Implant displacement to the maxillary sinus– a retrospective multicenter cohort study and a management protocol
Daniel Muchnik, Gavriel Chaushu, Eli Rosenfeld, Shaked Adut, Aiman Elmograbi, Meir Debecco, Amir Laviv, Daya Masri

TL;DR
This study examines dental implants moving into the maxillary sinus, identifies common complications, and suggests surgical treatments like Functional Endoscopic Sinus Surgery.
Contribution
A new management protocol is proposed for implant displacement into the maxillary sinus, emphasizing surgical intervention based on clinical symptoms.
Findings
91% of patients with displaced implants required surgical intervention.
Functional Endoscopic Sinus Surgery was the most common treatment method.
Displacement often occurred during implantation and was linked to sinusitis and oroantral fistulas.
Abstract
This study aims to investigate the potential complication of implant displacement into the maxillary sinus, exploring its etiology and various management strategies, while proposing a systematic approach for clinicians to effectively address this evolving complication. This retrospective multi-center cohort study evaluated patients with dental implant migration into the maxillary sinus treated between 2010 and 2023 at two Israeli medical centers. Data included demographics, symptoms, clinical findings, and treatment modalities. 32 patients (mean age: 62.3 years) were analyzed, with a notable incidence of sinusitis and oroantral fistulas. 91% required surgical intervention, predominantly Functional Endoscopic Sinus Surgery (63%). The majority of displacements occurred during the implantation process, often correlating with clinical symptoms. As shown in our study, displacement of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
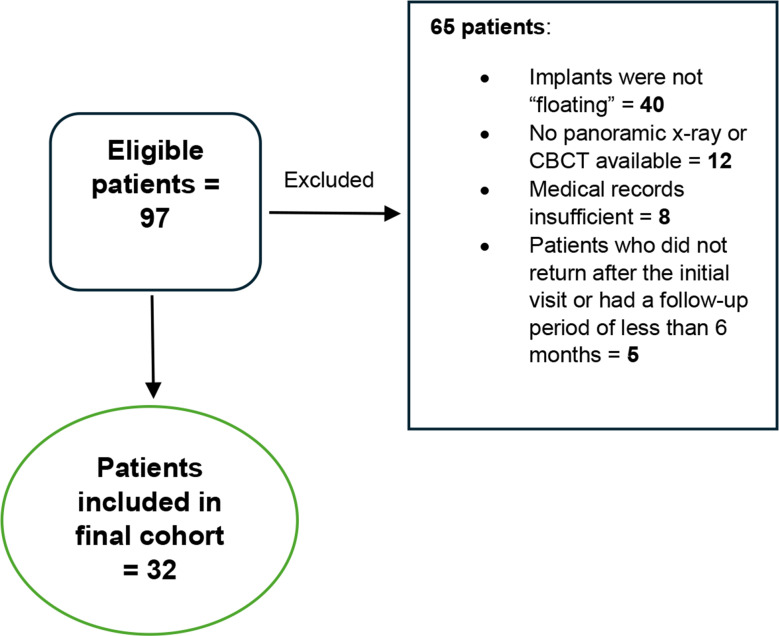 Figure 1
Figure 1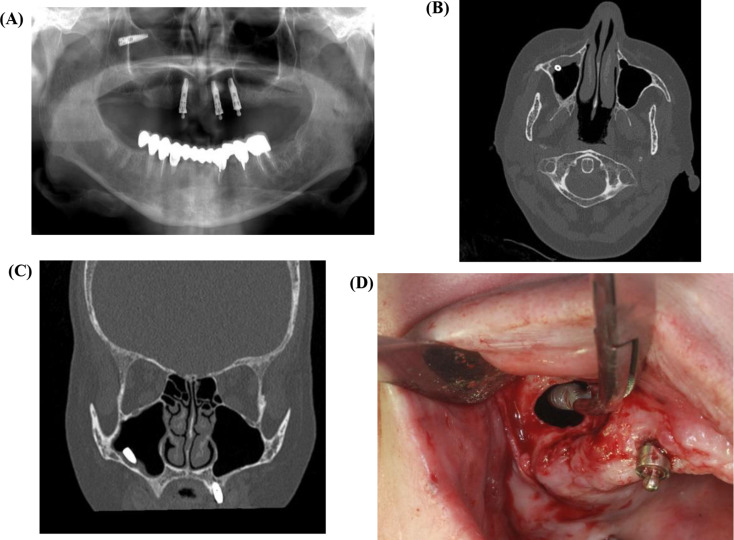 Figure 2
Figure 2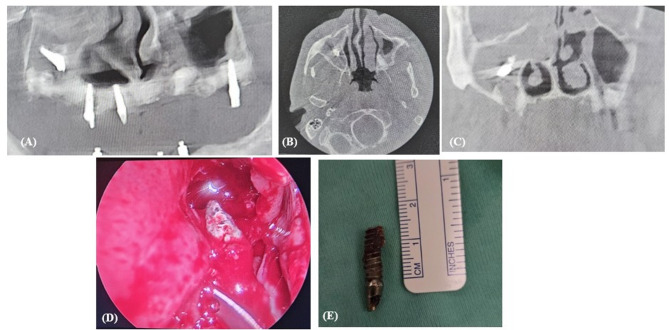 Figure 3
Figure 3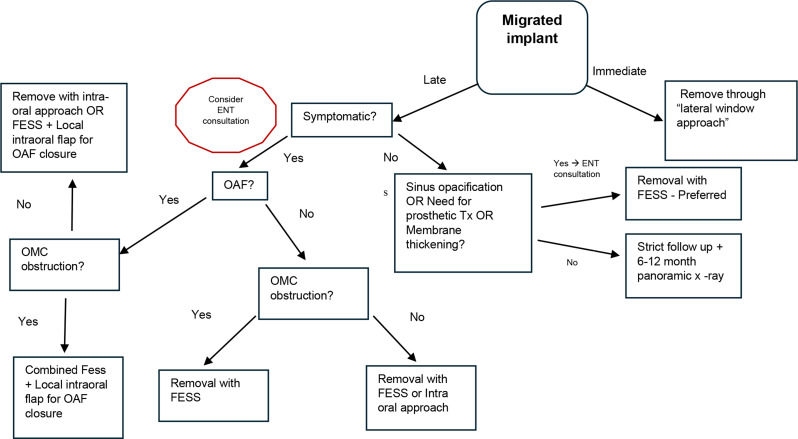 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Implant Techniques and Outcomes · Sinusitis and nasal conditions · Head and Neck Surgical Oncology
Background
Dental implants have become a common solution for restoring upper posterior teeth. However, several factors must be addressed to achieve successful long-term rehabilitation, including poor bone quality of the maxilla, pneumatization of the maxillary sinus, and alveolar bone resorption in edentulous areas. A critical factor influencing the success of the implantation procedure is primary stability, which prevent micromovements, facilitate clot adherence and the beginning of bony healing process around implant. Late migration of the implant into the sinus can occur due to loss of osseointegration, which may happen during the exposure procedure, after loading due to peri-implantitis or unfavourable distribution of occlusal forces. Other risk factors for displacement of dental implants into the maxillary sinus have been suggested to include inadequate drilling protocol, and insufficient surgical experience [1, 2].
This potential complication in oral implantology must be considered by clinicians [3, 4]. Research indicates that dental implants are frequently encountered foreign bodies within the maxillary sinus [5, 6]. Such complications can result in serious sequelae, including the development of oroantral fistula (OAF), maxillary sinusitis, and, in rare instances, orbital cellulitis or intracranial infections [7–9].
Various therapeutic approaches have been proposed, ranging from observation without removal to several surgical techniques [10, 11]. These methods have evolved considerably over the years, with the “Caldwell-Luc” and lateral sinus approaches being the most documented in the literature [12–14]. In the early 2000s, functional endoscopic sinus surgery (FESS) emerged as a significant technique in this area [14, 15].
Most existing literature has primarily reported individual cases or small series, making it challenging to draw comprehensive conclusions. This study aims to investigate the potential complication of implant displacement into the maxillary sinus, exploring its etiology and various management strategies, while proposing a systematic approach for clinicians to effectively address this evolving complication.
Materials and methods
Aim
Examine implant displacement into the maxillary sinus, its causes, management strategies, and propose a systematic approach for clinicians to handle this complication.
Study design
This study was conducted as a retrospective multi-center cohort study.
Study group
The study involved patients diagnosed with migration of dental implants into the maxillary sinus who sought treatment at the Department of Oral and Maxillofacial Surgery from 2010 to 2023 at two medical centers in Israel: Rabin Medical Center, Beilinson Campus, Petah Tikva, and Assuta Medical Center, Ashdod.
Inclusion criteria
Participants included those referred to the maxillofacial surgery departments of the aforementioned medical centers with a confirmed diagnosis of dental implant migration to the maxillary sinus.
Exclusion criteria
Patients were excluded if they did not have a “floating” implant in the maxillary sinus, lacked panoramic or CBCT radiographs, if demographic records were inadequate. Patients with a zygomatic implant which was present on the side where the displacement occurred, were also excluded.
Data collection
Data were gathered from patient records using a structured form, compiled from the hospitals’ medical records, and organized in Microsoft Excel.
Demographic information recorded included age, gender, ASA classification, and smoking history. The reason for hospital referral was also documented, detailing whether it was due to dentist referral, any symptoms (rhinologic or dental), incidental findings (without symptoms), or pre-prosthetic needs. Rhinologic symptoms encompassed headache, smell disturbances, and nasal discharge or congestion, while dental symptoms included oral pus discharge, pain around the implant site, intra/extraoral swelling, or fluid passage between the oral and nasal cavity.
Sinusitis was diagnosed according to the international multidisciplinary consensus statement on the diagnosis of odontogenic sinusitis (ODS) [16]. This consensus highlighted the need for both otolaryngologists and dental specialists to recognize sinusitis based on specific clinical features, ensuring that patients are appropriately referred for diagnosis confirmation.
The features that raise suspicion of sinusitis include:
- Unilateral sinus symptoms, such as foul odor, loss of smell, posterior nasal drainage, anterior nasal drainage, nasal obstruction, and facial pressure.
- Unilateral maxillary sinus opacification seen on CT scans.
To confirm sinusitis, an otolaryngologist should perform nasal endoscopy, which may reveal purulence, edema, or polyps.
Data on the timing of implant displacement to the sinus were categorized as either immediate (during insertion or removal of the implant) or late (occurring during the osseointegration period or subsequent exposure procedure). If information regarding the timing was unavailable, it was classified as NA (Not Available). The status of whether the implant was placed immediately after extraction was also noted, with missing information marked as NA. In addition, whether or not sinus elevation was performed prior to implant placement, was recorded.
All patient symptoms and clinical signs were documented, including pain, pus discharge (oral or nasal), the presence of OAF and diagnosis of sinusitis. Patients referred to ENT when exhibited rhinological signs which is suspicious for sinusitis (facial pain/pressure, foul smell, any nasal discharge, congestion or blockage or symptoms and/or obstruction of the osteo-meatal complex (OMC). No nasal signs or symptoms were reported by the patients before the implantation procedure.
Treatment modalities were categorized as surgical or non-surgical. Surgical retrieval methods included techniques such as FESS, Caldwell-Luc approach, lateral sinus approach, and transcrestal approach. Non-surgical treatments encompassed no treatment, symptomatic relief, or antibiotics. Any complications during treatment or in the postoperative period were also recorded. If OAF was present, the closure technique was investigated. Timing for removal was categorized based on whether it occurred within one year of implant displacement or after one year.
Radiographic data were derived from panoramic, Cone Beam Computed Tomography (CBCT) and Multidetector Computed Tomography (MDCT) images. The choice of which CT to perform was primarily determined by clinical signs and symptoms. Patients without rhinologic complaints were referred for CBCT, while those with rhinologic issues and/or OMC obstruction on CBCT were referred for MDCT. Documented data included whether the OMC was obstructed, the thickness of the sinus membrane (considered pathological > 2 mm), sinus floor thickness in the area of implant displacement, which maxillary sinus the implant migrated into, and whether other paranasal sinuses were affected. Additionally, if available, the length of the displaced implant was measured on CBCT in both coronal and sagittal views, utilizing an in-program ruler.
The final proposed treatment algorithm was developed based on the data collected and the analysis of clinical sequelae and radiographic findings.
Statistical analyses
Statistical analyses included descriptive statistics arranged in Microsoft Excel’s tables. All relevant study data (number of cases for each category, average, and standard deviation -SD, were calculated using Excel’s in-program functions).
Results
Demographic data
This study included a total of 32 patients who were diagnosed with displaced implants into the maxillary sinus (Table 1). Data regarding patients who were excluded summarized in Fig. 1.
Fig. 1. Patient inclusion & exclusion process
The mean age was 62.3 years (ranging from 19 to 86 years, SD = 14.7). The patient demographic consisted of 18 males and 14 females, and the American Society of Anaesthesiologists (ASA) classification showed that no patients exceeded ASA 3, indicating a relatively low surgical risk within the cohort. Among the participants, 10 patients (31%) had a history of smoking.
Background for implant displacement
Patients were referred for various reasons. The predominant admission reasons included dental and rhinologic symptoms (12 patients), pre-prosthetic evaluations (9 patients), dentist referral after displacement (8 patients) and incidental findings (3 patients). Notably, 36% (12 patients) reported symptoms related to the migrated implant, including 8 patients with rhinologic symptoms and 4 with dental symptoms. Pus and pain were the most frequently observed clinical signs, present in 16 patients (50%) and 10 patients (31%), respectively.
Timing of implant displacement
In 8 out of the 15 patients (53%) for whom data was available, implant migration occurred during the implantation process, while in another 4 patients (27%), it happened during the exposure phase. Rest of the implants migrated during osseointegration period (between implant placement & exposure procedure).
Sinusitis and OMC obstruction
Sinusitis was observed in 16 patients (50%). Radiological signs of thickened membrane were seen in this subgroup (100%) and ostium obstruction presented in CT in 13 patients (81%).
Implant length and sinus membrane thickness
The mean implant length was 10.8 mm (out of the available information), and the average sinus floor thickness measured 2.2 mm, while the maximal thickness reached 3.6 mm. Only 9 patients (28%) had prior history of sinus floor elevation.
Surgical intervention
In terms of surgical interventions for managing complications (Table 2), FESS was performed in 20 patients (63%), while 4 patients underwent Caldwell-Luc procedures, 4 (9%) had lateral approaches and 2 underwent trans-crestal approach (6%); In 2 patients no surgical treatment needed, while in 1 of them (3%) the implant was discharged from nasal complex during sneezing. Twelve patients exhibited OAF, with specific surgical methods utilized for their closure, including buccal advancement flaps, buccal fat pad and palatal rotation flap.
Timing of implant removal
Among the patients received surgical treatment (30 patients), implant removal was conducted with a mean time to removal documented at less than one year in 17 patients (57%) and greater than one year in 13 patients (43%).
Discussion
Dental implants have become a prevalent solution for patients with missing teeth. This procedure has become a widespread procedure and is performed by many dentists and oral surgeons. As the frequency of implant placement, especially in the posterior maxilla, is rapidly increasing, the number of complications such as the displacement of implants to the maxillary sinus will probably also rise.
Signs and symptoms of implant migration to the maxillary sinus
In the present study, 12 out of 32 patients (37.5%) referred with clinical symptoms, while 8 of them (67%) suffered from rhinologic symptoms and 4 (33%) suffered from dental symptoms. Another 12 (37.5%) patients were admitted with migrated dental implant to the maxillary sinus as coincidental finding or for prosthetic reason, while 5 of them (42%) had clinical and/or radiological signs of sinusitis. Other 8 patients out of the total cohort (25%) were referred by the dentist after displacement in different time-frames which will be discussed later. Only 3 of them (37.5%) diagnosed with sinusitis, 3 had pain and OAF (37.5%). This data indicates that a significant number of patients may remain asymptomatic and seek treatment either as a random discovery or for future prosthetic needs.
Migration of implants into the maxillary sinus may irritate the sinus lining or block the OMC, which could lead to sinusitis. While the development of sinusitis may be postponed for several months or even years, prior studies have indicated that not all patients with displaced implants show clinical symptoms or significant radiographic pathological changes. In another study detailing 9 cases, 3 patients reported sinus infections, whereas the remaining 6 did not show any symptoms [17]. Chiapasco et al. noted in his study that 13 out of 21 patients were asymptomatic and only 8 patients sought for medical care due to sinusitis symptoms or OAF [11]. Petruson et al. also stated that the existence of dental implants in the maxillary sinus does not automatically lead to sinus-related issues [18]. Possible explanation he mentioned is that production of nitric oxide inside the sinus may prevent infections around implants [19].
Etiology and timing of implant migration
Regarding the potential causes and risk factors for implant migration, we examined sinus floor thickness, implant length, and prior sinus floor elevation. According to dental history and CBCT, only 9 patients (28%) had a previous history of sinus floor elevation. All patients had less than 4 mm of residual bone height (averaging 2 mm) around the area of implant displacement, while the average implant length was 10.7 mm. In a study by Sgaramella et al. only 6 out of 21 patients (29%) had undergone a sinus lift procedure before implant placement, and in almost all cases, no traces of bone graft material were found at the time of examination [4]. The same conclusions were drawn in another study by Manor et al. which showed implant migration occurred mainly in cases of bone deficiency and lack of sufficient residual bone for osseointegration [20]. This data suggests that inadequate treatment planning or poorly executed bone augmentation significantly contribute to the risk of implant displacement into the sinus. It underscores the importance of achieving primary stability, which is crucial for a successful surgical outcome.
In the present study in 8 out of 15 patients (53%) the implant migration occurred during implant placement procedure. As highlighted in earlier studies, obtaining adequate primary implant stability during simultaneous sinus elevation can be challenging, with a minimum residual bone height of 4 to 5 mm recommended [21, 22]. If the implant is unstable during placement, it may be necessary to remove it and carry out the grafting and implant placement in two separate stages. When the bone height is less than 5 mm, primary stability is at risk, leading to the traditional recommendation of performing a sinus lift and bone augmentation, with implant placement occurring 4–6 months later as a second stage. However, it is now possible to perform a sinus lift and bone augmentation with implant placement as a single stage even when the subantral bone is below 5 mm, provided certain conditions are met and there is significant surgical expertise. Additionally, bone quality should be considered, as it may necessitate underdrilling and the use of a wider implant. However, a key requirement for a one-stage approach is achieving initial implant stability [22, 23]. In 4 out of 15 patients (27%) the migration occurred during exposure procedure, which may be explained by failure of implant osteointegration and/or application of excessive forces during the procedure or in attempt to remove the non-integrated implant. Three implants migrated during osteointegration period (20%) and in other 17 patients data about the timing of implant displacement was not available, but we hypothesize that at least some of them were displaced during late period after exposure, which may also occur due to excessive loading forces, or progressive bone loss and peri-implantitis [24]. In this study, no information was available regarding the clinical experience of the clinician who performed the implant surgery, or treatment plan and surgical protocol that was executed before admission to the hospital. In summary, the primary factors related to the etiology of implant displacement identified in our study are linked to inadequate bone support and the subsequent challenges in achieving primary stability. This is evidenced by the insufficient bone height observed in our patient cohort, the inadequate or absence of prior bone augmentation procedures, and the fact that displacement occurred at the time of implantation in the majority of cases.
Clinical and radiological signs
Membrane thickening was observed in 88% of cases (28 out of 32 patients), and ostium obstruction was seen in 16 cases (50%), of which 13 patients were diagnosed with sinusitis. OAF were present in 12 patients (37.5%), with 50% (6 patients) experiencing obstruction of the OMC. The presence of a thickened membrane (over 2 mm) may be attributed to a foreign body reaction, local inflammation, or even infection resulting from the displaced implant and/or augmented sinus floor. When a migrated implant disrupts the anatomy of the Schneiderian membrane, it can impair mucociliary function, hindering ventilation and drainage, and allowing bacteria and viruses to access the OMC. The OMC may become obstructed for various anatomical and functional reasons, contributing to the development of sinusitis [25]. All these factors may subsequently lead to the formation of OAF, as indicated in previous studies [11, 26]. Chiapasco et al. reported that 7 out of 13 patients with sinusitis had ostium obstruction (54%), a lower prevalence than noted in our study (13 out of 16 patients, 81%). They also found that 19 out of 27 patients diagnosed with oroantral communication (70%), a figure which is higher comparable to our study (12 patients, 37.5%). Manor et al. Also reports higher prevalence of OAF (83%) [20]. This could be attributed to the timing of definitive treatment, which may be longer in other studies. In the present study, all OAFs that developed in patients with sinusitis were associated with obstructed OMC (5 cases), leading to impaired drainage. Conversely, the OAFs that developed in patients without sinusitis may have arisen due to the position of the displaced implant along with the presence of dense inflammatory tissue that facilitated OAF formation.
Treatment modalities
A total of 29 patients were treated surgically (91%), with FESS being employed in most cases (69%), followed by Caldwell-Luc procedure (14%), lateral approach (10%), and trans-crestal approach (7%). In one patient, the implant dislodged spontaneously through the nose during sneezing, despite her experiencing rhinologic symptoms and being scheduled for surgical intervention. In two patients (6%), no treatment was necessary as they exhibited no clinical symptoms or signs, and there were no intended prosthetic treatment plans. These patients were informed about the importance of strict follow-up. Few studies suggested that displaced dental implants in the maxillary sinus can lead to chronic maxillary sinusitis, necessitating surgical intervention even in asymptomatic patients [27, 28]. This perspective is also supported by the recent meta-analysis, which found that only 3.8% of cases were simply observed [2]. Observation may be considered in the absence of clinical symptoms or upon the patient’s request. It may also be indicated when the surgical removal of the intra-sinus implant poses risks due to its proximity to the orbital floor. In our study, 29 out of 32 patients (91%) underwent surgical intervention for implant removal, consistent with findings from other reports. Although some studies have indicated long-term follow-ups (greater than 12 months) without irritation of the sinus mucosa, such cases are rare, and patients must be adequately informed about the long-term risks of infection [1, 29–31].
The traditional method for treating sinus pathologies and removing foreign bodies has been the Caldwell-Luc surgery. This procedure involves creating a bony window near the canine fossa to access the maxillary sinus via the anterior wall, including performing an inferior meatal antrostomy. While this technique was commonly used in the early 20th century, it has become less frequently indicated in light of developments such as the lateral approach (Fig. 2) and FESS (Fig. 3), which are less invasive. Common complications associated with Caldwell-Luc surgery included recurrent nasal obstruction, facial asymmetry, facial numbness, OAF, wound dehiscence, dacryocystitis, devitalized teeth, recurrent sinusitis, and recurrent polyposis [13, 30].
Fig. 2. Displaced implant removal using lateral sinus approach. (A) Pre-operative panoramic x-ray, (B). Pre-operative CT in axial and (C) coronal view’s demonstrating the implant inside the right maxillary sinus with membrane thickening, (D) Removal of the implant through the “lateral approach”
Fig. 3. Displaced implant removal using FESS. (A) Pre-operative panoramic x-ray; (B) Pre-operative CT in axial view demonstrating the implant inside the right maxillary sinus with sinus opacification; (C) Pre-operative CT in coronal view demonstrating the implant inside the right maxillary sinus with OMC obstruction; (D)Removal of the implant through FESS; (E) Implant after removal
Tatum introduced less invasive intra-oral lateral sinus and trans-crestal approaches, which eliminate the need for additional inferior antrostomy and are now favored for sinus lifts, augmentations, and the removal of foreign bodies, usually leading to fewer complications [32]. However, they do not address cases with OMC obstruction.
FESS has become increasingly popular as a treatment for sinus pathologies and for retrieving foreign bodies. This approach facilitates the removal of displaced implants, addresses paranasal sinusitis, and restores proper patency of the natural maxillary ostium through a minimally invasive technique [33, 34]. One of the primary side effects reported from FESS is the formation of synechiae due to scar formation between the inferior turbinate and nasal septum, which appear to have minimal clinical implications [33]. This evolution in surgical techniques is reflected in our study, where FESS (69%) was the most common approach, particularly in recent years (2019 and later), whereas the Caldwell-Luc procedure was mainly employed earlier. Nevertheless, FESS cannot address OAFs, which require additional intra-oral surgical approaches. Small OACs (less than 5 mm) can typically close on their own after the formation of a blood clot, while larger defects or those present for more than three weeks often require surgical intervention [35]. For small OACs that occur immediately after implant retrieval, applying a collagen plug and suturing the mucosa may be adequate. In contrast, larger defects or chronic communications that have epithelialized (OAFs) will likely necessitate local flaps, such as buccal advancement flaps, buccal fat pad flaps, palatal flaps, and possibly bone grafts and membranes, depending on the size and location of the OAF [36]. A multidisciplinary approach involving ENT and maxillofacial teams is essential in these cases. If an OAF is present and FESS is indicated due to clinical or radiological signs of sinusitis, it is advisable to address both conditions in the same surgical procedure. If an OAF exists without the requirement for sinus drainage, it can be treated during a transoral implant retrieval, or if removal is done via FESS, it is preferable to do it simultaneously for the patient’s convenience.
Treatment algorithm
Our proposed treatment algorithm, based on the data presented in our study, depicted in Fig. 4.
Fig. 4. Proposed treatment protocol for patient diagnosed with migrated implant to the maxillary sinus (OMC– Osteo-meatal complex, OAF– Oroantral fistula)
A comprehensive initial assessment is crucial, encompassing a detailed medical history and clinical examination to identify dental or nasal signs/symptoms (pain, pus, nasal obstruction, swelling, headache, and OAF presence). 3D Imaging, is then necessary to visualize implant location, membrane thickness, sinus opacification, and OMC obstruction. Treatment decisions are guided by clinical presentation, while immediate implant removal is recommended, if possible.
Asymptomatic patients and no OAF, undergo risk stratification based on patient preference, prosthetic needs, membrane thickness, and sinus opacification which warrants surgical removal - FESS preferred. High-risk patients (those requiring pre-prosthetic intervention, significant membrane thickening, and/or sinus opacification) should undergo surgical removal to mitigate long-term risks. Low-risk patients warrant close monitoring with regular imaging (6–12 months) and strict clinical follow up. If any clinical signs or symptoms arise, or if there are any changes observed in radiological imaging, an intervention is warranted.
Symptomatic patients require surgical intervention: FESS is the primary approach for sinusitis (with or without OAF), potentially combined with intraoral flaps for OAF closure. In the absence of sinusitis, but with OAF, a transoral approach or FESS (depending on implant location) is used for removal of implant, followed by fistula repair. OMC obstruction necessitates surgical intervention to restore drainage– through FESS.
Whenever a suspicion for sinusitis rise according clinical or radiological data, a referral to otolaryngologist is mandatory. In other cases, if there is no OAF, the implant may also be removed by FESS and a consultation with otolaryngologist is recommended.
We suggest that any transoral procedure be conducted by a maxillofacial surgeon or a highly skilled dental surgeon who are experienced with these types of procedures. Additionally, FESS should be carried out by an otolaryngologist.
Postoperative management involves close monitoring for complications, antibiotic prophylaxis where appropriate, and patient education.
Strengths and limitations
A significant strength of this study is its multicenter approach, which allows for a more comprehensive analysis of 32 cases over a 13-year period, providing valuable insights into the etiology and management of implant displacement into the maxillary sinus. The proposed treatment protocol, informed by a thorough examination of diverse clinical scenarios, offers a systematic approach that can enhance the standard of care for practitioners addressing this complication.
Despite its contribution to understanding dental implant displacement, this study has some limitations. The retrospective design may introduce selection bias, as it relies on available medical records, potentially omitting critical data from patients who did not seek treatment.
Conclusion
The study highlights the increasing prevalence of implant displacement to maxillary sinus, emphasizing the need for improved preventative strategies and evidence-based treatment protocols. Analysis of 32 cases revealed that displacement can occur during implant placement, exposure, or osseointegration, often leading to sinusitis and OAF.
A proposed treatment algorithm, guided by the presence or absence of symptoms and sinusitis, advocates for surgical intervention (FESS being the preferred method) in most cases, while emphasizing the importance of thorough initial assessment, including advanced imaging, and careful consideration of individual patient factors.
Although this retrospective study cannot establish definitive causality, the results underscore the need for improved surgical techniques and meticulous pre-operative planning to reduce the incidence of this complication and to guide clinicians towards optimal management strategies. Further prospective studies are warranted to validate the proposed algorithm and assess the long-term outcomes of different treatment modalities.
Table 1. Study cohort data and characteristics N ageGenderASAsmokerAdmission reasonTiming of implant displacementImmediate implantSinus elevationOAFMethod of OAF closureostium obstructionsinusitismethod of implant removalTime to removalYear of treatmentSinus membrane thickeningPus dischargepaincomplicationsImplant length (mm)sinus floor thickness (mm)165M20Pre prostheticNANA00010FESS1 year >20231000NA2.4270F20Dentist referral after displacementImplantationNA00001FESS1 year <2022111011.51357M31Coincidental findingNANA00011FESS1 year <20231100101.8433F10Dentist referral after displacementImplantation100010FESS1 year >2022100062.5567F10Dental symptomsExposureNA00011FESS1 year <2020110011.52.9665M21Pre prostheticNANA00011FESS1 year <20201000162.2759M10Dental symptomsNANA01BFP11CALDWELL-LUC1 year <20151100NANA871M21Pre prostheticNANA00011FESS1 year <2019110082.9982M20Dental symptomsNANA01BFP00FESS1 year <2021111011.51.51054F20Dentist referral after displacementImplantationNA01BAF11FESS1 year >2020101013.53.11168M20Rhinologic symptomsImplantation111BFP11FESS1 year >20201110132.91256M20Rhinologic symptomsNA001BFP11FESS1 year <20221100NA3.31374M30Pre prostheticNA001BFP11FESS1 year >2023100083.51456F21Pre prostheticImplantation001BAF + PALATAL FLAP00FESS1 year <2018100OAF82.41554F11Dentist referral after displacementExposure001BAF00TRANSCRESTAL1 year >20211000NANA1668M10Pre prostheticNA000011FESS1 year >20211110101.81719F10Rhinologic symptomsImplantation101BAF00TRANS CRESTAL1 year >20191000NANA1857M10Rhinologic symptomsExposureNA00000FESS1 year >20181100NA2.51986M30Dental symptomsNANA11BFP00FESS1 year >20180000101.22085M20Pre prostheticNANA10BAF00LATERAL APPROACH1 year >202310001012155M11Dentist referral after displacementNA001000CALDWELL-LUC1 year >20111100NANA2268M30Pre prostheticNA011BAF10CALDWELL-LUC1 year >20111100NANA2336F10Rhinologic symptomsImplantation000001FESS1 year >20231110NA12485M20Dentist referral after displacementOsseointegration period010000LATERAL APPROACH1 year >201010001012556M21Rhinologic symptomsNANA10011FESS1 year <20221100132.52674M20Rhinologic symptomsNANA10011FESS1 year <2023111081.52761F10Dentist referral after displacementExposureNA10001FESS1 year >20231010103.62863F10Coincidental findingNANA00000No treatmentNo treatment neededNA00001032944F31Coincidental findingOsseointegration period000000CALDWELL-LUC1 year >201510001323061F31Dentist referral after displacementOsseointegration period010000No treatmentNo treatment neededNA000011.513179F10Rhinologic symptomsNANA00011SPONTANEOUS - SNEEZENo treatment neededNA111011.523265F21Pre prostheticNA000000LATERAL APPROACH1 year <20230000133*OAF– Ora-antral fistula; **BFP– Buccal fat pad; ***BAF– Buccal advancement flap
Table 2. Implant removal method of total cohortModality N %Fess2063Caldwell luc413Lateral approach39Trans crestal26No treatment26Spontaneous - Sneezing13 TOTAL
32
100
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1González-García A, González-García J, Diniz-Freitas M, García-García A, Bullón P. Accidental displacement and migration of endosseous implants into adjacent craniofacial structures: A review and update. Med Oral Patol Oral Cir Bucal. 2012;17(5).10.4317/medoral.18032 PMC 348252022549685 · doi ↗ · pubmed ↗
- 2Brescia G, Fusetti S, Apolloni F, Marioni G, Saia G. Displaced Dental Materials in the Maxillary Sinus: An Original Series. Analysis and Definition of a Surgical Decision-Making Process. Annals of Otology, Rhinology and Laryngology. 2019;128(3):177–83.10.1177/000348941881289830461291 · doi ↗ · pubmed ↗
- 3Quiney RE, Brimble E, Hodge M. Maxillary sinusitis from dental osseointegrated implants. J Laryngol Otol [Internet]. 1990 [cited 2025 Mar 24];104(4):333–4. Available from: https://pubmed.ncbi.nlm.nih.gov/2370457/10.1017/s 00222151001126302370457 · doi ↗ · pubmed ↗
- 4Felisati G, Lozza P, Chiapasco M, Borloni R. Endoscopic removal of an unusual foreign body in the sphenoid sinus: an oral implant. Clin Oral Implants Res [Internet]. 2007 Dec [cited 2025 Mar 24];18(6):776–80. Available from: https://pubmed.ncbi.nlm.nih.gov/17868385/10.1111/j.1600-0501.2007.01409.x 17868385 · doi ↗ · pubmed ↗
- 5Laureti M, Ferrigno N, Rosella D, Papi P, Mencio F, De Angelis F et al. Unusual case of osseointegrated dental implant migration into maxillary sinus removed 12 years after insertion. Case Rep Dent. 2017;2017.10.1155/2017/9634672 PMC 536837428392949 · doi ↗ · pubmed ↗
- 6Hamdoon Z, Mahmood N, Talaat W, Sattar AA, Naeim K, Qais A et al. Evaluation of different surgical approaches to remove dental implants from the maxillary sinus. Sci Rep. 2021;11(1).10.1038/s 41598-021-83721-z PMC 790480933627752 · doi ↗ · pubmed ↗
- 7Varol A, Türker N, Göker K, Basa S. Endoscopic retrieval of dental implants from the maxillary sinus. Int J Oral Maxillofac Implants [Internet]. 2006 [cited 2025 Mar 24];21(5):801–4. Available from: https://pubmed.ncbi.nlm.nih.gov/17066644/17066644 · pubmed ↗
- 8Ridaura-Ruiz L, Figueiredo R, Guinot-Moya R, Piñera-Penalva M, Sanchez-Garcés MA, Valmaseda-Castellón E et al. Accidental displacement of dental implants into the maxillary sinus: A report of nine cases. Clin Implant Dent Relat Res. 2009;11(SUPPL. 1).10.1111/j.1708-8208.2009.00175.x 19438955 · doi ↗ · pubmed ↗