditions · Breast Lesions and Carcinomas
Introduction
Juvenile fibroadenoma (JF), a distinct variant of benign fibroadenoma, primarily affects younger patients and exhibits rapid growth. Unlike conventional fibroadenomas that predominantly occur in women aged 15-35 years, JF appears more frequently in adolescents and is exceptionally rare in prepubertal children, likely due to immature breast tissue and limited hormonal stimulation. Reported incidence in children under 10 is extremely low [1]. Diagnosing JF in a six-year-old patient represents an exceptional clinical scenario that necessitates thorough evaluation to distinguish it from other pediatric breast masses, including phyllodes tumors, lipomas, and malignant lesions [2].
Effective management of pediatric JF demands a multidisciplinary strategy incorporating pediatricians, radiologists, and surgeons to achieve both accurate diagnosis and optimal treatment. This report expands the limited literature on prepubertal JF cases while offering practical guidance for clinicians.
Case presentation
Patient presentation
A six-year-old premenarchal girl presented with a rapidly enlarging left breast mass first noted by her parents four weeks earlier. The initially small lesion had progressed significantly, causing visible asymmetry. The patient reported no associated pain, nipple discharge, or breast trauma. She denied systemic symptoms, including fever or weight loss. Both personal and family histories revealed no breast pathology or malignancy.
Physical examination
Examination revealed a 4 cm firm, mobile, non-tender mass in the upper outer quadrant of the left breast. The overlying skin showed no erythema, ulceration, or peau d'orange changes. No contralateral breast masses or lymphadenopathy were detected. The remainder of the examination was normal. Tanner stage was I.
Diagnostic workup
Biological Assessment
The endocrine and tumor marker profiles are given in Table 1. No other abnormalities were noted in the laboratory findings.
Radiological Assessment
Brain and pituitary MRI was normal. Breast ultrasound (Figure 1) showed hypertrophy of both mammary glands with an oval, well-circumscribed, homogeneous, hypoechoic mass measuring 35 × 18 mm in the upper outer quadrant of the left breast.
Breast ultrasound images of the present case (a) B-mode ultrasound image showing the mass. (b) Pulsed Doppler ultrasound image showing central vascularization of the mass.
Given the patient's young age, mammography was not performed to avoid unnecessary radiation exposure.
Enhanced Endocrine Correlation
The patient's hormonal profile demonstrated elevated LH (6.57 IU/L) and FSH (7.89 IU/L) accompanied by normal estradiol levels (24.1 pg/mL), consistent with idiopathic precocious puberty. Pediatric endocrinologists confirmed the diagnosis following exclusion of CNS pathology through normal pituitary MRI findings. This hormonal pattern, involving elevated gonadotropins without a corresponding estradiol surge, is atypical and highlights possible peripheral or transient activation pathways.
Management approach
Under general anesthesia, a 2 cm transverse incision was created at the upper quadrant junction (Figure 2). A well-demarcated, mobile tumor encased in a thin fibrous capsule was identified (Figure 3). Complete excision was performed with 2 cm margins, selected due to the rapid tumor growth and concern for a potential phyllodes tumor. Care was taken to preserve the developing breast bud architecture.
Preoperative image showing the surgical approach used
Surgical images showing the stages of resection
The resected specimen measured 4.5 × 3.2 cm, exhibited characteristic whorled morphology, and was submitted for histopathological analysis (Figure 4). The margins were regular and clearly delineated.
Images showing the specimen sent to anatomopathology
Histopathological Analysis
The specimen, processed at an accredited private laboratory, demonstrated characteristic features of JF on microscopic examination (Figure 5). The epithelial component showed well-formed galactophoric ducts, while the stromal component revealed dense, homogeneous fusocellular proliferation without atypia or mitotic activity.
Histopathological features of juvenile fibroadenoma(A) High-power view showing well-formed galactophoric ducts surrounded by fusocellular stroma without atypia or mitotic activity. (B) Low-power view illustrating the overall lobulated architecture with preserved epithelial-stromal organization typical of juvenile fibroadenoma.
Clear surgical margins confirmed complete excision of this benign lesion. Immunohistochemistry (IHC) was not performed and represents a limitation.
Postoperative Course
The patient showed excellent recovery at one-, three-, and six-month follow-ups. There was no evidence of recurrence or surgical complications. Breast symmetry was restored, and both the patient and her family expressed high satisfaction with the outcome.
Discussion
JF is a rare benign breast tumor that accounts for less than 1% of all fibroadenomas [3]. It is characterized by its rapid growth and large size, often causing significant breast asymmetry and psychological distress in young patients [4]. It is exceptionally rare in prepubertal girls due to underdeveloped breast tissue and limited endogenous estrogen stimulation. Unlike typical fibroadenomas, JF tends to occur in younger age groups, with a peak incidence in adolescents aged 10 to 18 years [5]. The occurrence of JF in a six-year-old girl, as in our case, is exceptionally rare and underscores the need for awareness of this condition in prepubertal children.
This case presents a double paradox: the presence of a hormone-sensitive tumor in a patient with normal estradiol levels and biochemical signs of precocious puberty in the absence of central nervous system pathology or significant estrogen elevation. While Sklair-Levy et al. [6] associate JF with estrogen sensitivity, our findings suggest alternative pathways in prepubertal cases. The preserved tumor encapsulation and cleavage planes, unlike those seen in phyllodes tumors, further support JF’s unique biology in hormonal mosaicism. Clinically, JF presents as a firm, mobile, and painless breast mass, often with rapid enlargement over weeks to months. Imaging studies, including ultrasound and mammography, are essential for initial evaluation. On ultrasound, JF typically appears as a well-circumscribed, hypoechoic mass with homogeneous internal echoes [7]. However, definitive diagnosis requires histopathological examination, which reveals proliferative stromal and epithelial components without atypia [8].
The management of JF depends on the size of the lesion, the degree of breast asymmetry, and the patient's age. Small, asymptomatic lesions may be managed conservatively with close monitoring, while larger or rapidly growing masses often require surgical excision [9]. In pediatric patients, surgical intervention should aim to preserve breast tissue and future breast development, emphasizing the importance of a conservative approach [10].
Conclusions
JF represents a clinically significant diagnosis in pediatric breast masses, including prepubertal cases. Early detection and proper management are essential for preventing complications and achieving favorable outcomes. JF should be considered even in prepubertal girls with normal estradiol levels. This case emphasizes the importance of considering JF when evaluating breast masses in young girls and demonstrates the value of collaborative care among specialists. Additional research is necessary to elucidate the underlying mechanisms and progression of JF in this unique patient population. Pediatric breast masses, even in very young girls, may represent hormone-sensitive tumors despite normal endocrine profiles. Vigilance and interdisciplinary evaluation are key.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Phyllodes tumours Postgrad Med J Parker SJ Harries SA 4284357720011142359010.1136/pmj.77.909.428PMC 1760996 · doi ↗ · pubmed ↗
- 2Prevalence and longitudinal study of breast masses in adolescents J Adolesc Health Neinstein LS Atkinson J Diament M 277281141993834763810.1016/1054-139x(93)90174-n · doi ↗ · pubmed ↗
- 3Fibroadenomas in adolescence Curr Opin Obstet Gynecol Jayasinghe Y Simmons PS 4024062120091960603210.1097/GCO.0b 013e 32832 fa 06b · doi ↗ · pubmed ↗
- 4Management of breast fibroadenomas J Gen Intern Med Greenberg R Skornick Y Kaplan O 640645131998975452110.1046/j.1525-1497.1998.cr 188.x PMC 1497021 · doi ↗ · pubmed ↗
- 5Literature review of periclitoral cysts in the prepubertal population J Pediatr Adolesc Gynecol Nelson KL Mc Quillan SK Brain P 5585612920162723901410.1016/j.jpag.2016.05.005 · doi ↗ · pubmed ↗
- 6Incidence and management of complex fibroadenomas AJR Am J Roentgenol Sklair-Levy M Sella T Alweiss T Craciun I Libson E Mally B 21421819020081809431410.2214/AJR.07.2330 · doi ↗ · pubmed ↗
- 7Breast US in children and adolescents Radiographics García CJ Espinoza A Dinamarca V Navarro O Daneman A García H Cattani A 160516122020001111281410.1148/radiographics.20.6.g 00nv 171605 · doi ↗ · pubmed ↗
- 8Breast core needle biopsy: issues and controversies Mod Pathol Bilous M 04523201010.1038/modpathol.2010.3420436501 · doi ↗ · pubmed ↗