A Case of Atrial Standstill Misdiagnosed as Atrial Fibrillation: Diagnostic Insights and Clinical Implications
Zhengbo Wu, Yang Wu, Yang Liu, Jiqiang Hu

TL;DR
This case report describes a rare heart condition, atrial standstill, initially mistaken for atrial fibrillation, highlighting the importance of accurate diagnosis for proper treatment.
Contribution
The paper presents a novel case of atrial standstill misdiagnosed as atrial fibrillation and emphasizes the need for advanced diagnostic methods.
Findings
Atrial standstill was confirmed through electrophysiological testing after initial misdiagnosis as atrial fibrillation.
The case highlights the diagnostic challenges of atrial standstill and the importance of comprehensive evaluation.
Long-term atrial fibrillation may contribute to the development of acquired atrial standstill.
Abstract
Atrial standstill (AS), a rare and diagnostically challenging cardiac disorder with total absence of atrial electrical and mechanical activity, often presents variably, mimicking atrial fibrillation (AF) in electrocardiogram (ECG). This report details a case of AS initially misdiagnosed as AF. A 65-year-old Chinese female had 5-year intermittent palpitations. Prehospital ECG showed paroxysmal AF, and echocardiogram showed a giant atrium. A single-chamber pacemaker (ventricular pacing, ventricular sensing, inhibited) was implanted 6 months ago due to long ventricular intervals. During this hospitalization, AS was confirmed using electrophysiological examination, altering the treatment approach and prognosis. AS is complex and overlooked. Early recognition and proper management are crucial. Accurate diagnosis via echocardiogram and electrophysiological testing is vital for at-risk…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
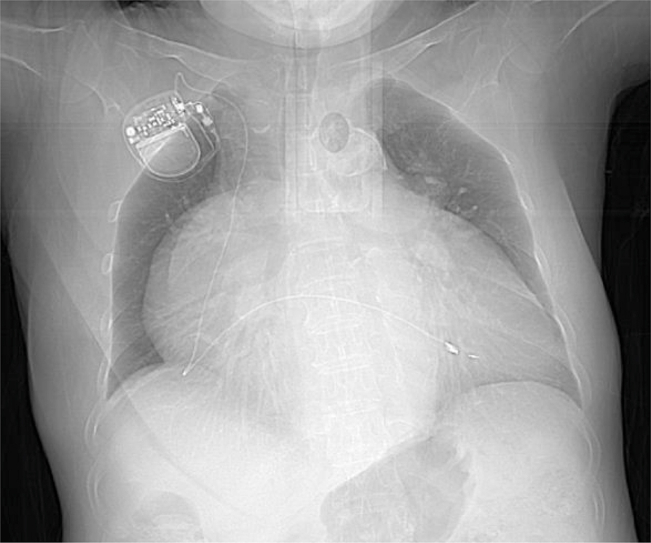 Figure 1
Figure 1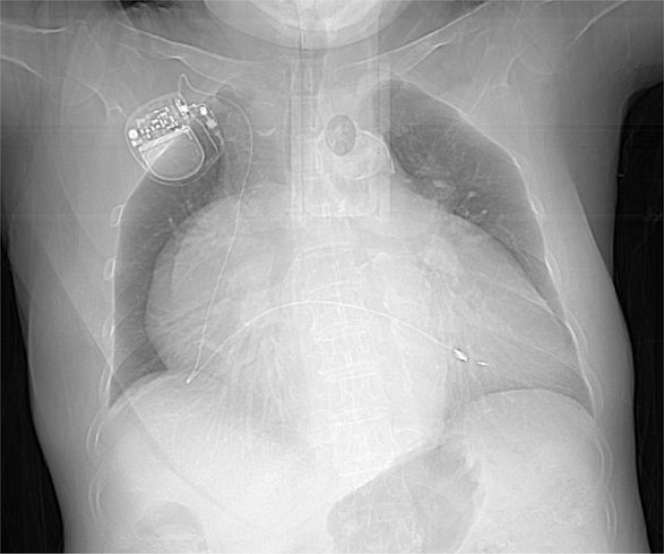 Figure 2
Figure 2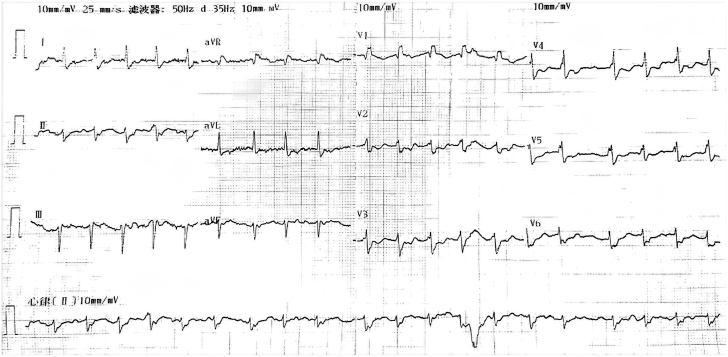 Figure 3
Figure 3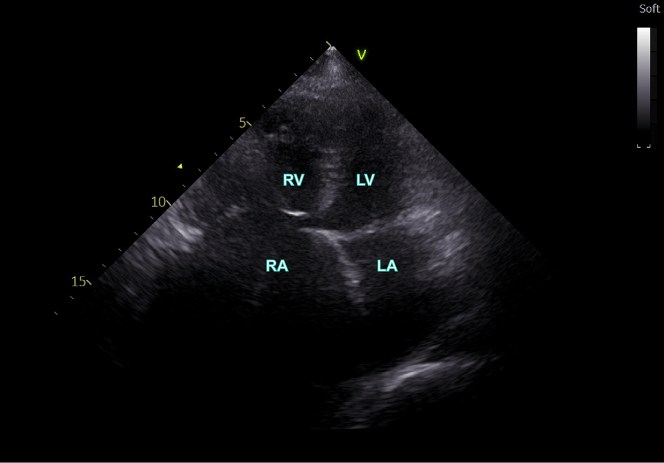 Figure 4
Figure 4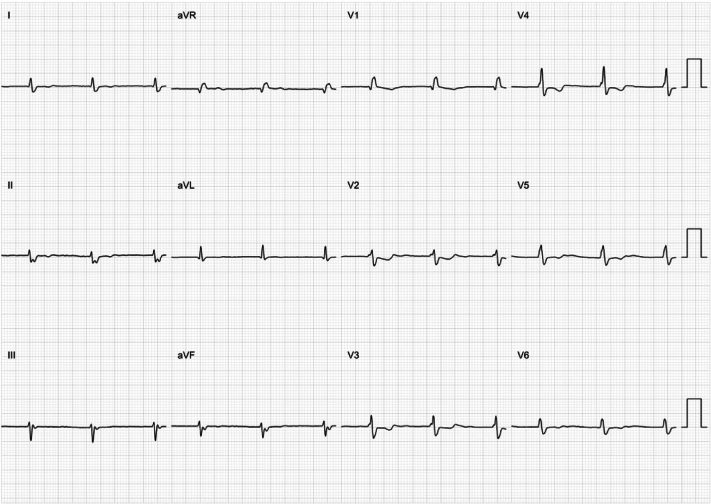 Figure 5
Figure 5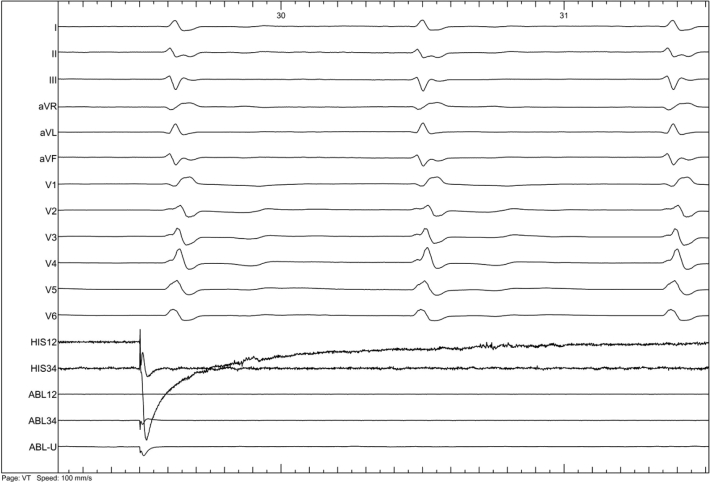 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes
Case Presentation
A 65-year-old Chinese female endured intermittent palpitations for 5 years. The prehospital electrocardiogram (ECG) indicated paroxysmal atrial fibrillation (AF), and chest radiograph revealed a giant heart (Figure 1). One week before current hospitalization, she presented with frequent palpitations and was diagnosed with AF via ECG (Figure 2). She was then admitted to the Cardiovascular Department.Take-Home Messages
- •The misdiagnosis of AS as AF emphasizes the complexity and subtlety of cardiac arrhythmia diagnosis, urging clinicians to be vigilant.
- •For patients with AS, accurate diagnosis using electrophysiological examination and timely implementation of treatment measures such as ventricular pacing are crucial for improving patient prognosis and the quality of medical care. Figure 1. Chest RadiographThe chest radiograph shows that the patient has a huge heart.Figure 2. ElectrocardiogramThe electrocardiogram obtained upon the patient’s admission suggested suspected atrial fibrillation.
On admission, her blood pressure was 113/76 mm Hg. Lungs were clear, bilateral heart border enlarged, and a grade 3/6 systolic murmur of the tricuspid valve was heard. The admission ECG showed no P waves, no distinct f waves, and supraventricular QRS waves. The bedside echocardiogram demonstrated a giant atrium with a left atrial inner diameter of 51 mm and a right atrial inner diameter of 71 mm (Figure 3), along with moderate tricuspid regurgitation and no A peak of the mitral valve.Figure 3. EchocardiogramThe echocardiogram demonstrated a significantly enlarged atrium. Specifically, the inner diameter of the left atrium measured 51 mm while that of the right atrium was 71 mm. LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.
Six months ago, a single-chamber pacemaker (ventricular pacing, ventricular sensing, inhibited) was implanted in the right ventricle due to significant bradycardia and long ventricular intervals. The patient was on dabigatran (110 mg, twice a day) for stroke prevention.
Based on clinical evidence, the main differential diagnosis was atrial standstill (AS) induced by atrial cardiomyopathy. After obtaining informed consent, an electrophysiological examination was performed. The ECG showed junctional rhythm without obvious P wave (Figure 4). During the electrophysiological examination, pacing tests were meticulously carried out at multiple key atrial sites, including the free wall of the right atrium, the right atrial appendage, the interatrial septum, and the coronary sinus. To ensure comprehensive assessment, the pacing voltage was elevated to its maximum level (range: 5-10 V, pulse width: 1.0-2.0 ms). In every instance, the atrium failed to be captured, verifying that the atrial electrical activity had vanished and that it was AS (Figure 5). The previous AF diagnosis was revised.Figure 4. Electrophysiological ExaminationThe electrophysiological examination revealed that the surface ECG presented junctional rhythm, lacking distinct P-waves. Abbreviation as in Figure 2.Figure 5. Pacing the Right AtriumWhen pacing the right atrium with a voltage of 10 V (2.0 ms), no capture was observed. This finding indicated the absence of atrial electrical activity, confirming the diagnosis of AS. AS = atrial standstill.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Discussion
In this case, the enlarged atrium and suspected cardiomyopathy disrupted the atrial electrophysiological environment. AS occurs due to the complete absence of atrial electrical and mechanical activity, often related to atrial myocardial cell and conduction system dysfunction, caused by advanced cardiac diseases, myocardial fibrosis, or genetic disorders.1
Differentiating AS from AF is crucial. Their ECG manifestations differ, with AF having chaotic atrial electrical activity and AS lacking it. Clinical manifestations and potential complications also vary, with AF associated with palpitations and thromboembolic risks, and AS with decreased cardiac output and junctional arrhythmias. The diagnosis of AS needs the following criteria. First, on the electrocardiogram, the P-waves should be completely absent. Second, cardiac electrophysiological examination must confirm the absence of any spontaneous electrical activity within the atrium. Third, other conditions that could potentially result in the disappearance of P-waves, including hyperkalemia and severe sinoatrial node dysfunction, need to be meticulously excluded.
Genetically, AS may be linked to SCN5A or HCN4 variants.2 Patients at risk of thromboembolic events due to lack of atrial pacing require anticoagulation or left atrial appendage closure. Accurate diagnosis of AS is essential for proper management and prognosis. Echocardiogram helps identify structural and functional atrial changes, and advanced electrophysiological studies clarify electrical abnormalities.
Treatment for AS depends on the cause and patient’s condition. Permanent AS may necessitate pacing therapy,3 with close monitoring and follow up to assess treatment effectiveness and detect complications. Left atrial appendage occlusion mainly prevents thromboembolic events. The atrium’s weakened activity leaves the left atrial appendage, with its special structure, a high-risk thrombus site due to slow, eddy-forming blood flow and hypercoagulability. The procedure removes this thrombus source, reducing stroke risks. Because AS is rare, there was scarce relevant literature and no reliable evidence yet.
This case underscores the critical significance of comprehensive and precise diagnosis. The initial misdiagnosis and the subsequent accurate diagnosis vividly demonstrate the imperative necessity for continuous monitoring of ECG and meticulous interpretation of echocardiogram. The discovery of the giant atrium and the electrophysiological findings ultimately paved the way for the correct diagnosis, which serves as a valuable lesson in the field of cardiology, emphasizing the importance of thorough examinations and vigilant monitoring in ensuring accurate disease identification and appropriate patient management.
Continuous monitoring and follow-up are also significant. The 10-month follow-up spanning from April 2024 to January 2025 not only attests to the effectiveness of the treatment but also accentuates the significance of long-term management. Overall, this case enhances clinicians’ understanding of cardiac arrhythmia differential diagnosis and treatment strategies for AS, improving the quality of patient care and optimizing health outcomes.
Conclusions
AS is a complex and frequently overlooked cardiac condition. Timely recognition and appropriate management, such as pacemaker implantation, are crucial for AS patients. For the ill at risk, achieving an accurate diagnosis through echocardiogram and electrophysiological examination is of paramount importance. This not only empowers medical professionals to make well-informed treatment decisions but also plays a pivotal role in enhancing the overall quality of patient care, ultimately leading to better health outcomes.
Data availability
All data relevant to this case report are included within the article. Any additional data not presented in the article can be made available on request to the corresponding author.
Funding Support and Author Disclosures
This research was supported by Capital Health Research and Development of Special Fund, China (2020-2-4203). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Howard T.S.Chiang D.Y.Ceresnak S.R.Atrial standstill in the pediatric population: a multi-institution collaboration JACC Clin Electrophysiol 9202357693643569410.1016/j.jacep.2022.08.022PMC 12998638 · doi ↗ · pubmed ↗
- 2Anand A.B.Shah B.S.Sabnis G.R.Mahajan A.U.Atrial standstill in a young patient with ischemic stroke associated with inheritance of a novel HCN 4 mutation J Arrhythm 402024151915223966992810.1002/joa 3.13150 PMC 11632268 · doi ↗ · pubmed ↗
- 3Hori H.Kosuga T.Hosokawa Y.Tayama K.Kosuga K.Atrial functional tricuspid regurgitation associated with atrial standstill Cureus 162024 e 6957710.7759/cureus.69577 PMC 1148363639421093 · doi ↗ · pubmed ↗