Transcatheter Intervention for Multiple Valve Diseases in a Patient With Cardiogenic Shock
Sixiong Hu, Gaxue Jiang, Lu Zhang, Tian rui Liu, Yong ling Wa, Ming Bai, Jizhe XU

TL;DR
This paper discusses a case of a patient with severe heart valve issues and how transcatheter interventions can help treat such complex conditions.
Contribution
The paper presents a novel case study on transcatheter intervention for multiple valve diseases in a high-risk patient.
Findings
Combined aortic and mitral regurgitation can cause severe hemodynamic disorders.
Transcatheter valve intervention offers a promising treatment for high-risk valve disease patients.
Abstract
The combination of aortic regurgitation (AR) and mitral regurgitation (MR) is not uncommon in clinical practice, and varying degrees of regurgitation often result in severe hemodynamic disorders. Combined AR and MR often present a therapeutic challenge given the difficulty of attributing symptoms to 1 or both valves and the lack of reliable clinical trial data to guide clinical decision making. Transcatheter valve intervention has brought a new light to patients with high-risk valve disease. We report a patient with high-risk multiple valve disease and discuss the hemodynamic characteristics of the diagnostic process as well as therapeutic ideas.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
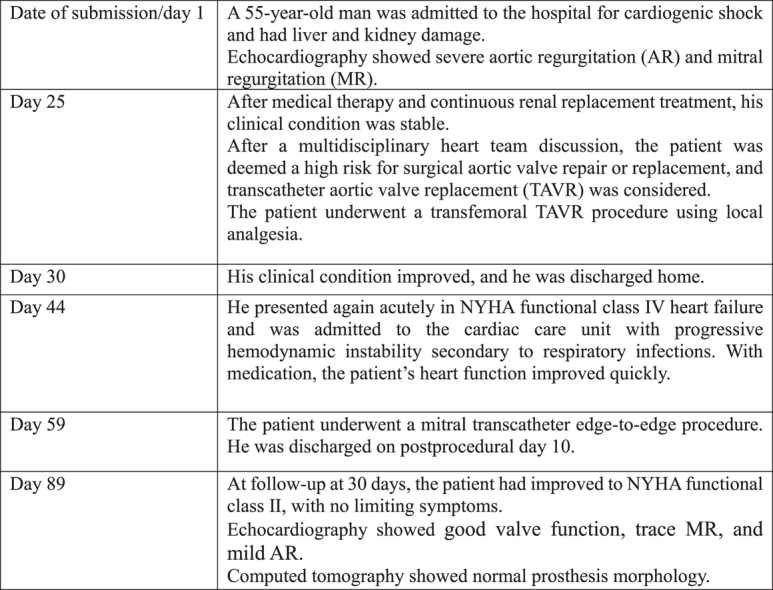 Figure 1
Figure 1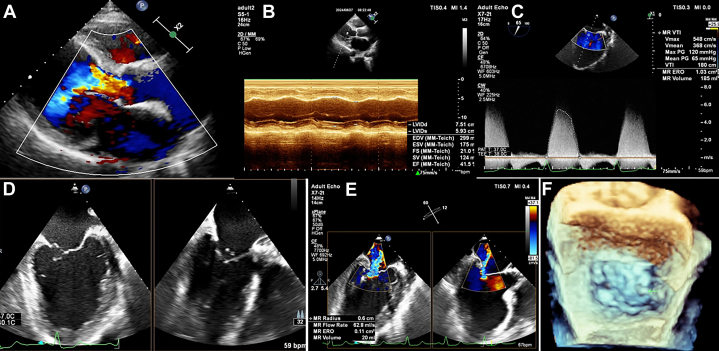 Figure 2
Figure 2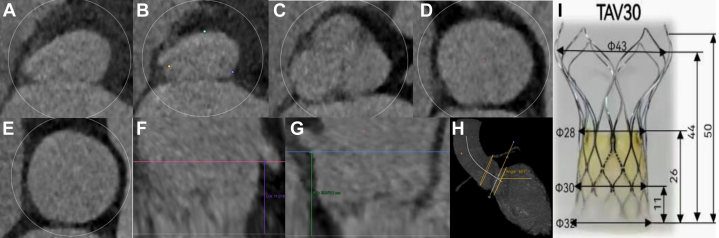 Figure 3
Figure 3 Figure 4
Figure 4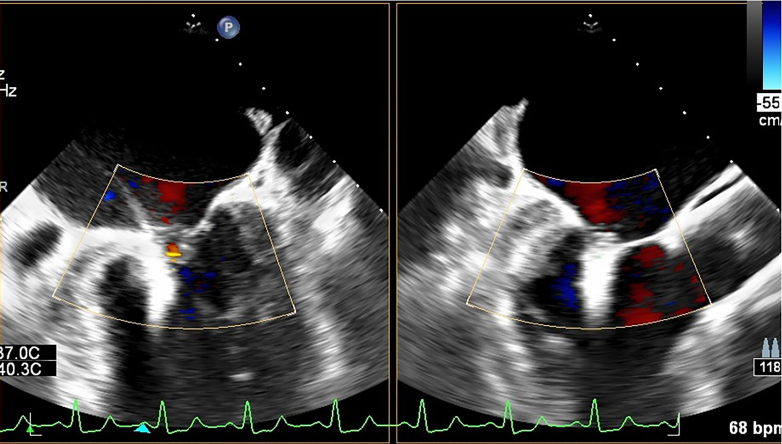 Figure 5
Figure 5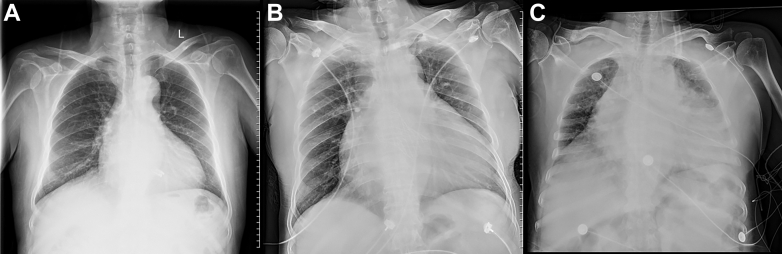 Figure 6
Figure 6 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Cardiac Structural Anomalies and Repair
History of Presentation
A 55-year-old male patient was admitted to the hospital for dyspnea lasting 1 year and worsening for 1 month. The patient first presented with symptoms of dyspnea in September 2023, with ultrasound indications of dilation of the ascending aorta combined with severe aortic regurgitation (AR), as well as mitral valve prolapse combined with severe mitral regurgitation (MR). The patient refused surgery and received medication. The patient developed severe heart failure following respiratory infection, combined with liver and kidney damage, in July 2024. On examination, his blood pressure was 92/50 mm Hg, his heart rate was 160 beats/min (atrial flutter), and he had orthopnea, cyanosis of the extremities, severe pitting edema of both lower extremities, and moist rales in both lungs. He had a heaving apex impulse, a severe diastolic murmur observed at the aortic valve area, and a systolic murmur observed at the mitral valve area.Take-Home Messages
- •We need to rationalize the characteristics of valvular diseases and the sequential order of disease from hemodynamic disorders.
- •The fundamentals of treatment need to be given in terms of the relationship between hemodynamic correction and prognosis, as well as considerations of surgical accessibility.
Past Medical History
The patient had a 10-year history of hypertension.
Differential Diagnosis
The differential diagnosis included ruptured aortic sinus aneurysm, rheumatic valvular disease, and degenerative valvular disease.
Investigations
The patient presented with cardiogenic shock and was dependent on vasoconstrictor drugs. The patient required volume management, cardiac function support, and effective infection control. We used continuous renal replacement therapy to remove excess fluid and toxins. With the combination of these measures, the patient’s condition initially improved.
Transthoracic echocardiography (TTE) showed moderate concentric left ventricular (LV) dilation with an LV ejection fraction (LVEF) of 41%. There was severe AR with left coronary cusp prolapse. According to the Carpentier classification of AR, type III was the main mechanism of AR in this patient.1 Transesophageal echocardiography (TEE) showed prolapse of the mitral valve in P3 with rupture of the tendon chords combined with a dilated mitral annulus (Figures 1A to 1F).Figure 1. Evaluation of Aortic Regurgitation and MR by Thoracic and Transesophageal Echocardiography(A) Aortic regurgitation; vena contracta = 12 mm. (B) Left ventricular dilation; left ventricular ejection fraction = 41.5%. (C) Mitral regurgitation (MR); effective regurgitant orifice (ERO) area = 1.03 cm^2^. (D) Biplane images in bicommissural and left ventricular outflow tract views by transesophageal echocardiography. (E) Effective regurgitant orifice area and proximal isovelocity surface area radius. (F) 3-dimensional en face surgery view; the arrow shows ruptured chordae tendineae. 2D = 2-dimensional; bpm = beats/min; EDV = end-diastolic volume; EF = ejection fraction; ESV = end-systolic volume; LVIDd = left ventricular internal diameter in diastole; LVIDs = left ventricular internal diameter in systole; max = maximum; PG = pressure gradient; SV = stroke volume; V = velocity; VTI = velocity time integral.
Surgery is preferred for multiple valve diseases according to guideline recommendations.2^,^3 The patient had a Society of Thoracic Surgeons predicted risk of mortality score of 9.5%, which is considered a high surgical risk. Guidelines suggest that in patients with surgical high-risk AR, transcatheter aortic valve replacement (TAVR) may be considered under conditions where the aortic root anatomy is suitable.2 MR often has complex mechanisms. AR caused LV enlargement, and chordae rupture caused degenerative MR. Therefore, the mechanisms of this MR comprised Carpentier types I, II, and IIIb. AR was improved after TAVR, the preload was reduced, and the FMR could be improved. We think maybe the mitral valve therapy strategy could be changed after TAVR and guideline-directed medical therapy (GDMT).
Management
Considering the patient’s basal status for tolerance of the procedure and anesthesia time, we chose to achieve TAVR using local anesthesia and prepared extracorporeal membrane oxygenation as a safeguard. Mitral transcatheter edge-to-edge repair (TEER) requires the use of general anesthesia, so we decide to separate the 2 procedures. Our anatomical analysis of the aortic root showed mild thickening of the valve, no calcification, and a low risk of coronary obstruction. All 3 levels can be anchored according to the diameters of the level of the LV outflow tract, the annulus, and the ascending aorta, all of which provided reliable anchoring force, and the valve leaflets were slightly thickened, which provided a positive impact on the success of transfemoral TAVR.4^,^5 We decide to use an off-label self-expanding valve and evaluate the degree of oversizing rate (Figures 2A to 2I). We first performed coronary angiography, which showed 2 severe stenoses in the right coronary artery and implanted 2 stents. The right femoral artery of the patient was chosen for TAVR as the primary vascular access with a 22-F-long introducer. A 30-mm VitaFlow self-expanding valve (MicroPort) was advanced through a 22-F sheath. Moving the pigtail catheter into the noncoronary cusp and adopting a cusp-overlapping strategy, the catheter was positioned accurately. The initial positioning of the implant should make the ring of the tip capsule about 2 mm below the annulus. Rapid pacing was performed at the rate of 160 to 180 beats/min to lower the systolic blood pressure below 60 mm Hg. Homogeneous velocity released the valve by an electric delivery system at the two-thirds of the valve overall. Evaluation by radiography and TTE focused on the valve position, anchoring, morphology, and paravalvular leakage. Rapid pacing at the rate of 140 beats/min released the valve stably. Angiography showed a correct position with mild perivalvular leakage according to the Selles grading criteria (Figures 3A to 3F, Video 1). TEE showed that the bioprosthesis was in a normal position, with an LVEF of 42%, and an aortic valve flow velocity of 1.6 m/s. Electrocardiography suggested atrial fibrillation combined with left bundle branch block. The patient was discharged from the hospital on the fourth day after TAVR.Figure 2. Evaluation of the Aortic Root and the Degree of Oversizing Rate by Computed Tomography Angiography(A) The left ventricular outflow tract diameter (area) was 26.7 mm; compression ratio: (323−26.7) / 32 = 16.6%. (B) The annular diameter (area) was 26.2 mm; compression ratio: (30−26.2) / 30 = 12.7%. (C) The sinus of Valsalva diameter (area) was 33.9 mm. (D) The sinotubular junction diameter (area) was 33.3 mm. (E) The ascending aorta diameter (area) was 37 mm; compression ratio: (43−37) / 43 = 14%. (F) The left coronary artery height was 19.2 mm. (G) The right coronary artery height was 19.1 mm. (H) The maximal intensity projection showed any calcification in the aortic root. (I) Radial line of the VitaFlow. TAV = transcatheter aortic valve.Figure 3. Procedure of Coronary Angiography, Percutaneous Coronary Intervention, and Transcatheter Aortic Valve Replacement Using Local AnesthesiaSevere coronary local stenosis in the right coronary artery. (B) Post stents implanted in the right coronary artery. (C) Aortic root angiography by power injection. (D) Initial positioning of the valve. (E) Confirmation of valve implantation position through angiography. (F) Valve fully released and trace paravalvular leak checked by angiography.
The patient’s cardiac function deteriorated again 2 weeks later as a result of a respiratory infection. The patient was in sinus rhythm, which suggested that the TAVR was effective. Subsequently, we used the DragonFly transcatheter mitral TEER system to help this patient. The first clip, 0612 (width by length), locked posterolateral commissure to A3P3, and the second clip, 0612, locked A3 to P2P3. MR was reduced from 4+ to 1+ by TEE evaluation (Figure 4, Video 2, Video 3, Video 4, Video 5), and the transvalvular pressure difference was 4 mm Hg. Table 1 is a list of equipment used for the procedures in this case.Figure 4. Final Result of Transcatheter Edge-to-Edge Repair by Transesophageal EchocardiographyThe first clip sized by 06 (width) and 12 (length) was implanted in posterior commissural leaflet P3. And another clip sized by 06 (width) and 12 (length) was implanted in A3 to P3 from shoulder to shoulder. Transesophageal echocardiography showed mitral regurgitation reduced from 4+ to trace. bpm = beats/min.Table 1. List of Equipment Used in This CaseTranscatheter aortic valve replacement Imaging
-
•Transthoracic echocardiography (TTE) (GE Medical System)
-
○M5Sc TTE probe Access
-
•Ultrasound machine (GE Medical System)
-
•Micropuncture needle and wire
-
•0.035-inch J wire and 7-F sheath
-
•2 ProGlide (Abbott Vascular)
-
•Lunderquist Extra Stiff Wire Guide (Cook)
-
•22-F sheath (APT Medical) Transcatheter aortic valve replacement device
-
•VitaFlow transcatheter aortic valve system (MicroPort) Mitral transcatheter edge-to-edge repair Imaging
-
•Transesophageal echocardiography (TEE) (Philips Healthcare)
-
○0.035-inch X7 TEE probe Access
-
•Ultrasound machine (Philips Healthcare)
-
•Micropuncture needle and wire
-
•0.035-inch J wire and 7-F sheath
-
•1 ProGlide (Abbott Vascular)
-
•Supra stiff guide wire (Boston Scientific)
-
•18-F Cook sheath (Cook Medical) Transseptal puncture
-
•Transseptal needle (Boston Scientific)
-
•SL-1 sheath (Abbott Vascular)
-
•0.032-inch wire
-
•Supra stiff guide wire (Boston Scientific) Mitral transcatheter edge-to-edge repair device
-
•DragonFly system (steerable guide catheter [SGC] and clip delivery system [CDS]) (Valgen Medtech) Visual SummaryTimeline of TreatmentDate of submission/day 1A 55-year-old man was admitted to the hospital for cardiogenic shock and had liver and kidney damage.Echocardiography showed severe aortic regurgitation (AR) and mitral regurgitation (MR).Day 25After medical therapy and continuous renal replacement treatment, his clinical condition was stable.After a multidisciplinary heart team discussion, the patient was deemed a high risk for surgical aortic valve repair or replacement, and transcatheter aortic valve replacement (TAVR) was considered.The patient underwent a transfemoral TAVR procedure using local analgesia.Day 30His clinical condition improved, and he was discharged home.Day 44He presented again acutely in NYHA functional class IV heart failure and was admitted to the cardiac care unit with progressive hemodynamic instability secondary to respiratory infections. With medication, the patient’s heart function improved quickly.Day 59The patient underwent a mitral transcatheter edge-to-edge procedure. He was discharged on postprocedural day 10.Day 89At follow-up at 30 days, the patient had improved to NYHA functional class Ⅱ, with no limiting symptoms.Echocardiography showed good valve function, trace MR, and mild AR.Computed tomography showed normal prosthesis morphology.
Outcome and Follow-Up
Postoperative treatment included angiotensin receptor-neprilysin inhibitor, beta-blockers, sodium-dependent glucose transporters 2, and mineralocorticoid receptor antagonist agents. Because of stent implantation in the patient’s coronary arteries and the comorbidity of atrial fibrillation, with a CHA_2_DS_2-_VA score of 3 and a HAS-BLED score of 3, the patient was indicated for anticoagulant therapy but had a high risk of bleeding and needed to be closely monitored for bleeding. After discharge, the patient was treated with clopidogrel and dabigatran. TTE showed good valve function and trace MR and mild AR at 1 month after intervention. Chest radiography showed that the heart shadow gradually shrank, and pulmonary congestion improved (Figures 5A to 5C). Computed tomography showed normal prosthesis morphology and no leaflet thrombus at 3-month follow-up (Figures 6A to 6E). The patient’s NYHA functional classification improved from class IV to class II.Figure 5. Evolution of Chest Radiography From First Admission to Recovery(A) Chest radiograph showed that the heart/chest ratio was 0.63 at discharge and recovery. (B) The heart/chest ratio was 0.81 at the second admission to the cardiac care unit. (C) The heart/chest ratio was 0.9 at the first admission to the cardiac care unit with cardiogenic shock and severe pulmonary edema.Figure 6. Computed Tomography Scan at 3-Month Follow-UpMorphology of the prosthesis and the relationship with surrounding tissues. (A) Left ventricular outflow tract. (B) Annulus. (C) 10 mm above the annulus. (D) Corolla. (E) The overall of the morphology.
Discussion
An observational study from China found that regurgitation accounts for the majority of valve heart diseases, and the most common dual dysfunction is aortic valve combined with mitral valve.6 Among these diseases, it is not uncommon to see patients with low-grade valve regurgitation, and when both valves have severe regurgitation at the same time, severe hemodynamic disorders can lead to decreased cardiac function, surgical risk becomes high, and the prognosis is poor. The diagnosis and treatment of heart valve disease have improved dramatically in recent years, but data to guide clinical decision making in patients with multiple valve disease remain limited.3
Transcatheter valve intervention has become an effective protocol for saving high-risk patients. TAVR in patients with AR is difficult and requires strict anatomical conditions for the valve annulus, and preoperative analysis of the aortic root anatomy is particularly important. For MR, there are often complex mechanisms, which determine the strategy of mitral TEER. A domestic study on TAVR in treating combined AR and MR found that severe AR manifests with varying degrees of functional MR (FMR), which can be improved after TAVR.7 The MATTERHORN (A Multicenter, Randomized, Controlled Study to Assess Mitral vAlve reconsTrucTion for advancEd Insufficiency of Functional or iscHemic ORigiN) study also confirmed that in patients with FMR, mitral TEER is not inferior to surgery.8 Therefore, mitral TEER is feasible for different mechanisms of MR, for which the mechanism and degree of MR will improve after downstream TAVR and GDMT treatment, thus leading to a rational surgical strategy. Patients with a high risk of combined valve disease have rapid progression and high surgical risk, and intraoperative remedial extracorporeal circulation surgery is extremely risky in the event of acute complications such as valve displacement and aortic dissection. Therefore, for this group of patients, we need to do a good job in the assessment of surgical risk, the choice of surgical methods, the timing of surgery, as well as strict follow-up.
Conclusions
Severe AR and MR combined with acute heart failure are characterized by high surgical risk and mortality, and initial correction of the heart failure state consists of medication, reasonable imaging, and assessment of the degree of surgical tolerance. Transcatheter intervention can be performed in stepwise fashion to correct the hemodynamic disorder and improve the patient’s clinical status and prognosis.
Funding Support and Author Disclosures
This work was supported by the Provincial Science and Technology Plan (funding number: 23YFWA0012). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Addetia K.Lang R.Roadmap to the mechanisms of aortic regurgitation on echocardiography JACC Case Rep 2102020158915943431702510.1016/j.jaccas.2020.07.012PMC 8302201 · doi ↗ · pubmed ↗
- 2Otto C.M.Nishimura R.A.Bonow R.O.2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol 7742021 e 25e 1973334258610.1016/j.jacc.2020.11.018 · doi ↗ · pubmed ↗
- 3Vahanian A.Beyersdorf F.Praz F.2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J 4372021561632
- 4Yao J.Lu Z.N.Modine T.Evaluation of the safety and efficacy of a novel Anatomical Classification and Dual Anchoring Theory to Optimize the TAVR Strategy for Pure Severe Aortic Regurgitation (AURORA): a prospective cohort study BMC Cardiovasc Disord 22120224453624369310.1186/s 12872-022-02883-4PMC 9571459 · doi ↗ · pubmed ↗
- 5Gao X.Zhang J.Kong X.Transcatheter aortic valve replacement in patients with pure native aortic regurgitation:results from a multicenter registry study Cardiol Discov 42202413414110.1097/CD 9.0000000000000101 · doi ↗
- 6Yang Y.Wang Z.Chen Z.Current status and etiology of valvular heart disease in China: a population-based survey BMC Cardiovasc Disord 21120213393425670010.1186/s 12872-021-02154-8PMC 8276378 · doi ↗ · pubmed ↗
- 7Cao J.Zheng X.Chen M.Liu X.Liu J.Zhang G.Effectiveness and feasibility of transcatheter aortic valve replacement in treating combined aortic and mitral regurgitation: a retrospective observational study J Thorac Dis 1552023276327683732407110.21037/jtd-23-505PMC 10267927 · doi ↗ · pubmed ↗
- 8Baldus S.Doenst T.Pfister R.Transcatheter repair versus mitral-valve surgery for secondary mitral regurgitation N Engl J Med 391192024178717983921609310.1056/NEJ Moa 2408739 · doi ↗ · pubmed ↗