Beyond Atrial Fibrillation: Prioritizing Stroke Evaluation in Resource-Limited Settings
Hong Yee Lim, Yew Chung Chan, Wee Lee Chin

TL;DR
This paper discusses how to prioritize stroke evaluations in resource-limited settings by using available clinical tools to identify patients needing echocardiography.
Contribution
The paper introduces a practical approach for prioritizing echocardiography in stroke patients when resources are limited.
Findings
Clinical parameters like bedside exams and chest X-rays can guide echocardiography prioritization.
A case highlights the importance of identifying structural heart defects beyond AF in stroke evaluation.
Abstract
Atrial fibrillation (AF) accounts for the majority of cardioembolic strokes. In addition to AF screening, echocardiography is recommended to evaluate structural heart diseases including congenital anomalies. In resource-limited settings, in-hospital echocardiography for all stroke patients may not be feasible. However, careful assessment of readily available clinical parameters, such as bedside examination, electrocardiography, and chest X-ray, can offer essential clues to guide prioritization of echocardiography in selected patients and facilitate timely management. We present a case of recurrent cardioembolic stroke in a patient with AF, who was later found to have an underlying atrial septal defect, highlighting the importance of a comprehensive approach beyond AF in stroke evaluation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
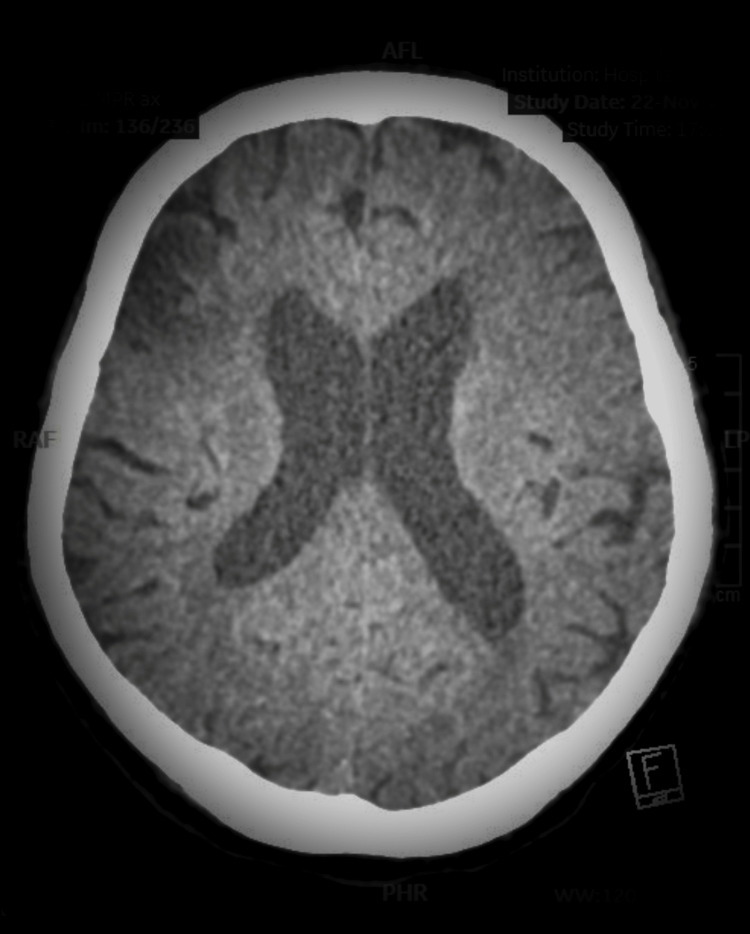 Figure 1
Figure 1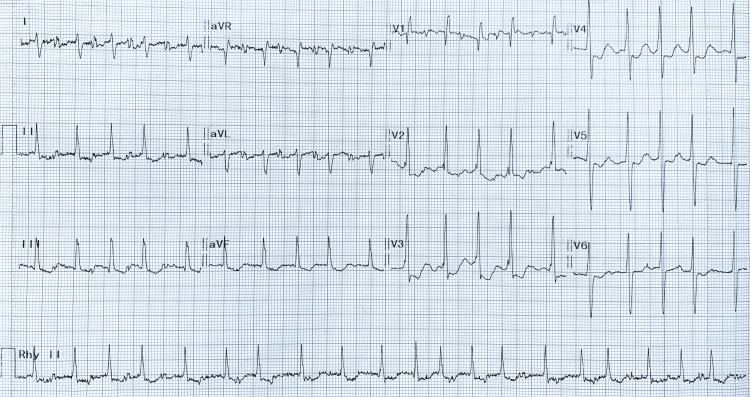 Figure 2
Figure 2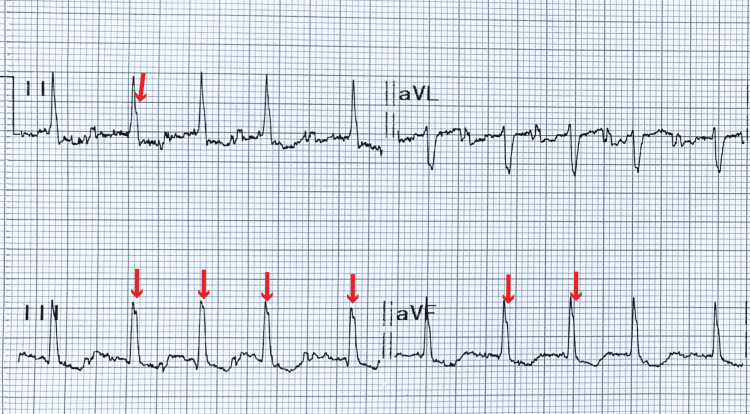 Figure 3
Figure 3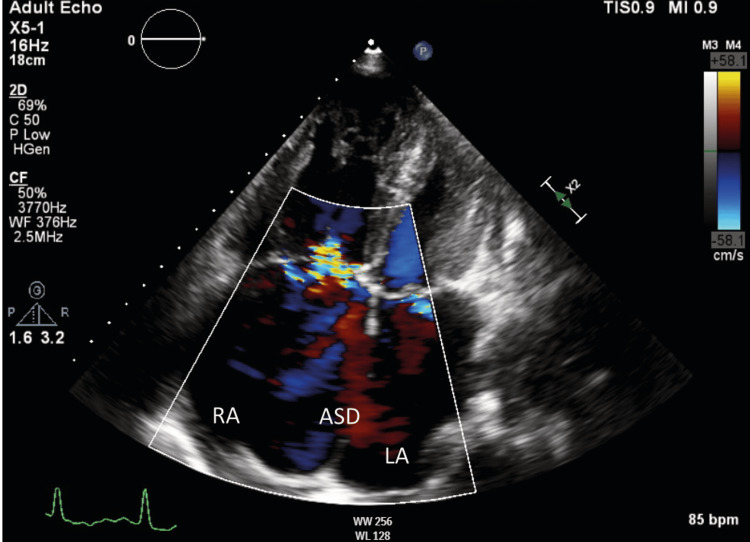 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Atrial Fibrillation Management and Outcomes · Cardiac Imaging and Diagnostics
Introduction
Atrial fibrillation (AF) is one of the most common arrhythmias worldwide and a major cause of cardioembolic stroke. The prevalence of AF increases with age, reaching a peak of 5% in people over 65 years of age, and its incidence and prevalence are increasing [1]. Standard evaluation of cardioembolic stroke typically involves screening for AF and performing echocardiography to assess for structural heart disease [2,3]. However, in resource-limited settings, echocardiography is often delayed, particularly when AF is presumed to be the sole etiology. In such contexts, clinical examinations such as electrocardiography (ECG) and chest X-ray can offer valuable insights that can help prioritize early echocardiographic assessment.
Case presentation
A 67-year-old man presented with a one-day history of right-sided weakness, facial asymmetry, and aphasia. Five months earlier, he had experienced an acute infarct involving the left temporo-occipital lobes, during which AF was detected. He was started on oral apixaban 5mg twice a day for stroke prevention. However, due to limited resources and a presumption that AF was the sole cause of the stroke, echocardiography was scheduled at a much later date. He had a 40-pack-year smoking history but had quit following his initial stroke. His past medical history was otherwise unremarkable.
On examination, he had a Glasgow Coma Scale (GCS) score of 11, with expressive aphasia, right-sided upper motor neuron facial palsy, and right-sided hemiplegia. Sensory examination was normal, and the other cranial nerves were intact. His blood pressure was 145/90 mmHg, heart rate was 80 beats per minute (bpm), and oxygen saturation was 100% on room air. Cardiovascular examination revealed an irregularly irregular pulse and a loud pulmonary component of the second heart sound (P2). There was no cardiac murmur, additional heart sound, or carotid bruit. A computed tomography (CT) of the brain revealed an acute infarct in the right middle cerebral artery territory, along with encephalomalacia in the right frontal and left temporo-occipital lobes (Figure 1).
CT of the brainCT of the brain revealed acute infarct in the right middle cerebral artery territory, along with encephalomalacia in the right frontal and left temporo-occipital lobes.CT, computed tomography
Beyond AF, ECG demonstrated right axis deviation, partial right bundle branch block (RBBB), and a subtle notch at the apex of the R wave in leads II, III and aVF (crochetage sign) - a marker suggestive of atrial septal defect (ASD), an important yet under-recognized stroke risk (Figures 2, 3). Chest X-ray showed cardiomegaly. Echocardiography subsequently confirmed the presence of an ASD with left-to-right shunt and features of pulmonary hypertension (Figure 4). The patient was referred to a cardiologist for right heart catheterization and ASD closure. He was also scheduled for an outpatient carotid artery ultrasound examination as a part of stroke screening to rule out significant carotid artery disease.
Electrocardiogram of the patientAF is noted by the absence of P waves and irregularly irregular QRS complexes. A positive QRS complex in lead aVF and negative QRS in lead I indicate right axis deviation. The presence of an rsR' pattern with a narrow QRS complex in lead V1 suggests partial RBBB. The crochetage sign is highlighted in the amplified ECG shown in Figure 3.RBBB, right bundle branch block
Amplified electrocardiogram of the inferior leadsThe crochetage sign is represented by a notching over the apex of the R wave in the inferior leads, as indicated by the red arrow. This sign is suggestive of an atrial septal defect.
Apical four-chamber echocardiographic viewThe A4C echocardiogram demonstrates the presence of an ASD with a left-to-right shunt. Both the right and left atria appear dilated.ASD, atrial septal defect; LA, left atrium; RA, right atrium
Discussion
AF is one of the most common arrhythmias worldwide and a major contributor to cardioembolic stroke. Current recommendations in cardioembolic stroke include screening for AF and performing echocardiography to assess for structural heart disease [2,3]. In many cases, the detection of AF in a stroke patient leads to a presumptive diagnosis of AF as the sole source of cardioembolic stroke. This pragmatic approach, however, often delays further cardiac evaluation. The term “lone AF” should no longer be used, as AF is often associated with a wide range of risk factors and comorbid conditions, including genetic predisposition, aging, ethnicity, gender, lifestyle-related factors, metabolic diseases, and structural heart abnormalities such as valvular defects and congenital heart diseases [2].
In addition to structural heart diseases, underlying coronary artery disease should also be considered and ruled out in patients initially presumed to have "lone AF." Recent studies indicate that up to 70% of AF patients may have coexisting coronary artery disease, which itself is an independent predictor of stroke [4-6]. This underscores the importance of comprehensive cardiovascular evaluation, particularly in high-risk individuals, rather than focusing solely on rhythm disturbances.
In developing countries with limited resources, echocardiography is not always readily available, especially in rural hospitals. As a result, when AF is detected and presumed to be the cause of cardioembolic stroke, echocardiography is often scheduled at a later time as part of routine screening. This is particularly true when the majority of stroke patients are expected to have normal echocardiographic findings [7]. Our case demonstrates the need for clinical risk stratification to prioritize urgent echocardiographic assessment in selected patients in order to prevent delayed diagnoses of structural heart diseases that require prompt treatment.
Congenital heart diseases, particularly left-to-right shunts such as ASD and ventricular septal defects, are often missed until later stages, especially in resource-limited settings. These conditions are major contributors to early onset heart failure and arrhythmias, including AF, in young adults. Early detection and targeted screening are essential to prevent irreversible complications and reduce the long-term burden of heart failure and stroke [8]. Relying solely on anticoagulant therapy in AF without addressing the underlying structural abnormalities may not adequately mitigate stroke risk. Moreover, oral anticoagulant adherence and persistence remain significant challenges in the management of AF. Multiple patient-level factors contribute to poor adherence, including fear of bleeding, low health literacy, emotional distress following diagnosis, and socioeconomic constraints. Factors such as asymptomatic or paroxysmal AF, younger age, limited treatment understanding, and competing life demands further influence medication persistence.
A systematic review of the patient’s clinical condition can provide critical insights to determine the need for in-hospital echocardiography. In addition to AF, our case highlighted important ECG findings such as the presence of crochetage sign, a notching over the R wave apex in the inferior leads, which, in the presence of right axis deviation and partial RBBB, raises strong suspicion of ASD [9,10]. Additional findings that suggested the need for early echocardiography include a loud P2 on auscultation and cardiomegaly evident on chest X-ray. This case emphasizes the importance of a thorough ECG analysis beyond merely confirming AF in stroke patients. When combined with physical signs, this approach supports the prioritization of echocardiography even at the initial stroke presentation. This is crucial as cardioembolic strokes in ASD may occur due to paradoxical embolism or as a result of AF, and both anticoagulation therapy and ASD closure are required to adequately mitigate stroke risk in this patient population.
Conclusions
While AF remains the major contributor to cardioembolic stroke, careful evaluation of ECG findings and other clinical parameters can help prioritize echocardiographic assessment, particularly for detecting structural heart diseases including acyanotic congenital heart diseases such as ASD. This approach is especially valuable in resource-limited settings, where early echocardiography may not be feasible in all patients with stroke, and prioritization is essential to ensure timely diagnosis and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute cardioembolic cerebral infarction: answers to clinical questions Curr Cardiol Rev Arboix A Alio J 5467820122284581610.2174/157340312801215791 PMC 3394108 · doi ↗ · pubmed ↗
- 22024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J Van Gelder IC Rienstra M Bunting KV 331434144520243921072310.1093/eurheartj/ehae 176 · doi ↗ · pubmed ↗
- 3The role of echocardiography screening at the stroke unit Front Neurol Pagola J Pagola C Juega J González-Alujas T Alvarez-Sabin J Molina CA 10031120203301366310.3389/fneur.2020.01003 PMC 7516041 · doi ↗ · pubmed ↗
- 4Assessment of coronary artery disease in non-valvular atrial fibrillation: is this light at the end of the tunnel?Vasc Health Risk Manag Batta A Hatwal J Sharma YP 493499202024 https://www.tandfonline.com/doi/full/10.2147/VHRM.S 484638#abstract 3953424610.2147/VHRM.S 484638 PMC 11556227 · doi ↗ · pubmed ↗
- 5Atrial fibrillation and coronary artery disease: an integrative review focusing on therapeutic implications of this relationship World J Cardiol Batta A Hatwal J Batta A Verma S Sharma YP 229243152023 https://www.wjgnet.com/1949-8462/full/v 15/i 5/229.htm 3727437610.4330/wjc.v 15.i 5.229PMC 10237004 · doi ↗ · pubmed ↗
- 6The relationship between atrial fibrillation and coronary artery disease: understanding common denominators Trends Cardiovasc Med Mekhael M Marrouche N Hajjar AH Donnellan E 91983420243618202210.1016/j.tcm.2022.09.006 · doi ↗ · pubmed ↗
- 7Value of routine echocardiography in the management of stroke CMAJ Fralick M Goldberg N Rohailla S 09191201910.1503/cmaj.190111 PMC 668248131387955 · doi ↗ · pubmed ↗
- 8Emerging risk factors for heart failure in younger populations: A growing public health concern World J Cardiol Parizad R Batta A Hatwal J Taban-Sadeghi M Mohan B 104717172025 https://www.wjgnet.com/1949-8462/full/v 17/i 4/104717.htm 4030862210.4330/wjc.v 17.i 4.104717 PMC 12038706 · doi ↗ · pubmed ↗