Isoniazid-resistant TB and associated factors in Ethiopia
S. Moga, T. Abebe, K. Bobosha, A. Alemu, G. Diriba, K.R.V. Harrington, R.H. Lyles, H.M. Blumberg, R.R. Kempker

TL;DR
This study finds that isoniazid-resistant TB is common in Ethiopia and suggests screening all TB cases for drug resistance.
Contribution
The study identifies the prevalence and regional variation of isoniazid-resistant TB in Ethiopia and recommends baseline screening for drug resistance.
Findings
The prevalence of Hr-TB in Ethiopia is 4.1%, higher than MDR-TB at 1.9%.
Hr-TB is more common in the Amhara region and Addis Ababa, with higher rates among older individuals.
Hr-TB cases are more likely to have resistance to ethambutol, streptomycin, and pyrazinamide.
Abstract
Isoniazid-resistant, rifampicin-susceptible Mycobacterium tuberculosis (Hr-TB) is the most common form of drug-resistant TB (DR-TB). We investigated the prevalence of and risk factors for Hr-TB in Ethiopia. A cross-sectional study was conducted to determine the magnitude of Hr-TB, and to compare characteristics of persons with Hr-TB to those with multidrug-resistant TB (MDR-TB) and INH/RMP-susceptible TB identified during the National Drug Resistance Survey from 2017–2019. Among 1927 M. tuberculosis isolates recovered from persons with pulmonary TB, the prevalence of Hr-TB was 4.1% (95% CI 3.2-5.1), whereas the prevalence of MDR-TB was 1.9%. (95% CI 1.3–2.6). Unlike MDR-TB, the occurrence of Hr-TB did not differ significantly between new and previously treated TB cases (P = 0.67). The prevalence of Hr-TB cases was high in the Amhara (8.0%, 95% CI 4.8–12.5) region and Addis Ababa…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE
FIGURE| Characteristics | All cases (n=1927) n (%) | Hr-TB (N = 79) n (%) | INH/RMP-S TB (N = 1,807) n (%) | OR (95% CI) multivariable stepwise regression | ||
|---|---|---|---|---|---|---|
| Sex | Male | 1,103 (57.2) | 50 (63.3) | 1,031 (57.1) | .272 | |
| Female | 824 (42.8) | 29 (36.7) | 776 (42.9) | |||
| Age (Years) | Mean (±SD) | 30.0 ±13.4 | 33.1±15.6 | 29.9±13.3 | 1.02 (1.01–1.04) | 0.01 |
| Residence | Rural | 1211 (62.8) | 50 (63.3) | 1,141 (63.1) | .979 | |
| Urban | 716 (37.2) | 29 (36.7) | 666 (36.9) | |||
| Regional state | Oromia | 666 (34.6) | 25 (31.6) | 633 (35.0) | 2.32 (0.80, 6.81) | .004 |
| Amhara | 237 (12.3) | 19 (24.1) | 217 (12.0) | 5.54 (1.83, 16.75) | ||
| SNNPR | 637 (33.1) | 21 (26.6) | 600 (33.2) | 2.12 (0.72, 6.30) | ||
| Addis Ababa | 141 (7.3) | 10 (12.7) | 124 (6.9) | 4.05 (1.23, 13.27) | ||
| Others | 246 (12.8) | 4 (5.1) | 233 (12.9) | Ref | ||
| Education status | Primary | 731 (37.9) | 34 (43.0) | 635 (35.1) | 2.29 (1.27, 4.14) | 0.02 |
| Secondary & higher | 688 (35.7) | 21 (26.6) | 475 (26.3) | 1.82 (0.93-3.56) | ||
| Illiterate | 508 (26.4) | 24 (30.4) | 697 (38.6) | Ref | ||
| Household family size (number) | ≤ 5 | 1,318 (68.5) | 53 (67.1) | 1,239 (68.6) | .782 | |
| >5 | 607 (31.5) | 26 (32.9) | 568 (31.4) | |||
| TB treatment history | New | 1,744 (90.5) | 71 (89.9) | 1,649 (91.3) | .671 | |
| Previously treated | 183 (9.5) | 8 (10.1) | 158 (8.7) | |||
| HIV status | Reactive | 142 (7.4) | 6 (7.6) | 130 (7.2) | .858 | |
| Non-reactive | 1,766 (91.7) | 71 (89.9) | 1,663 (92.0) | |||
| Unknown | 19 (0.9) | 2 (2.5) | 14 (0.8) | |||
| Current smoker | Yes | 139 (7.2) | 5 (6.3) | 134 (7.4) | .718 | |
| No | 1,788 (92.8) | 74 (93.7) | 1,673 (92.6) | |||
| Previous smoker | Yes | 147 (7.6) | 6 (7.6) | 138 (7.6) | .989 | |
| No | 1,780 (92.4) | 73 (92.4) | 1,669 (92.4) | |||
| History of incarceration | Yes | 65 (3.4) | 3 (3.8) | 59 (3.3) | .743 | |
| No | 1,862 (96.6) | 76 (96.2) | 1,748 (96.7) | |||
| Chewing khat | Yes | 340 (17.6) | 8 (10.1) | 323 (17.9) | .076 | |
| No | 1,587 (82.4) | 71 (89.9) | 1,484 (82.1) | |||
| Use of IPT | Yes | 31 (1.6) | 2 (2.5) | 27 (1.5) | .392 | |
| No | 774 (40.2) | 34 (43.0) | 717 (39.7) | |||
| Unknown | 1,122 (58.2) | 43 (54.4) | 1,063 (58.8) | |||
| History of contact with TB | Yes | 553 (28.7) | 18 (22.8) | 524 (29.0) | .232 | |
| No | 1,374 (71.3) | 61 (77.2) | 1,283 (71.0) | |||
| History of contact with MDR-TB | Yes | 22 (1.1) | 1 (1.3) | 19 (1.1) | .577 | |
| No | 1,905 (98.9) | 78 (98.7) | 1,788 (98.9) |
| Drugs (total number of pDST performed) | Phenotypic DST result | Hr-TB n (%) | INH/RMP-S TB n (%) | Estimated odds ratio (95% CI) | |
|---|---|---|---|---|---|
| Streptomycin (n = 1,535) | Resistant | 27 (44.3) | 30 (2.0) | 38.2 (20.5–71.1) | <.0001 |
| Susceptible | 34 (55.7) | 1,444 (98.0) | |||
| Ethambutol (n = 1,535) | Resistant | 5 (8.2) | 11 (0.7) | 11.9 (4.0–35.3) | <.0001 |
| Susceptible | 56 (91.8) | 1,463 (99.3) | |||
| Pyrazinamide (n = 1,444) | Resistant | 5 (8.3) | 17 (1.2) | 7.3 (2.6–20.5) | <.0001 |
| Susceptible | 55 (91.7) | 1,367 (98.8) |
| Characteristics | MDR-TB (N = 36) n (%) | INH/RMP-S TB (N = 1807) n (%) | OR (95% CI) multivariable stepwise regression | ||
|---|---|---|---|---|---|
| Sex | Male | 20 | 1,031 (57.1) | .857 | |
| Female | 16 | 776 (42.9) | |||
| Age (Years) | Mean | 30.7 | 29.9±13.2 | .697 | |
| Residence | Rural | 19 (52.8) | 1,141 (63.1) | .202 | |
| Urban | 17 (47.2) | 666 (36.9) | |||
| Regional state | Oromia | 6 (16.7) | 633 (35.0) | 0.29 (0.10- 0.84) | .011 |
| Amhara | 1 (2.8) | 217 (12.0) | 0.13 (0.02- 1.02) | ||
| SNNPR | 15 (41.7) | 600 (33.2) | 0.67 (0.28- 1.59) | ||
| Addis Ababa | 5 (13.9) | 124 (6.9) | 1.15 (0.37- 3.63) | ||
| Others | 9 (25.0) | 233 (12.9) | Ref | ||
| Education status | Illiterate | 9 (25.0) | 697 (38.6) | .204 | |
| Primary | 17 (47.2) | 635 (35.1) | |||
| Secondary & higher | 10 (27.8) | 475 (26.3) | |||
| Household family size (number) | ≤ 5 | 23 (63.9) | 1,239 (68.6) | .55 | |
| >5 | 13 (36.1) | 568 (31.4) | |||
| TB treatment history | New | 21 (58.3) | 1,649 (91.3) | 6.66 (3.33-13.32) | <0.001 |
| Previously treated | 15 (41.7) | 158 (8.7) | |||
| HIV status | Reactive | 5 (13.9) | 130 (7.2) | .115 | |
| Non-reactive | 30 (83.3) | 1,663 (92.0) | |||
| Unknown | 1 (2.8) | 14 (0.8) | |||
| Current smoker | Yes | 0 (0.0) | 134 (7.4) | 0.09 | |
| No | 36 (100) | 1,673 (92.6) | |||
| Previous smoker | Yes | 3 (8.3) | 138 (7.6) | .752 | |
| No | 33 (91.7) | 1,669 (92.4) | |||
| History of incarceration | Yes | 2 (5.6) | 59 (3.3) | .336 | |
| No | 34 (94.4) | 1,748 (96.7) | |||
| Chewing khat | Yes | 9 (25.0) | 323 (17.9) | .271 | |
| No | 27 (75.0) | 1,484 (82.1) | |||
| Use of IPT | Yes | 2 (5.6) | 27 (1.5) | .187 | |
| No | 19 (52.8) | 717 (39.7) | |||
| Unknown | 15 (41.7) | 1,063 (58.8) | |||
| History of contact with TB | Yes | 10 (27.8) | 524 (29.0) | .873 | |
| No | 26 (72.2) | 1,283 (71.0) | |||
| History of contact with MDR-TB | Yes | 2 (5.6) | 19 (1.1) | 4.77 (0.94- 24.25) | 0.06 |
| No | 34 (94.4) | 1,788 (98.9) |
- —National Institutes of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Diagnosis and treatment of tuberculosis · Pneumocystis jirovecii pneumonia detection and treatment
Drug-resistant TB (DR-TB) remains a significant challenge to TB prevention and control.^1^ Isoniazid (INH) and rifampicin (RMP) are the two most important first-line drugs for the treatment of active TB disease. In 2023, INH-resistant TB (Hr-TB), which is defined as Mycobacterium tuberculosis (Mtb) strains resistant to INH but susceptible to RMP, occurred in an estimated one million persons with TB, accounting for 9.3% of estimated TB cases globally.^2^ Hr-TB poses a significant public health challenge as it diminishes the efficacy of first-line anti-TB treatments and increases the risk of progression to multidrug-resistant TB (MDR-TB), a form of TB that is resistant to RMP and INH.^3^ A systematic review showed that individuals with Hr-TB experience notably higher rates of treatment failure (11% vs 1%), TB relapse (10% vs 5%), and acquisition of further drug resistance during treatment (3.6% vs 0.6%) compared with persons with pan-susceptible TB.^3^ Moreover, a genomic study has revealed that the development of INH resistance is often the initial step towards acquiring additional resistance to other anti-TB drugs, including RMP and second-line drugs.^4^
Ethiopia is among 30 countries globally designated as high-burden TB and TB-HIV co-infection countries by the WHO.^2^ The COVID-19 pandemic has greatly impacted TB incidence and mortality, and reversed a decade-long trend of decline. In 2023, an incidence of 146 cases per 100,000 persons was reported, marking an increase compared to previous consecutive years.^2^ Although there are substantial data on MDR-TB, data describing Hr-TB remains more limited, particularly around identifying risk factors for Hr-TB in Ethiopia. The detection of INH resistance has historically received low priority, resulting in Hr-TB often being treated empirically with first-line TB drugs.^5^ This practice contributes to suboptimal treatment outcomes, prolonged infectiousness and emergence of MDR-TB.^3^ Given the rising global prevalence of Hr-TB and its potential to progress to MDR-TB ^3^, identifying risk factors associated with Hr-TB is crucial for developing effective TB control strategies. We therefore set out to assess the prevalence of Hr-TB and identify risk factors associated with Hr-TB by leveraging data from the National Drug Resistance Survey (DRS) conducted in Ethiopia from 2017–2019.
METHODS
We conducted a population-based cross-sectional study using data from the Ethiopian National DRS carried out by the Ethiopian Public Health Institute (EPHI) from August 2017 to January 2019 at selected health facilities across all regional states. A probability-proportional to size (PPS) cluster sampling method was used to select health facilities where persons with TB seek care and were diagnosed using either the Xpert MTB/RIF assay or acid-fast bacilli (AFB) microscopy. A health facility reporting ≥30 smear-positive pulmonary TB cases annually formed its own cluster, while those with fewer cases were grouped into district-level clusters. A total of 1,237 clusters were derived from 4,503 health facilities available during the DRS. Using PPS, 67 clusters encompassing 217 health facilities were selected to recruit 30 cases per cluster. The sample size was determined to include 2,010 newly diagnosed TB cases, and all previously treated cases registered for treatment during the study period at selected health facilities. During the DRS, 2,560 bacteriologically confirmed new and previously treated pulmonary TB cases registered for treatment were consecutively enrolled in selected health centers after obtaining written informed consent or assent. Patients who had received treatment for more than one week at the time of enrolment and patients with extra-pulmonary TB were excluded. Socio-demographic, clinical, and behavioural data was collected at enrollment through interview and review of medical records. After enrollment, the Xpert MTB/RIF assay was performed for confirmation of TB and for determination of RMP resistance. A morning sputum sample was collected at health facilities and was transported to the nearest TB culture laboratories available at Regional Reference Laboratories (RRLs) and Referral Hospitals for culture isolation of Mtb using Löwenstein-Jensen medium and the BACTEC mycobacteria growth indicator tube (MGIT) 960 system (Becton Dickinson, Sparks, Maryland, USA).
Culture-positive Mtb isolates were tested with phenotypic drug susceptibility testing (DST) at the EPHI National TB Reference Laboratory (NTRL) located in Addis Ababa, Ethiopia. Phenotypic DST was performed using the BACTEC MGIT 960 system according to WHO-recommended critical concentrations of 0.1µg/ml for INH, 1.0µg/ml for RMP, 1.0µg/ml for streptomycin (SM), 5µg/ml for ethambutol (EMB), and 100µg/ml for pyrazinamide (PZA).^6^ Whole genome sequencing (WGS) was also performed on culture isolates from patients with MDR-TB, Hr-TB, and selected INH/RIF-susceptible Mtb isolates to confirm DST results. Resistance was interpreted based on the 2023 WHO catalogue of mutations associated with drug resistance.^7^ In cases where phenotypic DST was not available, a GenoType MTBDRplus line probe assay (LPA) was utilized to detect additional INH and RMP resistance in smear-positive sediments.
Participant characteristics were summarised descriptively, overall and separately for the groups presenting with Hr-TB, MDR-TB, and INH/RMP-susceptible TB. Distributions of risk factors among the Hr-TB were compared against those in the INH/RMP-susceptible and the MDR-TB groups, using chi-square tests for categorical variables and two sample t tests for continuous variables. In instances where categorical variables had small cell counts, the Fisher’s exact test was used in place of chi-squared test. Stepwise logistic regression with entry and retention significance levels of 0.20 was applied to obtain parsimonious multivariable models for Hr-TB and MDR-TB status, using the set of risk factors that were examined univariately to form the list of candidate predictors. All statistical analyses were performed using the SAS statistical software package (SAS Institute, Inc.). Cases with RMP-resistant but INH-susceptible TB including RMP monoresistant TB were excluded from risk factor analysis. INH/RMP-susceptible cases include cases susceptible to both INH and RMP.
This study was reviewed and approved by the Institutional Review Boards (IRBs) of the Ethiopian Public Health Institute (EPHI-IRB-258-2020) and Addis Ababa University (041/21/DMIP). Because the study involved secondary analysis of DRS data, a waiver of individual informed consent was obtained from the IRBs. Informed consent was collected from participants enrolled in the primary DRS.
RESULTS
Characteristics of study participants
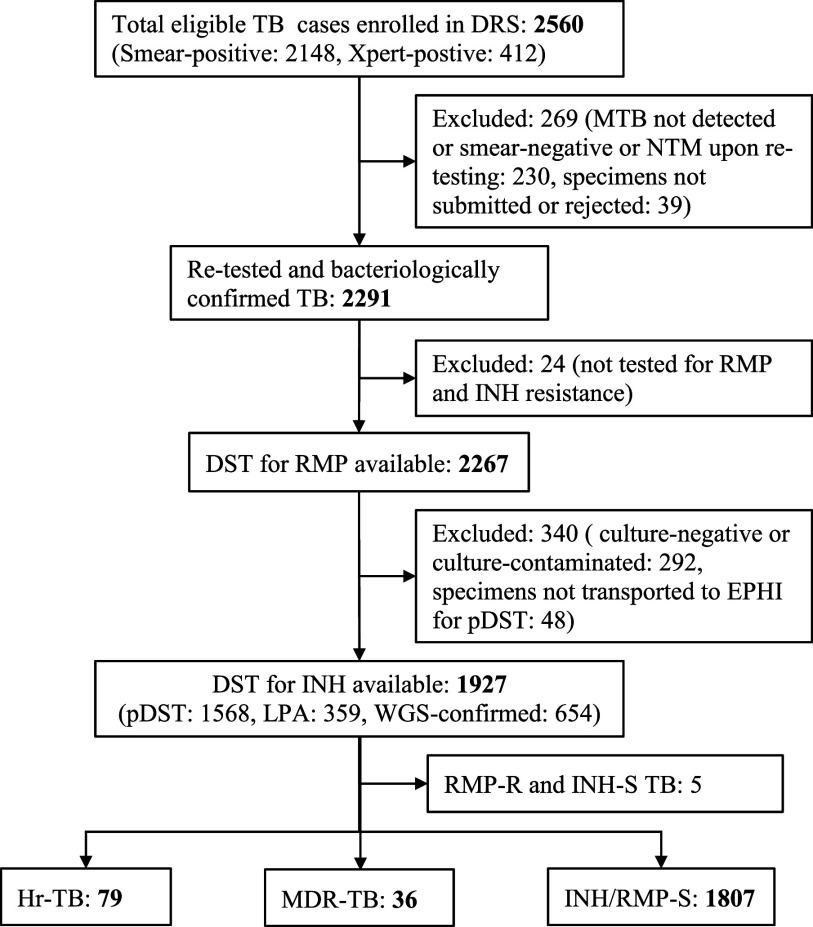
There were 2,560 pulmonary TB cases enrolled in the DRS; 2,148 cases were diagnosed through AFB smear-positive results and 412 cases by positive Xpert MTB/RIF results. Among these TB cases, 1,927 (75.3%) had DST results for at least RMP and INH. The remaining 633 cases were excluded from analyses due to lack of DST data for INH. The flow chart outlining the enrolment process in this study is shown in the Figure. Among 1927 participants, more than half (57.2%) were male, with a mean age of 30.0 years (standard deviation 13.4, range 2–99). More than one-third of cases reported no formal education (37.9%) and lived in an urban area (37.2%). Thirty-one (1.6%) participants had a prior history of taking INH preventive therapy. Additionally, 183 (9.5%) participants had a history of previous TB treatment. The demographic and clinical characteristics of study participants are presented in Table 1. Of the 1,927 Mtb isolates analysed, 79 (4.1%) were classified as Hr-TB. Among 79 Hr-TB cases, 61 were identified through phenotypic DST, 16 were detected using LPA, and 2 were additionally confirmed by WGS. The highest proportions of Hr-TB cases were observed in the Amhara (8.1%) regions and Addis Ababa (7.5%) (Table 1). Additionally, 36 (1.9%) isolates were identified as MDR-TB and 5 (0.3%) isolates exhibited RMP-resistant but INH-susceptible TB. Higher prevalence of MDR-TB (n = 5, 3.9%) was recorded in Addis Ababa, while only one (0.5%) case of MDR-TB was reported from Amhara region (Table 1). Overall, 115 (5.9%) isolates demonstrated INH resistance, including those that were RMP-susceptible and RMP-resistant. In contrast, INH/RMP-susceptible TB accounted for 93.8% (1807) of isolates.
Flow chart of participant enrolment and isoniazid resistance pattern. DRS = drug resistance survey; NTM = nontuberculous mycobacteria; RMP = rifampicin; INH = isoniazid, DST = drug susceptibility testing; LPA = line probe assay: EPHI = Ethiopian Public Health Institute: RMP-R and INH-S TB= rifampicin resistant and isoniazid susceptible TB; Hr-TB = isoniazid-resistant, rifampicin-susceptible TB; MDR-TB = multidrug-resistant TB; INH/RMP-S TB = isoniazid and rifampicin susceptible TB
Drug resistance profiles of Hr-TB and Isoniazid/rifampicin-susceptible TB
Phenotypic DST was performed for 1,568 of Mtb culture isolates. Among these, 61 were Hr-TB phenotypes, 1,474 were INH/RMP-susceptible TB, and the remaining 33 were either MDR-TB or RMP-resistant TB. A comparison between the DST patterns of Hr-TB and IHN/RMP-susceptible isolates for SM, EMB, and PZA are shown in Table 3. Among the 61 Hr-TB phenotypes, 30 exhibited additional resistance to ≥1 first-line anti-TB drug, whereas 31 demonstrated monoresistance to INH. Additional resistance was observed for SM (n = 27), for PZA (n = 5), and for EMB (n = 5). Two Hr-TB isolates were resistant to both PZA and EMB. In contrast, among INH/RMP-susceptible isolates, we observed resistance to SM (n = 30), PZA (n = 17), and EMB (n = 11). We found that Hr-TB cases were significantly associated with increased resistance to SM, EMB, and PZA compared to INH/RMP-susceptible strains (P < 0.0001).
Factors associated with Hr-TB and MDR-TB
Risk factors for Hr-TB in multivariable analysis included increasing age in years (aOR 1.02, 95% CI 1.01–1.04), primary level of education (aOR 2.29, 95% CI 1.27–4.14), and residence in Addis Ababa (aOR 4.05, 95% CI 1.23–13.27) and the Amhara region (aOR 5.54, 95% CI 1.83–16.75) (Table 1). The primary risk factor for MDR-TB was previous TB treatment (aOR 6.66, 95% CI 3.33–13.32), see Table 2, with marginal adjusted associations identified between MDR-TB and variables capturing confirmed prior MDR-TB contact and region of residence.
DISCUSSION
In this population-based study, the overall prevalence of Hr-TB was 4.1%. This prevalence is notably lower than the reported global estimate of Hr-TB at 9.3 %.^2^ However, the prevalence of Hr-TB represents a large proportion of the DR-TB cases in Ethiopia, particularly when compared to the relatively low rate of RMP-resistant TB and MDR-TB.^2^ Notably, our findings suggest a decline in the overall Hr-TB prevalence compared to 6.1% (95% CI 4.5–8.0) prevalence from the first DRS conducted in Ethiopia from 2003–2005.^8^ This reduction may highlight the impact of the TB control program in decentralization of rapid molecular diagnostics for the detection of DR-TB at primary health care level and high treatment success rate among DR-TB cases compared to global estimates. Ethiopia has seen a consistent decline in DR-TB prevalence, resulting in its removal from of the list of 30 high MDR-TB burden countries in 2021.^9^
Prior studies in Ethiopia have reported Hr-TB prevalence ranging from 8.9% to 9.3% among pulmonary TB cases.^10,11^ However, these studies were small in size and were conducted in general and tertiary hospitals that typically manage more complicated DR-TB cases, which may have led to an overestimation of Hr-TB prevalence. Previous work has described that studies with limited sample sizes based in specific institutions can inflate reported MDR-TB prevalence.^12^ Moreover, the pre-2020 diagnostic algorithm that recommended DST specifically for patients at high risk of MDR-TB could result in inflation of DR-TB in those studies. A strength of our findings includes the use of the population-based DRS and performing DST for bacteriologically confirmed TB cases, as this is likely a better representative sample to estimate the true prevalence of Hr-TB in Ethiopia. This underscores the need for comprehensive national surveys to accurately assess DR-TB burden in low and middle income countries including Ethiopia.
In our study, the prevalence of Hr-TB was 4.1% among newly diagnosed TB cases and 4.4% among previously treated TB cases. These estimates are lower than Hr-TB prevalence among new and previously treated TB patients reported in both the first DRS and global estimates, but they align with recent findings from Kenya and Eritrea.^8,13–15^ A history of previous anti-TB treatment is a well-established risk factor for developing MDR-TB in Ethiopia.^12^ Consistent with this study, the previous surveys indicate that patients with previous history of anti-TB treatment are at high risk for MDR-TB compared to new TB cases.^8^ However, it is noteworthy that Hr-TB was not associated with previous treatment history in our findings. This suggests the need for routine screening for INH resistance regardless of a patient’s previous treatment history.
We found an increase in the proportion of Hr-TB with increasing age. This could be due to increase in risk of TB disease with increasing age.^2^ A study showed that INH monoresistance tends to occur in persons aged 15–64 years.^16^ In contrast, another study highlighted a lower odds of INH monoresistant TB among older age groups.^17^ Although other studies inconsistently reported diabetes,^18^ non-diabetes,^19^ female sex,^20^ male sex, homelessness,^17^ use of preventive therapy, previous history of treatment ^21^ as independent risk factors associated Hr-TB, few studies also failed to demonstrate any significant predictors for Hr-TB.^22^ These works further reveal that factors associated with developing Hr-TB may vary by settings and more work is needed to gain a better understanding of these risks from different clinical and epidemiological perspectives. We also observed that Hr-TB more commonly occurred in Addis Ababa and the Amhara region, compared to other regional states in Ethiopia. Geographic variation in Hr-TB prevalence has been observed in other studies.^20,23^ This may imply local spread of Hr-TB and highlight the potential impact of setting-specific interventions and importance of real time molecular information to better identify and respond to local outbreaks.
We found association of Hr-TB with resistance to other first line drugs including EMB and PZA. This finding has raised important questions about which drug resistance appears first in the evolution of resistance. The most comprehensive genomic study of 5,310 Mtb isolates collected from five continents revealed that INH resistance emerge prior to RMP resistance and all other first-line drugs.^4^ Thus high proportion of resistance to first-line drugs observed among Hr-TB in our and other studies could partly explain the high rate of treatment failure and relapse rate among Hr-TB, compared to INH/RMP-susceptible TB.^3^ Moreover, a modelling study has indicated that INH resistance could even occur in an estimated 11% of latent TB infection (LTBI).^24^ This highlights that Hr-TB could emerge in TB patients without exposure to well-known predictors to DR-TB. This also implies that early detection of Hr-TB could prevent emergence of not only MDR-TB but also resistance to other first line TB drugs.
The Ethiopian national TB guidelines recommend rapid molecular testing for INH resistance among new and previously treated pulmonary TB cases that remain smear-positive at the second or later month of first line anti-TB drugs, to all previously treated cases at baseline, and to contacts of known Hr-TB cases.^5^ However, our data poses questions around whether targeted testing strategies or testing all TB patients for INH resistance is preferable. As we did not find any individual-level predictors compelling for targeted testing, our results suggest that a universal approach for INH-resistant screening should be considered. Consistently, the review of multi-country drug resistance data reported to WHO highlighted the need for INH DST for all bacteriologically confirmed TB cases at baseline prior to treatment.^23^ Moreover, rapid detection of RMP and INH resistance at moment of diagnosis has been shown to be cost effective and improve public health outcome.^25^ This is could enable the program to use levofloxacin in the treatment regimen and prevent worse treatment outcomes among Hr-TB cases.^26^
A limitation to this study is that certain cases were excluded because of lack of a culture growth or lack of DST for INH. However, our use of a national survey presented an opportunity to analyze risk factors and estimate the magnitude of INH that can be generalizable to overall TB/DR-TB patients.
CONCLUSIONS
The prevalence of Hr-TB in Ethiopia is twice as high as MDR-TB prevalence, but notably lower than the global prevalence of Hr-TB. The prevalence of Hr-TB increased with advancing age and varied by regional states in Ethiopia with the highest rates in Addis Ababa and the Amhara region. We recommend baseline screening for Hr-TB among all bacteriologically confirmed TB cases given the impact on clinical care and increased resistance to other first line drugs. Expanding our current understanding of Hr-TB is important to guide policy makers and clinicians regarding the application of rapid molecular DST for screening of Hr-TB cases.
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Farhat M Drug-resistant tuberculosis: a persistent global health concern. Nat Rev Microbiol. 2024;22(10):617-635.38519618 10.1038/s 41579-024-01025-1 · doi ↗ · pubmed ↗
- 2World Health Organisation. Global tuberculosis Report 2024. Geneva, Switzerland: WHO, 2024.
- 3Gegia M Treatment of isoniazid-resistant tuberculosis with first-line drugs: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(2):223-234.27865891 10.1016/S 1473-3099(16)30407-8 · doi ↗ · pubmed ↗
- 4Manson AL Genomic analysis of globally diverse Mycobacterium tuberculosis strains provides insights into the emergence and spread of multidrug resistance. Nat Genet. 2017;49(3):395-402.28092681 10.1038/ng.3767 PMC 5402762 · doi ↗ · pubmed ↗
- 5Ethiopian Ministry of Health. Guidelines for Clinical and Programmatic Management of TB, TB/ HIV, DR-TB and Leprosy in Ethiopia. 7th ed. Addis Ababa, Ethiopia: Ministry of Health; 2021.
- 6Mycobacteriology Laboratory Manual. 1st ed. Global Laboratory Initiative; 2014.
- 7World Health Organization. Catalogue of mutations in Mycobacterium tuberculosis complex and their association with drug resistance. 2nd ed. Geneva, Switzerland; WHO, 2023.
- 8Wright A Epidemiology of antituberculosis drug resistance 2002-07: an updated analysis of the Global Project on Anti-Tuberculosis Drug Resistance Surveillance. Lancet. 2009;373(9678):1861-1873.19375159 10.1016/S 0140-6736(09)60331-7 · doi ↗ · pubmed ↗