Dynamic changes in vasohibin and nitric oxide signaling following surgical resection of head and neck squamous cell carcinoma
Ying-Hsuan Tai, Hsiang-Ling Wu, You-Hsiang Chu, Cheng-Hsien Wu, Shyh-Kuan Tai, Tso-Chou Lin, Shung-Tai Ho, Chih-Cherng Lu

TL;DR
This study shows how levels of certain proteins and signals in the blood change after surgery for head and neck cancer, which could help monitor the disease.
Contribution
The study reveals dynamic changes in vasohibin and nitric oxide signaling in leukocytes after tumor resection in HNSCC patients.
Findings
Plasma VASH1 levels decreased significantly after tumor resection in HNSCC patients.
NO levels in plasma also dropped significantly following surgery.
Leukocyte iNOS phosphorylation increased after surgery, while VASH2 levels remained unchanged.
Abstract
Angiogenesis is essential for tumor growth and metastasis, with various molecules, including vasohibin (VASH), nitric oxide (NO), and inducible nitric oxide synthase (iNOS), implicated in its regulation and potential prognostic value in oncology. However, their roles in modulating surgery-induced angiogenesis in head and neck squamous cell carcinoma (HNSCC) remain unclear. Therefore, the objective of the study was to assess the dynamic changes in VASH, NO, and iNOS levels in HNSCC patients undergoing surgical resection. We prospectively enrolled patients with histology-proven HNSCC who underwent surgical resection of primary tumors at the medical center between May and November 2021. Non-cancer controls were recruited to compare baseline biomarker levels with those of HNSCC patients. We measured preoperative and postoperative levels of VASH1 and VASH2 in plasma and leukocytes using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
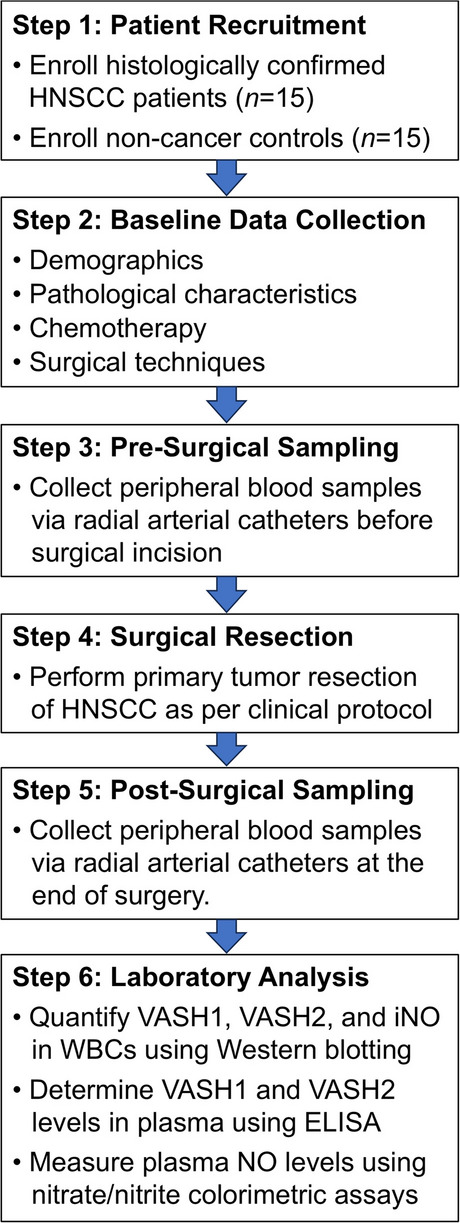 Figure 1
Figure 1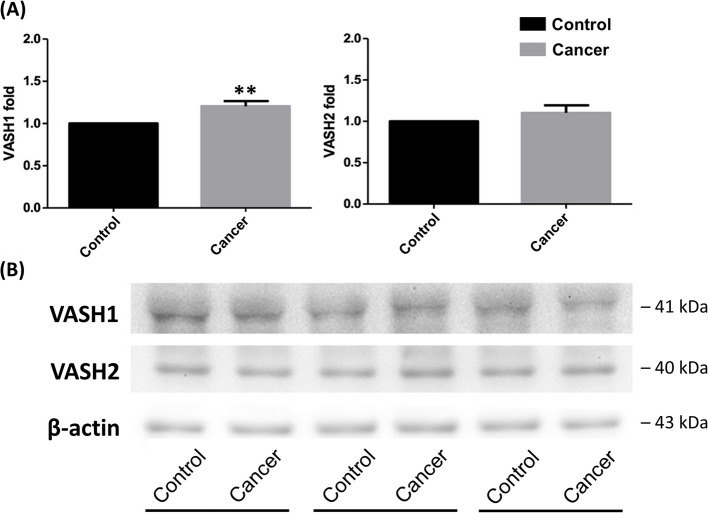 Figure 2
Figure 2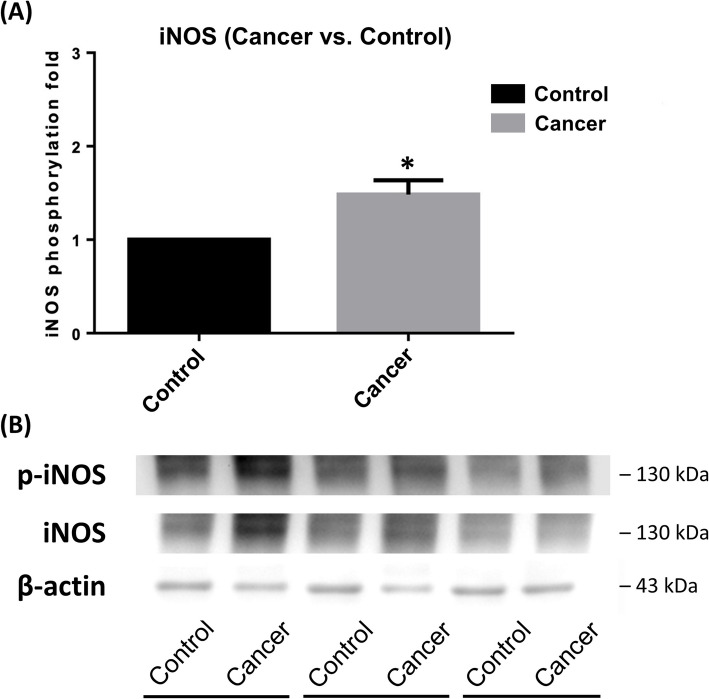 Figure 3
Figure 3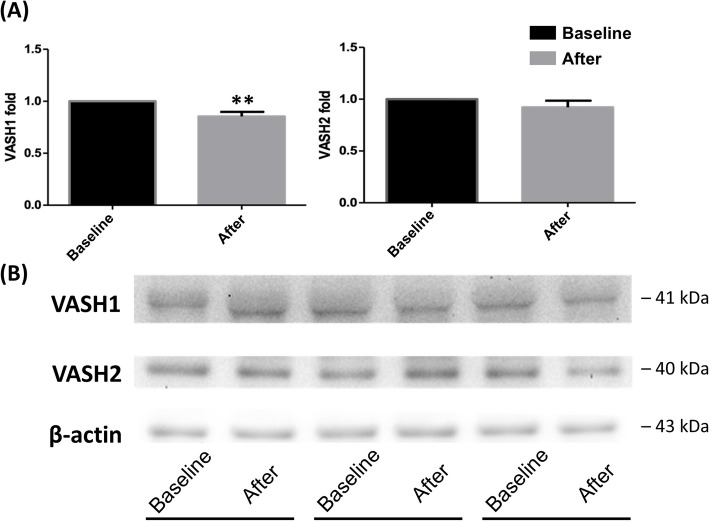 Figure 4
Figure 4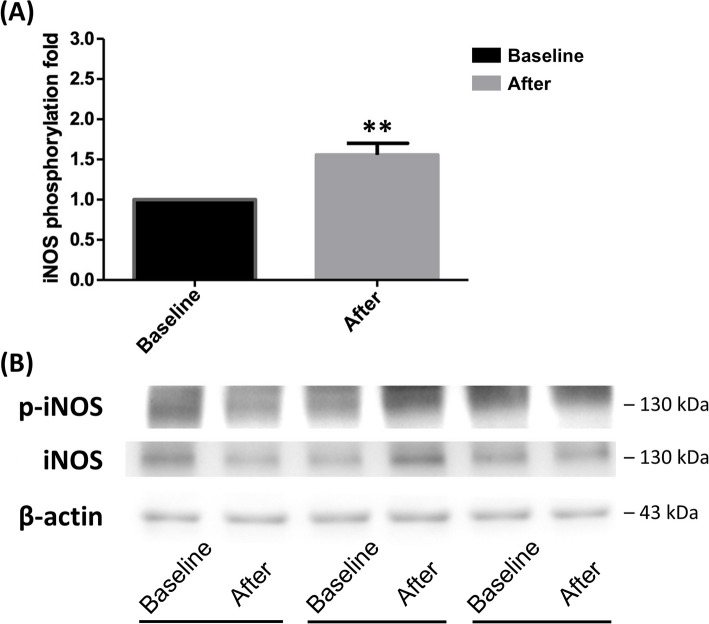 Figure 5
Figure 5- —https://doi.org/10.13039/501100011912Taipei Veterans General Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAngiogenesis and VEGF in Cancer · Cancer, Hypoxia, and Metabolism · Congenital heart defects research
Introduction
Angiogenesis, the process of forming new blood vessels, is a hallmark of cancer, playing a pivotal role in tumor growth, progression, and metastasis by supplying nutrients and oxygen to malignant cells [1]. Dysregulated angiogenesis disrupts the balance between stimulatory and inhibitory factors, enabling tumors to thrive and spread. Studying angiogenesis is critical in oncology, as targeting this process offers opportunities for novel diagnostics and therapies to halt cancer progression. Key molecules involved in angiogenesis include vasohibin-1 (VASH1) [2–4], vasohibin-2 (VASH2) [5–8], and nitric oxide (NO) [9, 10]. VASH1 and VASH2, as regulators of angiogenesis, exert opposing effects, while NO influences vascular dynamics, collectively shaping the tumor microenvironment [2–10]. Understanding their roles provides a foundation for exploring their potential as biomarkers or therapeutic targets in cancer.
VASH1 and VASH2 play contrasting roles in angiogenesis, a critical process driving tumor growth and metastasis in head and neck squamous cell carcinoma (HNSCC) [11]. VASH1, primarily expressed in endothelial cells (ECs), acts as a negative feedback regulator of angiogenesis, induced by vascular endothelial growth factor receptor (VEGFR) signaling via VEGFR2 and protein kinase C-delta (PKCδ), as well as by fibroblast growth factor [2–4]. In contrast, VASH2, expressed in infiltrating mononuclear cells or cancer cells, promotes angiogenesis and is frequently associated with poorer prognosis across various cancer types [5–8]. Notably, despite its anti-angiogenic role in ECs, elevated VASH1 expression in tumor blood vessels has been associated with poorer oncological prognosis and increased tumor recurrence, suggesting a complex role in tumor progression [12–16]. The interplay between VASH1 and VASH2 underscores their potential as prognostic biomarkers, with VASH1 levels in circulating white blood cells (WBCs) possibly indicating anti-angiogenic capacity, tumor behavior, and response to therapies.
NO, synthesized primarily by inducible nitric oxide synthase (iNOS) in response to inflammatory and pathological stimuli, is a key regulator of diverse physiological and pathological processes, including tumor growth, angiogenesis, and metastasis [9, 10]. iNOS-driven NO production promotes tumor vascularization by enhancing vasodilatation and increasing tumor vasculature permeability, often in concert with pathways like prostaglandin E2 signaling [17]. Our prior research identified stage-dependent changes in plasma levels of angiopoietin-1, angiopoietin-2, and NO following HNSCC tumor resection, indicating their role in an endogenous anti-angiogenic response to malignancy [18]. However, the specific impact of surgical resection on VASH1 and VASH2 concentrations, and the interplay between NO signaling and vasohibins in modulating surgery-induced angiogenesis, remain unexplored in HNSCC.
This study primarily aimed to evaluate the dynamic changes in angiogenesis-regulating molecules, specifically VASH1, VASH2, and NO in plasma, and VASH1, VASH2, and iNOS in circulating WBCs, in HNSCC patients undergoing surgical resection. By measuring these markers before and after surgery, we sought to elucidate their roles in modulating anti-angiogenic responses and their potential as prognostic indicators for survival. Additionally, we investigated the influence of the tumor process on these markers by comparing their baseline levels in plasma (VASH1, VASH2, NO) and circulating WBCs (VASH1, VASH2, iNOS) between HNSCC patients and non-cancer controls. This comparison aimed to clarify the physiological and regulatory roles of these molecules in tumor angiogenesis, providing insights into their neovascular behavior and potential for developing novel methods to assess angiogenic activity in cancer patients.
Materials and methods
Setting and patient enrollment
This study was approved by the Institutional Review Board of Taipei Veterans General Hospital in Taiwan (IRB-TPEVGH No. 2020–06-012 AC, date of approval: July 10, 2020). It was conducted in accordance with the institutional ethical standards and the Declaration of Helsinki 2013. Written informed consent was obtained from all participants prior to their enrollment.
Patients with pathology-confirmed HNSCC who underwent surgical resection of primary tumors at a tertiary medical center between May and November 2021 were recruited for this study. Patients were excluded if they met any of the following criteria: age below 20 years, previous diagnoses of leukocyte disorders (e.g., leukopenia and leukemia), or use of NO therapy (e.g., glyceryl trinitrate) within 30 days before surgery. Following the application of these selection criteria, a total of 15 patients with HNSCC were enrolled. For comparison, 15 age-matched healthy volunteers with no prior cancer diagnoses were recruited as non-cancer controls. This allowed for a comparative analysis of baseline levels of VASH1, VASH2, and NO signaling biomarkers between HNSCC patients and controls. The study methodology is presented in Fig. 1.Fig. 1. Flowchart illustrating the methodology for studying dynamic changes in vasohibin (VASH) and nitric oxide signaling following surgical resection of head and neck squamous cell carcinoma (HNSCC)
Study outcomes
The primary outcome assessed VASH1 and VASH2 expression levels in peripheral WBCs before and after HNSCC tumor resection. Secondary outcomes included plasma levels of VASH1, VASH2, and NO, and iNOS phosphorylation in WBCs in cancer patients before and after surgery. Baseline levels of these markers were compared between HNSCC patients and non-cancer controls. Using a median VASH1 change fold of 0.72 in leukocytes, we categorized patients into high-deltaVASH1 (≥ 0.72) and low-deltaVASH1 (< 0.72) groups, comparing their 1-year and 3-year overall survival rates, defined as the time from surgery to death from any cause, with data sourced from medical records and death certificates. Survival times for patients without death were censored, and follow-up continued until October 31, 2024.
Collection of covariates
Clinical data for the cancer patients were obtained from their electronic medical records. Demographic information included age, sex, body mass index, and history of tobacco smoking, alcohol consumption, and betelnut chewing within the 30 days prior to surgery. The American Society of Anesthesiologists physical status classification was used to evaluate their overall health status. Pathological features included primary tumor location (categorized as tongue, buccal mucosa, gingiva, palate, hypopharynx, or other), tumor cell differentiation, angiolymphatic invasion, perineural invasion, and tumor stage [19, 20]. Tumor, node, metastasis staging was categorized into stages I to IV according to the 8 th edition of the American Joint Committee on Cancer (AJCC) criteria [21]. Surgical factors included the use of preoperative chemotherapy, duration of anesthesia, intraoperative blood loss, intraoperative blood transfusion, and surgical procedures (neck dissection and flap reconstruction).
Blood sample collection
Peripheral blood samples were collected via radial arterial catheters before surgical incision (baseline) and at the end of surgery. Samples were stored in K2 ethylenediaminetetraacetic acid (EDTA)-containing tubes (Becton Dickinson, NJ, USA) for plasma and protein extraction. Plasma was centrifuged at 3000 rpm for 10 min without braking and stored at −80 °C. WBCs were isolated using Ficoll-Paque Plus (GE Healthcare Bio-Sciences AB, Uppsala, Sweden). Equal volumes of WBCs were added to an ice-cold wash buffer containing 1 mM Na_2_HPO_4_, 1 mM EDTA, and 1 mM phenylmethylsulfonyl fluoride (PMSF, Gold Biotechnology, St. Louis, MO, USA), at a pH of 7.4, in a 1:3 ratio. To remove hemoglobin, the WBCs membranes underwent four or more wash cycles, each involving centrifugation at 14,500 rpm for 20 min at 4°C. The washed WBCs membranes were then stored at −80°C for further analysis.
VASH1 and VASH2 expression
VASH1 and VASH2 proteins were extracted from WBCs, which were lysed using RIPA buffer to ensure efficient lysis and protein solubilization. The protein fraction was isolated via centrifugation. Western blotting was used to analyze the expression levels of VASH1 and VASH2 proteins. Protein samples were separated by SDS-PAGE, transferred to PVDF membranes, and blocked with 5% BSA. The membranes were incubated overnight with primary antibodies specific to VASH1 and VASH2, followed by HRP-conjugated secondary antibodies. An enhanced chemiluminescence (ECL) system was used for detection, and the protein band intensities were quantified using image analysis software to determine the expression levels of VASH1 and VASH2 in the leukocyte samples. To quantify plasma levels of VASH1 and VASH2, enzyme-linked immunosorbent assay (ELISA) kits were employed, following the manufacturer’s protocol, consistent with established methodologies from prior studies [22]. All measurements were performed in duplicate.
NO levels and iNOS phosphorylation detection
Plasma NO concentration was determined by measuring its stable end products, nitrite and nitrate [23]. Plasma nitrite and nitrate levels were measured using a nitrate/nitrite colorimetric assay kit (Cayman Chemical®, MI, USA). The first step involved converting nitrate to nitrite using nitrate reductase. Subsequently, Griess reagents were added. After 10 min of incubation at room temperature, the absorbance was measured at 550 nm using a microplate reader (BioTek Instruments, VT, USA).
Cytoplasmic proteins were extracted from leukocyte lysates to assess the phosphorylation of iNOS in WBCs. Following lysis of leukocytes with lysis buffer and isolation of the cytoplasmic fraction via centrifugation, iNOS protein was extracted. The phosphorylation levels of iNOS were analyzed using Western blotting. Protein samples were separated by SDS-PAGE, transferred to PVDF membranes, and blocked with 5% BSA. Membranes were incubated overnight with a primary antibody specific to phosphorylated iNOS, followed by an HRP-conjugated secondary antibody. An ECL system was used for detection, and the intensity of the protein bands was quantified using image analysis software to determine iNOS phosphorylation levels in the leukocyte samples. All measurements were performed in duplicate to determine the mean value.
Statistical analysis
A minimum sample size of 14 was determined to achieve 80% power to detect an 80% change in VASH1 or VASH2 levels in WBCs for paired comparisons, using a two-sided significance level of 0.05. Kolmogorov–Smirnov tests assessed normality. Independent t-tests or Mann–Whitney U tests compared baseline plasma levels of VASH1, VASH2, NO, and iNOS phosphorylation in WBCs between cancer patients and non-cancer controls, as appropriate. Paired t-tests or Wilcoxon signed-rank tests evaluated changes in these markers before and after surgery in HNSCC patients, as appropriate. All hypothesis tests used a two-sided significance level of 0.05. Statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and graphs were created with Prism version 5.0 (GraphPad Software, San Diego, CA, USA).
Results
Baseline patient characteristics
Table 1 presents the clinical characteristics of the included cancer patients. The average age of the cancer patients was 54.7 ± 11.2 years, with 12 (80.0%) being male. Regarding pathology, the primary tumor was located in the buccal mucosa in 5 (33.3%) patients, and 6 (40.0%) patients had stage IV cancer. Fourteen patients (93.3%) had moderately-differentiated tumors, and 5 (33.3%) and 6 (40.0%) patients had angiolymphatic invasion and perineural invasion, respectively. Nine patients (60.0%) underwent neck dissection to remove lymph nodes from the neck, and 6 (40.0%) underwent free flap reconstruction. In the non-cancer control group, the mean age was 58.7 ± 9.7 years, with 13 (86.7%) participants being male.Table 1. Clinical characteristics of the included cancer patientsCancer patients****(n = 15)****Age, year54.7 ± 11.2Sex, male12 (80.0%)Body weight, kg74.8 ± 14.2Body height, cm169.3 ± 5.8Body mass index, kg·m^−2^26.1 ± 5.1ASA class II8 (53.3%) III7 (46.7%)Tobacco smoking7 (46.7%)Alcohol consumption6 (40.0%)Betelnut chewing8 (53.3%)Primary tumor location Tongue3 (20.0%) Buccal mucosa5 (33.3%) Gingiva2 (13.3%) Palate1 (6.7%) Hypopharynx1 (6.7%) Other3 (20.0%)TNM classification T14 (26.7%) T22 (13.3%) T34 (26.7%) T4a2 (13.3%) T4b3 (20.0%) N011 (73.3%) N11 (6.7%) N2b1 (6.7%) N2c1 (6.7%) N3b1 (6.7%) M015 (100.0%)Cancer stage I4 (26.7%) II2 (13.3%) III3 (20.0%) IVa3 (20.0%) IVb3 (20.0%)Differentiation grade Good1 (6.7%) Moderate14 (93.3%) Poor0 (0)Angiolymphatic invasion5 (33.3%)Perineural invasion6 (40.0%)Preoperative chemotherapy1 (6.7%)Neck dissection9 (60.0%)Flap reconstruction6 (40.0%)Values were mean ± standard deviation or counts (percent)ASA American Society of Anesthesiologists, TNM tumor, node, metastasis
Table 2 presents intraoperative vital signs and laboratory testing data. The duration of anesthesia was 680 ± 235 min. The intraoperative blood loss volume was 600 ± 261 mL, and 3 (20.0%) and 1 (6.6%) patient received red blood cell and fresh frozen plasma transfusions during surgery, respectively.Table 2. Intraoperative vital signs and laboratory testing data of the cancer patientsPre-inductionEnd of surgerySystolic blood pressure, mmHg122 ± 15138 ± 16Diastolic blood pressure, mmHg69 ± 1569 ± 15Heart rate, beats·min^−1^81 ± 1077 ± 17Body temperature, ℃36.0 ± 0.236.2 ± 0.3SpO2, %99 ± 199 ± 1Serum glucose, mg·dL^−1^164 ± 53165 ± 38Serum hemoglobin, g·dL^−1^12.6 ± 1.513.5 ± 0.9Intraoperative parameters****Anesthesia duration, min680 ± 235Surgical blood loss, mL600 ± 261Blood transfusion Red blood cells3 (20.0%) Fresh frozen plasma1 (6.6%)Values were mean ± standard deviation or counts (percent). SpO_2:_ oxyhemoglobin saturation by pulse oximetry
Baseline levels of VASH1 and VASH2
Plasma VASH1 concentration was significantly higher in cancer patients compared to non-cancer controls (2425 ± 1493 pg·mL^−1^ vs. 1402 ± 368 pg·mL^−1^, p = 0.0097 by Mann–Whitney U tests; Kolmogorov–Smirnov test, p < 0.0100). However, no significant difference was observed in plasma VASH2 levels between the two groups. The expression level of VASH1 in WBCs was significantly higher in cancer patients compared to non-cancer controls (1.24 ± 0.06 folds, p = 0.0093 by independent t-tests; Kolmogorov–Smirnov test, p > 0.1500) (Fig. 2 and supplementary Figure S1). However, no significant difference was observed in VASH2 expression levels in WBCs between cancer patients and controls (1.15 ± 0.37 folds, p = 0.3030 by Mann–Whitney U tests; Kolmogorov–Smirnov test, p < 0.0100).Fig. 2A Baseline vasohibin-1 levels in WBCs were significantly higher in cancer patients compared to controls. However, there was no significant difference in vasohibin-2 levels in WBCs between the two groups. Data were presented as mean ± SD. (^**^P < 0.01 indicate a significant difference between cancer and non-cancer subjects). B A representative gel was shown. VASH1 = vasohibin-1; VASH2 = vasohibin-2
Baseline plasma NO level and WBCs iNOS phosphorylation
Plasma NO levels were significantly elevated in cancer patients compared to non-cancer controls, with means of 6.04 ± 2.23 μM versus 2.21 ± 1.62 μM (p = 0.0004 by Mann–Whitney U tests; Kolmogorov–Smirnov test, p < 0.0100), respectively. Additionally, the degree of phosphorylation expression of leukocyte-induced iNOS was significantly higher in cancer patients compared to non-cancer controls (1.48 ± 0.12 folds, p = 0.0235 by independent t-tests; Kolmogorov–Smirnov test, p > 0.1500) (Fig. 3 and supplementary Figure S2).Fig. 3A The baseline level of iNOS phosphorylation in WBCs was significantly higher in cancer patients compared to controls. Data were presented as mean ± SD. (^*^P < 0.05 indicate a significant difference between cancer and non-cancer subjects). B A representative gel was shown
Dynamic changes in VASH1 and VASH2
Plasma VASH1 levels were significantly reduced after tumor resection, 2233 ± 1464 pg·m^−1^ vs. 2425 ± 1493 pg·m^−1^ (0.90 ± 0.07 fold, p = 0.0085 by Wilcoxon signed-rank test; Kolmogorov–Smirnov test, p < 0.0100) (supplementary Figure S3). However, no significant change in plasma VASH2 levels was observed before and after surgery (0.94 ± 0.13 fold, p = 0.0980 by independent t-tests; Kolmogorov–Smirnov test, p > 0.1500). VASH1 expression levels in WBCs were significantly reduced after tumor resection (0.85 ± 0.04 fold, p = 0.0068 by Wilcoxon signed-rank test; Kolmogorov–Smirnov test, p < 0.0100) (Fig. 4 and supplementary Figure S4), while VASH2 expression levels did not change significantly after surgery (0.92 ± 0.11 fold, p = 0.4780 by Wilcoxon signed-rank test; Kolmogorov–Smirnov test, p < 0.0100). The 1-year and 3-year overall survival rates were 100.0% (95% CI: 100.0–100.0) and 100.0% (95% CI: 100.0–100.0) in the high-deltaVASH1 group, while the low-deltaVASH1 group had rates of 100.0% (95% CI: 100.0–100.0; p > 0.9999 by log-rank test) and 85.7% (95% CI: 63.3–100.0; p = 0.4795), respectively.Fig. 4A Vasohibin-1 expression in WBCs was significantly reduced after tumor resection in cancer patients. However, no significant change was observed in vasohibin-2 expression levels. Data were presented as mean ± SD. (^**^P < 0.01 indicate a significant difference before and after surgery). B A representative gel was shown. VASH1 = vasohibin-1; VASH2 = vasohibin-2
Dynamic changes in plasma NO and WBCs iNOS phosphorylation
Plasma NO concentration was significantly reduced in cancer patients after surgery (0.29 ± 0.09 fold, p = 0.0001 by Wilcoxon signed-rank test; Kolmogorov–Smirnov test, p < 0.0100). Additionally, the degree of phosphorylation expression of iNOS in WBCs increased significantly after surgery (1.52 ± 0.10 fold, p = 0.0024 by Wilcoxon signed-rank test; Kolmogorov–Smirnov test, p < 0.0100) (Fig. 5 and supplementary Figure S5).Fig. 5A The phosphorylation level of iNOS in WBCs was significantly enhanced after tumor resection in the cancer patients. Data were presented as mean ± SD. (^**^P < 0.01 indicate a significant difference before and after surgery). B A representative gel was shown
Discussion
This study revealed that VASH1 levels in WBCs and plasma were significantly elevated in patients with HNSCC, but the baseline level of VASH2 was similar between HNSCC patients and controls. Following surgical resection of HNSCC tumors, plasma and leukocyte levels of VASH1, but not VASH2, were significantly reduced, accompanied by a decrease in plasma NO. These findings may serve for monitoring the efficacy of therapeutic interventions for malignant tumors, particularly HNSCC.
Our study revealed significantly higher VASH1 levels in HNSCC patients compared to non-cancer controls, with no notable difference in VASH2 levels, reflecting their distinct roles in the tumor microenvironment. VASH1, primarily expressed in endothelial cells, is upregulated by pro-angiogenic factors like VEGF, which are often overexpressed in tumors to drive angiogenesis, likely acting as a feedback mechanism to regulate excessive vessel formation [2–4]. In contrast, VASH2, expressed in cancer cells or infiltrating mononuclear cells, may not be consistently elevated due to tumor heterogeneity or variable immune cell infiltration [5–8]. Additionally, post-surgical comparisons showed a significant decrease in VASH1 levels in WBCs and plasma, while VASH2 levels remained unchanged. This likely stems from the removal of the tumor-driven angiogenic microenvironment, where tumors secrete factors like VEGF that stimulate VASH1 and iNOS expression in WBCs, enhancing NO production to support vascularization [2–4]. Surgical resection removes this stimulus, diminishing inflammatory and angiogenic signals that activate these pathways.
The vasohibin family significantly influences tumor angiogenesis regulation [24]. Kopczynska et al. demonstrated that surgical resection of non-small cell lung cancer altered angiogenic factor levels, with angiotensin II and VEGF rising by postoperative day 7 and declining by day 30 [25]. However, prior studies have not explored whether tumor resection specifically affects VASH1 or VASH2 concentrations in cancer patients. VASH1 has emerged as a potential prognostic biomarker for HNSCC, with Torii et al. linking its expression in tumor cells to increased lymph node recurrence [12]. In prostate cancer, VASH1 density independently predicts prostate-specific antigen recurrence [26], and its expression correlates with tumor progression, metastasis, and micro-vessel density across cancers [27, 28]. Recombinant adenovirus encoding vasohibin shows promise in suppressing tumor angiogenesis and growth [29]. Although VASH1 holds promise, the search for predictive biomarkers in HNSCC persists, particularly focusing on immune checkpoint inhibitors targeting the programmed cell death protein-1 pathway [30]. Our research suggests vasohibin activation in WBCs could serve as a novel biomarker for assessing angiogenic activity, tracking metastasis, and evaluating chemotherapy efficacy, enhancing precision in HNSCC diagnosis and treatment alongside established markers [31–33]. Further studies are needed to validate the prognostic value of vasohibin and identify additional biomarkers for targeted therapies and immunotherapies.
The lack of significant changes in VASH2 levels following surgical resection of HNSCC may arise from multiple factors. In contrast to VASH1, which is closely linked to tumor progression and angiogenesis, VASH2 may play a more restricted or context-dependent role within the HNSCC tumor microenvironment. For instance, VASH2 expression might be primarily governed by local microenvironmental signals, such as hypoxia or cytokine profiles, which remain largely unaffected by resection [34, 5]. Alternatively, VASH2 may predominantly influence early tumor development, with its expression stabilizing in advanced HNSCC, resulting in minimal responsiveness to surgical intervention [35]. This stability suggests that VASH2 may not be a primary driver of angiogenesis regulation in this context, potentially diminishing its value as a therapeutic target or biomarker in advanced HNSCC. Further research is essential to elucidate the specific role of VASH2 and its interactions with other angiogenic factors, providing deeper insights into its implications for tumor behavior and vascular remodeling in HNSCC.
In our study, HNSCC patients displayed significantly higher plasma NO metabolite levels than non-cancer controls, with a notable reduction after tumor resection. This reduction possibly correlates with reduced VASH1 levels, driven primarily by endothelial NO synthase (eNOS) phosphorylation rather than iNOS activity measured in WBCs [36]. Intriguingly, iNOS phosphorylation in WBCs increased after surgery, contrasting with the decline in plasma NO metabolites, suggesting attenuated vasohibin and NO signaling in WBCs and a normalization of plasma NO levels toward those of non-cancer individuals. NO signaling influences HNSCC angiogenesis and tumor behavior in complex ways. At low levels, eNOS-derived NO from tumor or endothelial cells promotes angiogenesis by enhancing VEGF expression and endothelial cell proliferation, supporting tumor growth [37]. Conversely, high iNOS-derived NO levels from immune cells, like macrophages, may exert cytotoxic effects, inducing tumor cell apoptosis and inhibiting progression [37]. Additionally, NO modulates the tumor microenvironment by regulating immune cell infiltration and cytokine production, potentially fostering immunosuppression or enhancing anti-tumor responses [38]. The interplay between NO levels, cellular sources, and the HNSCC microenvironment underscores its dual role, necessitating further research to elucidate mechanisms and therapeutic potential.
Assessing angiogenesis-regulating markers, including VASH1, VASH2, and iNOS, in circulating WBCs provides deeper insights into the tumor microenvironment and immune response in HNSCC, surpassing the limitations of plasma measurements alone. Prior research indicates that WBCs and platelets in cancer patients harbor significantly higher VEGF levels than in healthy controls, contributing to tumor angiogenesis and metastasis [39]. While angiogenic factors like basic fibroblast growth factor and angiogenin show potential, their clinical utility is less established than VEGF [40]. In acute myeloid leukemia, elevated cellular VEGF levels independently predict shorter survival [41]. In contrast to plasma, which measures systemic levels of VASH1, VASH2, and NO, circulating WBCs actively contribute to tumor-associated immune and angiogenic activities, expressing these markers in direct response to tumor signals. This dynamic expression offers a direct view of cellular mechanisms driving tumor progression, capturing localized activity that plasma may obscure. Our study found that VASH1 and NO signaling in WBCs decreased after HNSCC tumor resection, highlighting their potential for monitoring therapeutic responses.
This study has several limitations. First, we did not monitor long-term postoperative changes in VASH1 and VASH2 levels. Second, we did not assess the relationship between vasohibin levels and cancer recurrence risk, leaving uncertainty about their predictive value for oncological outcomes in HNSCC. Third, the modest sample size may have limited statistical power for certain outcomes and restricted comprehensive multivariable adjustments. Fourth, the mechanisms underlying how dynamic changes in vasohibin and NO levels in WBCs affect angiogenesis or tumor behavior remain unclear, necessitating further in vitro or in vivo studies to explore interactions with the tumor microenvironment following surgery or anticancer therapy. Finally, the observational study design may introduce confounding from unmeasured or unadjusted factors, such as immune-modifying drugs or anesthesia management.
The findings of this study offer several perspectives for guiding future research in HNSCC and tumor angiogenesis. First, the observed dynamic changes in VASH1, VASH2, and NO signaling in WBCs and plasma following surgical resection highlight their potential as biomarkers for monitoring angiogenic activity and therapeutic responses. These insights pave the way for longitudinal studies to track vasohibin and NO levels over extended postoperative periods to assess their predictive value for oncological outcomes. Second, the distinct roles of VASH1 and VASH2 in the tumor microenvironment suggest avenues for investigating their interactions with other angiogenic factors, such as VEGF, and immune checkpoint pathways to optimize targeted therapies and immunotherapies. Last, future research should also focus on larger, controlled studies to validate these biomarkers, elucidate underlying molecular mechanisms, and explore their utility in personalized treatment strategies, ultimately enhancing precision medicine for HNSCC patients.
Conclusions
This study identified angiogenesis regulators as potential biomarkers in HNSCC patients. We observed downregulation of VASH1 and NO in plasma and VASH1 in circulating WBCs following curative surgical resection, while iNOS levels were upregulated in WBCs. Compared to non-cancer controls, HNSCC patients showed elevated VASH1 and NO in plasma and VASH1 and iNOS in WBCs. These findings suggest that these biomarkers may hold prognostic and predictive value in HNSCC. However, further studies are required to validate these results and assess their clinical utility in oncology practice.
Supplementary Information
Supplementary Material 1.