Reversible Acute Kidney Injury Due to Suspected Paraneoplastic Glomerulopathy in Malignant Ovarian Germ Cell Tumor: A Case Report
Nozomi Furuzono, Shinichi Togami, Honami Oi, Aoi Iwao, Hiroaki Kobayashi

TL;DR
A young woman with ovarian cancer had reversible kidney failure linked to a rare tumor-related kidney condition, which improved after surgery.
Contribution
This is the first report linking paraneoplastic glomerulopathy to malignant ovarian germ cell tumors.
Findings
Renal function improved rapidly after tumor resection, suggesting a paraneoplastic cause.
The patient's kidney failure was not due to obstruction, infection, or electrolyte issues.
Complete remission was achieved with chemotherapy following successful surgery.
Abstract
Acute kidney injury (AKI) in patients with malignancies is typically caused by urinary obstruction, tumor infiltration, or metabolic derangements. However, paraneoplastic glomerulopathy remains an uncommon and under-recognized etiology of AKI, particularly in gynecologic malignancies. We describe the case of a 21-year-old woman who presented with abdominal distension and a large pelvic mass. Imaging and laboratory data suggested an International Federation of Gynecology and Obstetrics stage IIIC malignant ovarian germ cell tumor. Renal dysfunction was evident on admission and did not respond to intensive fluid resuscitation. The patient showed no signs of hydronephrosis, infection, or electrolyte abnormalities. Despite supportive care, her renal function continued to deteriorate, and continuous hemodiafiltration (CHDF) was initiated. Due to progressive clinical decline, emergency tumor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
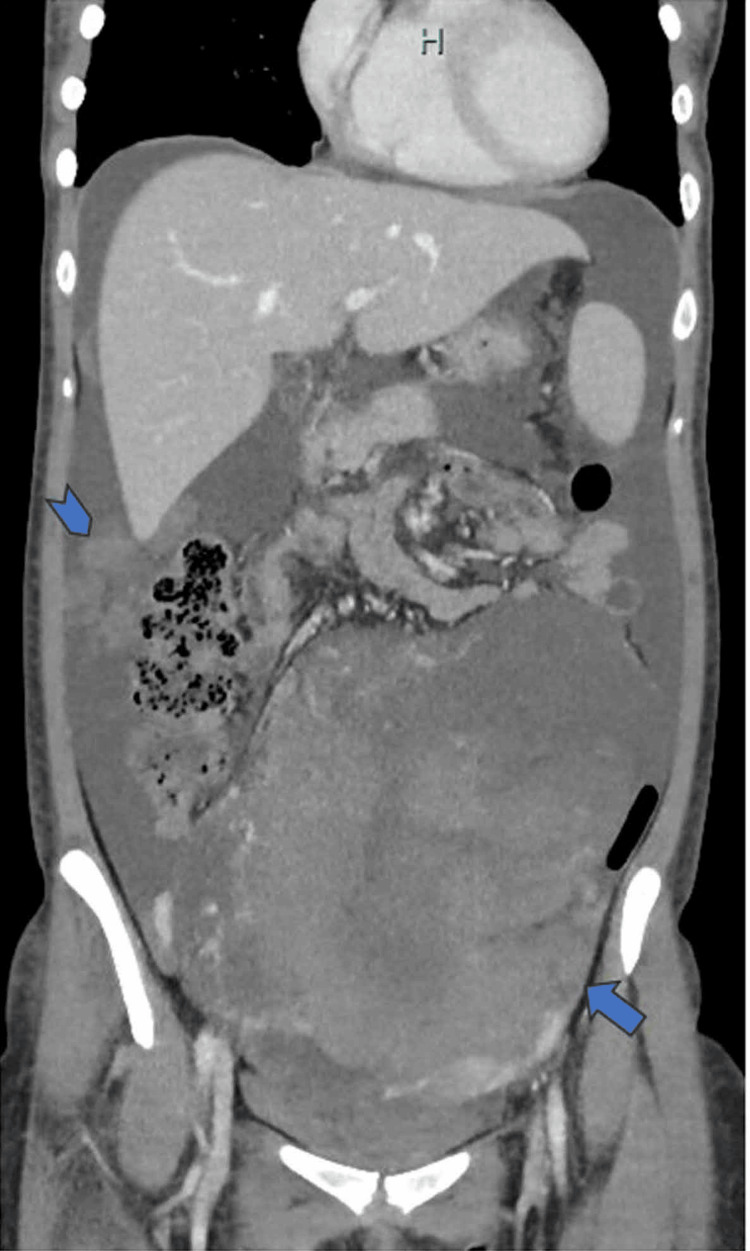 Figure 1
Figure 1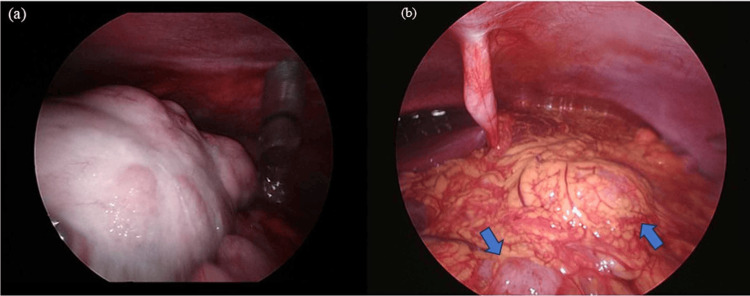 Figure 2
Figure 2 Figure 3
Figure 3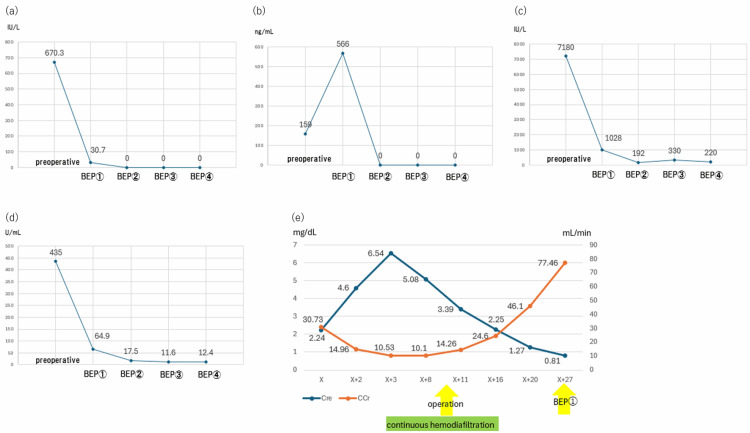 Figure 4
Figure 4| Parameter | Result | Reference Range |
| White blood cell count | 8,560/μL | 3,300-8,600/μL |
| Hemoglobin | 10.1 g/dL | 11.6-14.8 g/dL |
| Platelet count | 427,000/μL | 158,000-348,000/μL |
| Serum creatinine | 2.24 mg/dL | 0.46-0.79 mg/dL |
| Creatinine clearance | 30.73 mL/min | >60 mL/min |
| Alpha-fetoprotein (AFP) | 159 ng/mL | <7 ng/mL |
| Cancer antigen 125 (CA125) | 435 U/mL | <35 U/mL |
| Carbohydrate antigen 19-9 (CA19-9) | 4.0 U/mL | <37 U/mL |
| Human chorionic gonadotropin (hCG) | 670.3 IU/L | <5 IU/L (non-pregnant women) |
| Lactate dehydrogenase (LDH) | 7,095 IU/L | 124-222 IU/L |
| Category | Mechanism |
| Direct mechanisms of the tumor | Direct infiltration of tumor cells into the kidney |
| Urinary tract obstruction | |
| Compression of the renal vasculature | |
| Indirect mechanisms of the tumor | Renal calcification |
| Cast nephropathy due to multiple myeloma | |
| Immunological abnormalities (paraneoplastic glomerulopathy) | |
| Electrolyte imbalance | |
| Disseminated intravascular coagulation | |
| Urinary tract infections | |
| Treatment induced | Tumor lysis syndrome |
| Drug-induced nephrotoxicity | |
| Radiation nephropathy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMuscle and Compartmental Disorders · Methemoglobinemia and Tumor Lysis Syndrome · Chemotherapy-induced organ toxicity mitigation
Introduction
Malignant ovarian germ cell tumors account for 3.2% of all malignant ovarian tumors, with mixed germ cell tumors being extremely rare, comprising only 0.3% of cases. Histologically, malignant ovarian germ cell tumors include dysgerminoma, yolk sac tumor, and immature teratoma, with mixed germ cell tumors encountered less frequently than the others [1]. One of the most notable characteristics of malignant ovarian germ cell tumors is their predominance in adolescents and young adults, typically occurring in their 10s and 20s. Due to their high sensitivity to chemotherapy, fertility-sparing surgery is often considered, regardless of the disease stage [2].
Acute kidney injury (AKI) associated with malignancy is typically caused by tumor-related urinary tract obstruction, direct tumor invasion of the kidneys, or humoral hypercalcemia of malignancy - resulting from tumor-derived parathyroid hormone-related protein, activated vitamin D, or extensive bone metastases leading to hypercalcemia [3]. However, there have been no prior reports of AKI complicating malignant ovarian germ cell tumors without these underlying mechanisms.
Herein, we describe the rare case of a patient with a mixed malignant ovarian germ cell tumor, complicated by AKI, which progressed to the point of requiring emergency renal replacement therapy (RRT).
Case presentation
A 21-year-old woman (gravida 0) presented with a chief complaint of abdominal distention to a local gynecological clinic. Transabdominal ultrasonography revealed a pelvic tumor extending up to the umbilicus. Subsequently, she was referred to our department for further evaluation and treatment. Upon arrival, she was ambulatory, with a performance status of 0. The physical examination revealed a palpable tumor in the left lower abdomen, extending to one fingerbreadth above the umbilicus. The uterus was mobile and approximately the size of a hen’s egg, while the left adnexa was not palpable. On speculum examination, the cervix was deviated to the left, suggesting uterine displacement due to a right adnexal tumor.
Transvaginal ultrasonography revealed a solid pelvic mass with areas of high and low echogenicity, along with ascites and a 5-cm nodule in the pouch of Douglas, suggesting peritoneal dissemination. Laboratory test results indicated mild anemia (white blood cell count: 8,560/μL; hemoglobin level: 10.1 g/dL; platelet count: 427,000/μL) and impaired renal function (serum creatinine (Cre) level: 2.24 mg/dL; creatinine clearance (CCr): 30.73 mL/min). Tumor markers were significantly elevated: alpha-fetoprotein (AFP) level: 159 ng/mL (normal <10 ng/mL); cancer antigen 125 (CA125) level: 435 U/mL; carbohydrate antigen 19-9 level: 4.0 U/mL; and human chorionic gonadotropin (hCG) level: 670.3 IU/L (normal <5 IU/L in non-pregnant women). The level of lactate dehydrogenase (LDH), a tumor marker associated with dysgerminoma, was markedly elevated at 7,095 IU/L (Table 1).
Pelvic contrast-enhanced magnetic resonance imaging demonstrated a 24-cm solid tumor originating from the right adnexa, with low signal intensity on T1-weighted images and slightly high signal intensity on T2-weighted images, along with diffusion restriction. The uterus was displaced to the left by the tumor. Computed tomography showed no distant metastasis but revealed para-aortic lymphadenopathy, with a short axis of 10 mm, suggesting lymph node metastasis. Additionally, peritoneal dissemination, with nodules exceeding 2 cm in diameter, was identified in the upper abdomen (Figure 1).
Computed tomography imagingA 24-cm right ovarian mass extending from the pelvic cavity to the upper abdomen is observed (arrow), along with scattered intraperitoneal dissemination (arrowhead).
We observed no hydronephrosis or urinary tract involvement. On the basis of these findings, we diagnosed the patient with suspected stage IIIC malignant ovarian germ cell tumor [4].
Due to the presence of renal dysfunction, urgent treatment was deemed necessary, and the patient was admitted two days after her initial visit to our department (day X+2). Upon admission, blood chemistry test results revealed a rapid progression of renal dysfunction over the preceding two days, with Cre increasing to 4.60 mg/dL and CCr decreasing to 14.96 mL/min. The patient’s urine output was 300 mL/day, which was below 0.5 mL/kg/hour. Thus, we diagnosed AKI on the basis of the Kidney Disease: Improving Global Outcomes (KDIGO) diagnostic criteria [5], which the patient met. No significant electrolyte abnormalities, including serum calcium levels, were observed, and transabdominal ultrasonography did not reveal bilateral hydronephrosis. Given the presence of abdominal distention, poor oral intake following a recent coronavirus disease infection, and a fractional excretion of sodium of 0.57% (below 1%), prerenal azotemia was suspected.
Despite consultation with nephrology and aggressive fluid resuscitation, renal function deteriorated further on the following day (day X+3), with the Cre level increasing to 6.54 mg/dL and CCr decreasing to 10.53 mL/min. The patient met the clinical indications for emergency RRT according to the KDIGO guidelines [5]. She was unresponsive to diuretics, with a 3-kg weight gain over two days. Although serum potassium levels remained within normal limits and no uremic symptoms were noted, arterial blood gas analysis revealed severe metabolic acidosis (pH: 7.345; bicarbonate level: 18.6 mmol/L; base excess: -7.3 mmol/L). Consequently, emergency RRT was initiated, and the patient was transferred to the intensive care unit, where continuous hemodiafiltration (CHDF) was initiated and led to improvements in fluid overload and metabolic acidosis. However, urine output remained minimal, and renal function showed no significant improvement.
The etiology and pathophysiology of AKI remained unclear in this patient, but given the need for rapid intervention to improve the patient’s overall condition, diagnostic laparoscopic surgery was performed on day X+10 (Figure 2).
Findings of diagnostic laparoscopy(a) The tumor is occupying the pelvic cavity; (b) multiple peritoneal implants are observed on the omentum (arrows).
Intraoperative assessment using the Predictive Index [6] yielded a score of 4, indicating feasibility for primary debulking surgery. Thus, the procedure was converted to an open laparotomy, and right salpingo-oophorectomy, partial omentectomy, appendectomy, and resection of the disseminated nodules were performed. Macroscopic residual tumors included a 5-cm nodule in the pouch of Douglas and a 1-cm nodule around the ileocecal region, with a calculated reduction rate of 98%. The pathological diagnosis was mixed malignant ovarian germ cell tumor, consisting of undifferentiated germ cell tumor (95%) and yolk sac tumor (5%) (Figure 3).
Histopathological findings of the resected specimen(a) Low-power view reveals nests with trabecular arrangements of polygonal tumor cells (hematoxylin and eosin staining); (b) low-power view reveals partial positivity of alpha-fetoprotein staining.
Remarkably, by postoperative day 5 (day X+15), urine output had increased to >30 mL/hour, the Cre level improved to 2.8 mg/dL, and CCr increased to 24.59 mL/min, meeting the KDIGO criteria for discontinuation of CHDF [5]. While early initiation of postoperative bleomycin, etoposide, and cisplatin (BEP) as chemotherapy was considered, dose reduction (50%-75%) is recommended when CCr is <30 mL/min [7]. Given the need to administer full-dose chemotherapy, BEP initiation was postponed for one week to allow for further renal recovery.
By postoperative day 17 (day X+27), renal function had normalized (Cre level: 0.81 mg/dL; CCr: 88.49 mL/min), allowing for the initiation of BEP chemotherapy without dose reduction. Serial monitoring of tumor markers (AFP, CA125, hCG, and LDH) following BEP chemotherapy is shown in Figures 4a-4e.
Trends in tumor markers and renal function(a) AFP (alpha-fetoprotein); (b) CA125 (cancer antigen 125); (c) LDH (lactate dehydrogenase); (d) hCG (human chorionic gonadotropin); (e) Renal functionBEP, bleomycin, etoposide, and cisplatin
By the start of the third cycle of BEP, all tumor marker values had normalized, and imaging studies performed after completing four cycles of BEP confirmed a complete response. The patient has been followed up on an outpatient basis, without any evidence of recurrence to date.
Discussion
The present case underscores the importance of considering tumor-related factors as potential contributors to AKI, even in the absence of common mechanisms such as urinary obstruction or hypercalcemia. Our patient initially had normal renal function but developed severe AKI that necessitated emergency RRT. Despite adequate fluid resuscitation, renal function continued to deteriorate, but it improved rapidly following tumor debulking surgery. Possible causes of AKI in malignant ovarian germ cell tumors include tumor lysis syndrome associated with treatment initiation [8] or drug-induced nephrotoxicity during BEP chemotherapy [7]. However, these mechanisms are treatment-related and were not applicable in this case. Causes of renal impairment associated with malignant tumors [9], including hematologic malignancies, are summarized in Table 2.
Paraneoplastic glomerulopathy, a form of glomerular injury triggered by various hormones, growth factors, cytokines, and tumor-specific antigens produced by tumor cells, can occur independently of tumor invasion or metastasis [10]. Paraneoplastic glomerulopathy is most commonly associated with membranous nephropathy in solid tumors, particularly gastric, esophageal, renal, and lung cancers [11], and renal dysfunction secondary to paraneoplastic glomerulopathy typically improves or resolves with effective treatment of the primary malignancy. The diagnostic criteria for paraneoplastic glomerulopathy include: (1) exclusion of other apparent causes of renal dysfunction, (2) onset of renal dysfunction after the development of malignancy, and (3) improvement of renal function following successful treatment of the malignancy, with recurrence or worsening of renal dysfunction correlating with disease progression. Notably, renal biopsy is not mandatory for diagnosis [10].
Although there have been no previous reports of paraneoplastic glomerulopathy associated with malignant ovarian germ cell tumors [11], this diagnosis was strongly suspected in the present patient based on the following factors: (1) the absence of tumor infiltration or metastasis affecting the urinary tract, (2) lack of response to adequate fluid management, (3) absence of electrolyte disturbances, and (4) rapid improvement of renal function following tumor debulking surgery, which effectively treated the underlying malignancy. These findings suggest that paraneoplastic glomerulopathy was the most likely mechanism underlying the AKI observed in this patient.
BEP chemotherapy remains the standard adjuvant chemotherapy for malignant ovarian germ cell tumors and has demonstrated excellent treatment outcomes [1]. Maintaining the intensity of BEP chemotherapy, including adherence to the recommended dosage and treatment schedule, is crucial for achieving optimal outcomes [1]. Attempts to substitute cisplatin with carboplatin, due to concerns about nephrotoxicity and gastrointestinal toxicity in the treatment of testicular germ cell tumors, result in poorer prognoses [12]. In this case, the decision to delay BEP chemotherapy by a few days after surgery allowed for sufficient renal recovery, enabling the administration of full-dose BEP chemotherapy without the need for dose reduction. This approach contributed significantly to the successful completion of the treatment regimen and to the favorable outcome observed in this patient.
Although the diagnostic value of high-resolution ultrasound images and color Doppler evaluation is widely recognized in the characterization of adnexal masses, we regret that high-quality grayscale and Doppler images were not available for this particular case. This limitation precluded the inclusion of representative imaging figures in the manuscript.
Nonetheless, the lesion’s features were assessed based on standard sonographic parameters during the examination. In clinical practice, risk stratification tools such as the Risk of Malignancy Index (RMI), the International Ovarian Tumor Analysis (IOTA) Simple Rules, and the ADNEX (Assessment of Different NEoplasias in the adneXa) model are often employed to support the diagnosis. These models integrate factors such as menopausal status, CA-125 level, and specific ultrasound characteristics to estimate the probability of malignancy. Although these models were not formally applied in this case, their potential utility in similar clinical scenarios should be emphasized. Future studies should aim to incorporate such standardized models to enhance objectivity and reproducibility in the evaluation of adnexal lesions.
Moreover, this case report provides a detailed account of the patient's clinical presentation, physical findings, and initial sonographic features to support diagnostic reasoning in similar cases. It is important to note, however, that accurate interpretation of adnexal ultrasound findings requires experienced and well-trained personnel, as subtle features may be overlooked by less experienced examiners.
In many clinical settings, ultrasound serves as the first-line and often the most critical diagnostic tool. When interpreted correctly, it may offer sufficient information to reach a presumptive diagnosis without the need for additional imaging. This is particularly relevant in resource-limited environments, where access to advanced imaging modalities may be restricted. Acknowledging this, we emphasize the need for both comprehensive clinical evaluation and adequate operator training to ensure reliable interpretation and appropriate management.
Finally, recent advances in artificial intelligence (AI) have opened new possibilities in medical imaging analysis, including the evaluation of adnexal lesions. Although AI-based diagnostic tools were not applied in the present case, future studies may benefit from incorporating such technologies to improve diagnostic accuracy and reduce interpretation time. Integrating AI into ultrasound assessment may also help minimize inter-observer variability and support clinical decision-making, particularly in settings with limited access to expert operators.
Conclusions
Prompt treatment of the primary malignancy in this patient led to the restoration of renal function, allowing for the successful administration of full-dose BEP chemotherapy without dose reduction. The ability to maintain the full treatment intensity of BEP chemotherapy was a critical factor contributing to the achievement of complete remission in this patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NCCN Guidelines® insights: ovarian cancer, version 3.2022 J Natl Compr Canc Netw Armstrong DK Alvarez RD Backes FJ 9729802020223607539310.6004/jnccn.2022.0047 · doi ↗ · pubmed ↗
- 2Fertility-sparing surgery should be the standard treatment in patients with malignant ovarian germ cell tumors J Adolesc Young Adult Oncol Turkmen O Karalok A Basaran D 270276620172808553510.1089/jayao.2016.0086 · doi ↗ · pubmed ↗
- 3Acute kidney injury in patients with cancer N Engl J Med Rosner MH Perazella MA 1770178137620172846786710.1056/NEJ Mra 1613984 · doi ↗ · pubmed ↗
- 42014 FIGO staging for ovarian, fallopian tube and peritoneal cancer Gynecol Oncol Mutch DG Prat J 40140413320142487839110.1016/j.ygyno.2014.04.013 · doi ↗ · pubmed ↗
- 5KDIGO clinical practice guidelines for acute kidney injury Nephron Clin Pract Khwaja A 084120201210.1159/00033978922890468 · doi ↗ · pubmed ↗
- 6A laparoscopy-based score to predict surgical outcome in patients with advanced ovarian carcinoma: a pilot study Ann Surg Oncol Fagotti A Ferrandina G Fanfani F Ercoli A Lorusso D Rossi M Scambia G 115611611320061679144710.1245/ASO.2006.08.021 · doi ↗ · pubmed ↗
- 7Indications and dosing of anticancer drug therapy in patients with impaired kidney function, from clinical practice guidelines for the management of kidney injury during anticancer drug therapy 2022 Int J Clin Oncol Nishiyama H Inoue T Koizumi Y 129813142820233757219810.1007/s 10147-023-02377-z · doi ↗ · pubmed ↗
- 8Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus Br J Haematol Cairo MS Coiffier B Reiter A Younes A 57858614920102033146510.1111/j.1365-2141.2010.08143.x · doi ↗ · pubmed ↗