The association of body image with quality of life, psychological assistance and social support in neurofibromatosis type 1 patients: a cross-sectional study
Daniel Muñoz, Mercè Jodar, Laia Valls, Albert Fornieles-Deu, Elisabeth Castellanos, Ignacio Blanco

TL;DR
This study finds that body image issues, not skin severity, most strongly affect quality of life in neurofibromatosis type 1 patients, highlighting the need for psychological support.
Contribution
The study identifies body image as a critical but underemphasized factor affecting quality of life in neurofibromatosis type 1 patients.
Findings
Body image impairments significantly reduce quality of life in neurofibromatosis type 1 patients.
Patients with body image concerns are more likely to seek psychological assistance but report less social support.
Skin severity and appearance concerns do not strongly correlate with quality of life.
Abstract
Neurofibromatosis type 1 is a genetic disease with an autosomal dominant pattern. One of its clinical features is the presence of disfiguring neurofibromas. Most adults with Neurofibromatosis type 1 have visible neurofibromas depending on the severity of their skin related clinic that can affect their body image, and body image influencing psychological assistance and social support. This research explored Body image, the negative perception of the appearance of neurofibromas and skin severity in Neurofibromatosis type 1 patients; assessed its association with quality of life; and the role of social support and psychological assistance. Two hundred five patients with Neurofibromatosis type 1 (16–74 years) were included in the study. They responded to questionnaires about their quality of life, body image and other sociodemographic data. Correlations and simple and multiple regressions…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
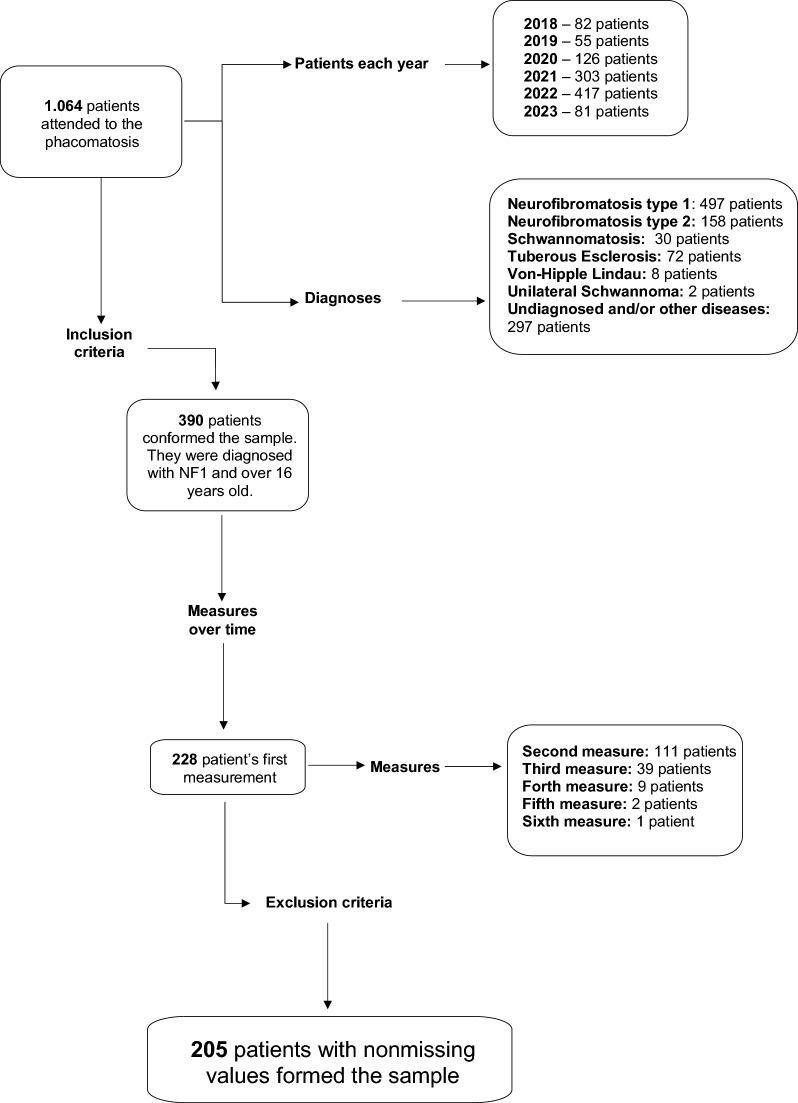 Figure 1
Figure 1- —Associació Catalana de les Neurofibromatosis
- —http://dx.doi.org/10.13039/100008666Fundació la Marató de TV3
- —http://dx.doi.org/10.13039/501100003030Agència de Gestió d'Ajuts Universitaris i de Recerca
- —http://dx.doi.org/10.13039/501100004587Instituto de Salud Carlos III
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Sport Psychology and Performance
Background
Neurofibromatosis type 1 (NF1) is a genetic disease with an autosomal dominant pattern. The incidence of this condition is 1/2000–3000, with 50% of individuals having de novo mutations [1].
The NF1 clinical manifestations consists of multiple café-au-lait macules (CALMs), which are present in 100% of children, skinfold freckling in non-sun-exposed areas (such as armpits or/and groins), Lisch nodules, scoliosis and disfiguring tumors of the nervous system (neurofibromas), specifically, plexiform neurofibromas (PN) that has a volume that increases faster than the body growth rate in some individuals [1–3]. Neurofibromas are complex tumors that arise constantly throughout life, especially in adolescence [4–6]. The majority of adults with NF1 have small neurofibromas throughout their body, and visible PN is present in 30% of patients [7].
It is important to acknowledge that skin is considered a vector of intimacy and sexuality, and when it is affected, it influences the perception of our own body [8]. The neurofibromas (PN or not) of NF1 adults may disfigure their body parts, and patients may experience body dissatisfaction because of this [7]. Therefore, in NF1, body image is affected [3, 7, 9]. Body image (BI) is a multidimensional construct that defines a variety of aspects related to an individual’s body appearance. It refers to how people perceive their own body and what attitudes and feelings people have toward their own body. It can be divided into four concepts: a) satisfaction with our body and their parts (body satisfaction), b) how one experiences and appraises their own body (body experience), c) being aware of our body (body awareness), and d) the boundaries we experience with our body parts (body boundaries). It develops during childhood and adolescence [7, 10]. Therefore, NF1 has been related to psychiatric and psychological signs such as depressive symptoms, dysfunctional coping and negative body image [6, 7, 11–13].
Despite the relevance of this topic, to date, there is no specific scale for evaluating body image in NF1 patients. The Body Image Scale (BIS) evaluates the BI for oncological patients with gynecological or breast cancer [14]. The Spanish version was adapted to the Spanish Body Image Scale (S-BIS). The scale consists of 10 items that measure different dimensions of the BI (affective, behavioral and cognitive). It has solid psychometric properties (α = 0.96) [15].
In addition to BI, patients with NF1 also report a negative impact on quality of life (QoL). Quality of life refers to the perception that individuals have about themselves and their role in life [16]. The degree and manner in which NF1 affects QoL vary greatly among individuals [11].
One of the factors that affects QoL in NF1 patients is the stigma caused by cutaneous neurofibromas [11, 12]. A greater number and wider distribution of cutaneous neurofibromas are strongly associated with poor skin-related QoL [13, 17]. Despite these findings, compelling evidence suggests that disease visibility alone does not predict general QoL [18]. In line with this, Granström et al. 2012 studied the relationship between disease visibility/severity and QoL through body image, proving that body experience mediates the link between disease visibility and poor QoL. According to Granström and colleagues adult NF1 patients expressing bodily insecurity/uneasiness and fewer feelings of attractiveness and self-confidence have a negative body image [7].
Building on this perspective, additional studies affirm that body image significantly affects QoL across all its subdomains [19]. Further investigation on the connections between BI, skin severity, neurofibromas and QoL will provide a better understanding of how these aspects are linked.
QoL and BI could improve with optimum interventions and social support [20]. Cognitive behavioral therapy (CBT), social skills training and psychoeducational interventions have been shown to address individuals’ negative self-perceptions and improve their psychosocial functioning [9, 13, 21, 22]. Moreover, the presence of friends, family or attempting a support group is of great importance. These relationships constitute social networks and provide experiences that may help adults overcome challenges associated with NF1 [20]. Patients actively strive to enhance their social support by employing adaptive strategies to better cope with their situation. One such strategy is positive reframing, where people emphasize the positive aspects of their lives, placing greater emphasis on their social support and evaluating it more positively [23]. Although body image is linked to psychological stress and social burden, few studies have examined BI in NF1 patients considering the evaluation of the social support and psychological assistance they need [7].
It is reasonable to hypothesize that the negative perception of the appearance of neurofibromas will correlate with increased concerns about body image (BI), and these impairments will have a more significant impact on the quality of life (QoL) of patients with neurofibromatosis type 1 (NF1) than solely evaluating the severity of skin manifestations. Additionally, due to this association, they will report increased psychological assistance and more social support. Therefore, this study aimed to explore the BI, the negative perception of the appearance of neurofibromas and the clinical skin severity of NF1 patients; assess each of these in association with quality of life; and to explore the relevance of social support and psychological assistance among NF1 patients dealing with BI concerns.
Methods
A sample of 205 patients with NF1 who attended the Spanish National Reference Center for Neurocutaneous Syndrome-Phacomatosis (CSUR) of the Germans Trias and Pujol Hospital in the province of Barcelona were included in the study. The study was approved by the Ethics Research Committee of the Germans Trias i Pujol Hospital and was conducted in accordance with the latest version of the ethical principles of the Declaration of Helsinki.
The study has a cross-sectional design. The inclusion criteria involved NF1 patients aged 16 years and older who were capable of responding to the survey questions. According to these criteria, we included all patients who visited the unit between February 2018 and May 2023 and agreed to participate in the study (Fig. 1). To ensure bias control, patients with missing data were excluded from the sample [24, 25].Fig. 1. Flow diagram illustrating the sample process applying the inclusion and exclusion criteria
All participants attended the Phacomatosis Unit of the Germans Trias and Pujol Hospital on scheduled dates to follow-up their health condition. Informed consent was provided by the participants prior to the assessment. A trained psychologist administered all the questionnaires.
Assessment
Sociodemographic data: Patients provided their gender, age, education, marital status and employment status. Age was divided into five age groups: adolescents (16–18 years), young adults (19–24), adults (25–44 years), middle-aged individuals (45–64 years) and aged individuals (65–80 years).
Psychological assistance: Was evaluated with a dichotomized question asking if they were receiving psychological assistance at the time of evaluation. The duration of the therapy, any previous psychological assessment or the perceived effectiveness were not considered.
Social Support: Social support was assessed with a dichotomized question asking whether the participants had social support. Patients who answered “Yes” were prompted to select their sources of support from six options: social networks, institutions, others, family, friends and partner. They can choose more than one source.
Modified Spanish body image scale: The modified version of the S-BIS used in the study was adjusted from the original S-BIS. S-BIS is composed of 10 items evaluating various aspects of BI in cancer patients, including affective (e.g. feeling self-conscious), behavioral (e.g. avoiding looking at one’s body) and cognitive (e.g. dissatisfaction with appearance) dimensions. Each item is rated on a four-point scale from 0 (not at all) to 3 (very much). The total score, ranges from 0 to 30, is calculated adding all items, with higher scores indicating higher BI impairments [15]. We removed items 8 and 10 because the NF1 clinic does not involve feeling the body less complete or having scars (Supplementary material 1).
Neurofibromas question (Ad. Hoc): We included a question referring to patient satisfaction with the appearance of their neurofibromas: “Have you felt unsatisfied with the way your neurofibromas look like”. It follows a Likert structure similar to the S-BIS, and their scores vary from 0 (not at all) to 3 (a lot). The S-BIS scale captures cognitive aspects of body image but does not specifically address neurofibromas, which we considered a key feature of the NF1 skin manifestations. Thus, we included this additional question to address the impact of neurofibromas on body image directly.
Skin severity: Skin severity index values ranging from 1 to 3 according to the clinical guidelines of the hospital. These grades were defined by the qualitative impact and severity of the clinical characteristics of NF1 on these patients. The clinicians of the Phacomatosis unit (dermatologist, geneticists, neurologists and genetic counselors) combine their opinions to classify them into one of these grades.
- Grade 1 or mild involvement: indicates the presence of some features of the disease, such as a café au lait spot color and few neurofibromas.
- Grade 2 or moderate involvement: There was no significant compromise to the patient’s health; there were café au lait-colored spots and a modest number of cutaneous and/or subcutaneous neurofibromas.
- Grade 3 or severe affectation: is characterized by the presence of plexiform neurofibromas and/or a significant number of cutaneous and subcutaneous neurofibromas throughout the body. These skin manifestations affect the patient’s health.
QoL was assessed with the EuroQol Quality of Life Scale (EQ-5D) [26, 27]. It consists of a descriptive system in which the individual assesses their health status in five dimensions: mobility, personal care, daily activities, pain/discomfort and anxiety/depression. Each dimension is valued at three levels of severity: without problems, with problems or moderate problems and with serious problems. The scale also includes a vertical visual analog scale (EQ-VAS), where individuals must assess their global health status, from the worst imaginable health state (0) to the best state of health imaginable (100) [28].
Statistical analysis
The statistical analysis (descriptive, bivariate and multivariate) was conducted using R version 4.2.2. Shapiro–Wilk tests were performed for each variable to evaluate the data distribution. We included means and standard deviations for quantitative variables and frequencies and percentages for qualitative variables, and we used the Mann‒Whitney U test for quantitative variables and the chi2 test for qualitative variables with gender, psychological assistance and social support. We also analyzed the S-BIS modified with the exploratory factor analysis (EFA) method [29–31]
We retrieved Spearman correlations and simple regressions with the independent variables (S-BIS modified and Neurofibromas question Ad Hoc) and the most significant covariables (social support and psychological assistance) to test their relationships with the other variables and determine whether social support and psychological assistance are associated with BI.
The multivariate analysis consisted of multiple regressions with a stepwise method to test whether QoL was related to BI. We made two blocks: the first one contained all sociodemographic variables (gender, age, education, marital status and employment), and the second one included the independent variables of our study (S-BIS-modified and Neurofibromas Question Ad Hoc).
The researchers include the variables following the adjusted R-squared statistic of the goodness of fit method [32]. The criteria fixed to exclude a variable from the model were set to p = > 0.05 [33]
Results
Description of the sample and S-BIS modified
The sample consisted of 205 patients with NF1 diagnoses, above 16 years old and with no missing data (Fig. 1). Presented 93 male patients and 112 female patients. The majority of the participants were young adults or adults (19–44), were single, had studied until high school, were employed and presented social support. Their family mostly gave this support. They did not receive psychological assistance, and their skin severity index was low. The average age was 33 years, with a good QoL (0.77/71.6) and low body image-related problems (5.13). A large part of the sample reported no problems at all with their tumors (Table 1).Table 1. Sample description—sociodemographic, dependent and independent variablesVariablesCategories/ RangesTotal (n = 205)Male (n = 93/ % = 45.37)Female (n = 112 / % = 54.63)W (p) / X^2^ (p)N (%)M (SD)N (%)M (SD)N (%)M (SD)Age16–74–33.67 (13.81)–31.47 (13.73)–35.5 (13.68)4371 (< 0.001)***Age groupsAdolescent (16–18)7 (3.41)–2 (2.15)–5 (4.46)–14.01 (0.007)**Young Adult (19–24)74 (36.10)–46 (49.46)–28 (25.00)–Adult (25–44)73 (35.61)–25 (26.88)–48 (42.86)–Middle aged (45–64)44 (21.46)–18 (19.35)–26 (23.21)–Aged (65–80)7 (3.41)–2 (2.15)–5 (4.46)–Marital statusMarried55 (26.83)–15 (16.13)–40 (35.71)–13.58 (0.003)**Single141 (68.78)–76 (81.72)–65 (58.04)–Divorced8 (3.90)–2 (2.15)–6 (5.36)–Widowed1 (0.49)–0 (0)–1 (0.89)–EducationNo-studies4 (1.95)–2 (2.15)–2 (1.79)–7.61 (0.107)Primary school27 (13.17)–15 (16.13)–12 (10.71)–Middle school38 (18.54)–21 (22.58)–17 (15.18)–High school78 (38.05)–37 (39.78)–41 (36.61)–University58 (28.29)–18 (19.35)–40 (35.71)–EmploymentEmployed107 (52.19)–48 (51.61)–59 (52.68)–0.341 (0.952)Unemployed83 (40.49)–39 (41.93)–44 (39.29)–Paid leave12 (5.85)–5 (5.38)–7 (6.25)–Retired3 (1.46)–1 (1.07)–2 (1.79)–Skin severity index^a^1–3–1.62 (0.77)–1.63 (0.75)–-1.61 (0.80)4371 (< 0.001)***Low severity115 (56.10)–49 (52.69)–66 (58.93)–2.57 (0.277)Medium severity53 (25.85)–29 (31.18)–24 (21.43)–High severity37 (18.05)–15 (16.13)–22 (19.64)–Psychological assistanceYes62 (30.24)–22 (23.65)–40 (35.71)–2.95 (0.086)No143 (69.76)–71 (76.34)–72 (64.29)–Social supportYes158 (77.07)–66 (74.19)–89 (79.46)–0.53 (0.467)No47 (22.93)–27 (25.81)–23 (20.54)–Sources of supportSocial networks3 (1.46)–2 (2.15)–1 (0.89)–0.03 (0.871)Institutions9 (4.39)–4 (4.30)–5 (4.46)– < 0.001 (1)Others9 (4.39)–4 (4.30)–5 (4.46)– < 0.001 (1)Family145 (70.73)–60 (64.52)–85 (75.89)–2.65 (0.103)Friends79 (30.24)–33 (35.48)–46 (41.07)–0.45 (0.500)Partner39 (19.02)–18 (46.15)–21 (53.85)– < 0.001 (1)EuroQoL (EQ-5D)0.00–1.00–0.77 (0.22)–0.82 (0.22)–0.73 (0.22)4278 (< 0.001)***EuroQol Visual Scale (EQ-VAS)0–100–71.6 (26.00)–76.57 (24.15)–67.48 (26.85)4005 (< 0.001)***S-BIS modified0–24–5.13 (6.25)–3.63 (6.25)–6.36 (6.67)1485 (< 0.001)Neurofibromas (Ad Hoc) ^b^0–3–0.95 (1.14)–0.75 (1.04)–1.11 (1.20)820 (< 0.001)Not at all103 (50.24)–53 (56.99)–50 (44.64)–5.03 (0.169)A little45 (21.95)–21 (22.58)–24 (21.43)–Quite a bit22 (10.73)–8 (8.60)–14 (12.50)–Very much35 (17.07)–11 (11.83)–24 (21.43)–Total data and segmentation by genderN, number of subjects; %, percentages; M, means; SD, standard deviations; W, Wilcoxon tests and X^2^, chi-squared test for non-parametric variables; p, Significance level: < 0.05 (), < 0.01 (), < 0.001 (). ^a^ Skin Severity was considered numerical and categorical. ^b^ Neurofibromas (Ad Hoc) was considered numerical and categorical
We tested the psychometric properties of the S-BIS modified and their relationships with the neurofibromatosis question Ad Hoc. The scale presented good validity and reliability requirements. The Cronbach’s alpha of the scale was 0.94 and presented a one-factor structure, similar to the original S-BIS version; the proportion of variance was 68%. The item total, inter item and item-rest correlations were above 0.4, which indicates that each item contributes to the internal consistency of the scale. The alpha if an item is dropped remains the same. Furthermore, it correlated with the EQ-5D and EQ-5D VAS scores (-0.52/-0.53). The neurofibromas assessed by the Ad Hoc test correlate with the modified S-BIS 0.83 and with EQ-5D and the EQ-VAS (-0.37/-0.41), respectively (Supplementary materials 2 and 3).
Body image, negative perception of the neurofibromas and skin severity index
The simple regression results show that a higher score on the neurofibromas question Ad Hoc increased the S-BIS score by 4.544 (< 0.001).
The S-BIS-modified and neurofibromas questions were positively correlated with gender and age. The skin severity index increased by 2.009 for the modified S-BIS, and individuals with a high severity score were 4.262 more likely to have higher scores than those with a low severity score, with both relationships being significant at < 0.001.
The findings from the regression analysis concerning the question about neurofibromas suggested that the skin severity index increased by 0.464. High-severity-rated individuals are more prone to neurofibroma appearance problems than low-severity-rated individuals are, with both relationships being significant at < 0.001 (Table 2).Table 2. Simple regressions with the independent variables and the sociodemographic dataVariables ^a^Categories^b^Total (n = 205)BβSE (B)t valuePr ( >|t|)95% CI (B)S-BIS modifiedGenderMale/ female2.7220.2170.8573.1750.0021.0324.413Age16–740.1000.2210.0313.2250.0010.0390.161Age GroupsAdolescent/ young adult − 2.263 − 0.1740.897 − 2.5240.012* − 4.031 − 0.495Adolescent/ middle aged3.2600.2151.0403.1330.0021.2085.311Skin Severity Index–2.0090.2460.5683.537 < 0.0010.9093.072Low severity/ high severity4.2620.2451.1673.651 < 0.0011.8006.147Neurofibromas (Ad Hoc)–4.5440.8280.21621.046 < 0.001 4.1184.969Neurofibromas (Ad Hoc)GenderMale/ female0.3540.1550.1582.2410.0260.0430.666Age16–740.0220.2670.0063.956 < 0.0010.0110.033Age GroupsAdolescent/ young adult − 0.550 − 0.2320.161 − 3.41 < 0.001 − 0.869-0.232Adolescent/middle aged0.7340.2650.1873.921 < 0.0010.3651.103EmploymentUnemployed/ paid leave0.8540.1760.3342.5540.0110.1951.513Skin severity index–0.4640.3160.0984.744 < 0.0010.2710.657Low severity/ high severity0.8570.2900.1984.321 < 0.0010.4661.248B, regression coefficient; β, standardized regression coefficient; SE, standard error of B; t value of B; Pr ( >|t|), Significance level: < 0.05 (*), < 0.01 (), < 0.001 (***); 95% CI, 95% confidence interval of B; ^a^ The variables selected correspond to those that significantly correlated with both variables; ^b^ We created dummy variables for those qualitative variables with more than two categories
Quality of life
The EQ-5D regressions include gender, age, marital status, education, employment and skin severity indices in the statistical model. Patients whose skin severity was moderate were 0.082 more likely to have higher scores on the EQ-5D than those whose skin severity was low, but there were no significant differences between patients with higher severity scores and those with higher severity scores on the EQ-5D. The modified S-BIS is included because it is significant (< 0.001). High scores on the modified S-BIS are related to a 0.21 decrease in the EQ-5D score. The neurofibromas question Ad Hoc was not significantly related to the EQ-5D score.
The EQ-VAS, includes gender, age and education in its statistical model. The S-BIS-modified scale is included because it is significant (< 0.001). High scores on the modified S-BIS (2.599) decrease scores on the EQ-VAS, with this finding being significant at < 0.001. The neurofibromas question Ad Hoc was not significantly related to the EQ-VAS score (Table 3).Table 3. Multiple regressions of the EQ-5D and EQ-VAS scores with the independent variables: adjusted for covariablesVariables^a^Categories^b^Total (n = 205)BβSE (B)t valuePr( >|t|)95% CI (B)EQ-5DCovariablesGenderMale/ female − 0.043 − 0.0960.062 − 1.5580.121 − 0.2170.025Age– − 0.003 − 0.2010.085 − 2.3710.019* − 0.367 − 0.035Marital StatusSingle/ married0.1140.2290.0822.7970.0060.0690.389Single/ divorced0.1730.1520.0652.3430.0200.0250.278EducationNo-studies/ middle school0.0420.0920.0601.5360.126 − 0.0250.210EmploymentUnemployed/ paid leave − 0.103 − 0.1100.061 − 1.8060.072 − 0.2290.009Skin Severity IndexLow severity/ medium severity0.0820.1630.0632.5800.0110.0390.286Low severity/ high severity0.0160.0280.0650.4300.667 − 0.0990.155Independent variablesS-BIS modified– − 0.021 − 0.6050.106 − 5.710 < 0.001* − 0.813 − 0.397Neurofibromas (Ad Hoc)–0.0330.1700.1081.5790.116-0.0410.382EQ-VASCovariablesGenderMale/ female − 3.230 − 0.0620.062 − 1.0070.315 − 0.1830.059Age GroupsAdolescent/ young adult6.1450.1140.0631.8140.071 − 0.0090.237Adolescent/ Aged − 10.825 − 0.0760.058 − 1.2970.196 − 0.1900.039EducationNo-studies/ primary school31.9520.4170.1492.7930.0060.1240.709No-studies/ middle school33.5500.5030.1683.0010.0030.1740.831No-studies/ high school42.2640.7910.2063.842 < 0.0010.3881.195No-studies/ University42.6610.7410.1923.861 < 0.0010.3651.117Independent variablesS-BIS modified– − 2.599 − 0.6240.104 − 6.023 < 0.001*** − 0.827 − 0.421Neurofibromas (Ad Hoc)–4.3700.1910.1041.8460.066-0.0120.394B, regression coefficient; β, standardized regression coefficient; SE, standard error of B; t value of B; Pr ( >|t|), Significance level: < 0.05 (), < 0.01 (), < 0.001 (); 95% CI, 95% confidence interval of B; ^a^ The table shows the variables selected following the Stepwise method; ^b^ We created dummy variables for those qualitative variables with more than two categories
QoL is associated with the S-BIS-modified questionnaire and the Neurofibromas ad. Hoc question. Simple regressions show that each subscale of the EQ-5D is related to the modified S-BIS, all of which have a significance < 0.05. Daily activities, pain and anxiety/depression were significant at < 0.001. The Neurofibromas Questionnaire (Ad Hoc) is related to daily activities, pain and anxiety/depression, with a significance < 0.001. Self-care and mobility were not significantly related to the question (Supplementary material 4).
Psychological assistance and social support
The correlations of psychological assistance show that it is directly associated with the skin severity index (0.159, < 0.05), especially for high-severity patients (0.188, < 0.01), and with social support (0.208, < 0.01), especially if support is given by family members (0.190, < 0.01), friends and others (< 0.05). Additionally, the modified S-BIS correlated directly with performing psychological assistance (0.218, < 0.01) but not with the neurofibromas question Ad Hoc. In contrast, the EQ-5D score is inversely associated with psychological assistance (− 0.238, < 0.01) (Table 4).Table 4. Correlations with Psychological AssistancePsychological AssistanceVariableCategoriesρPr( >|p|)GenderMale/ female0.1310.062Age– − 0.1120.111Age groupsAdolescent/ young adult0.1020.145Adolescent/ adult − 0.0020.980Adolescent/ middle Aged − 0.1110.112Adolescent/ aged − 0.0070.922Marital statusSingle/ married − 0.1830.009Single/ divorced0.0320.651Single/ Widowed − 0.0460.512EducationNo-studies/ primary school0.0260.709No-studies/ middle school − 0.0950.173No-studies/ hyigh school − 0.0570.420No-studies/ University0.1520.029EmploymentUnemployed/ employed − 0.1350.053Unemployed/ paid leave0.0170.811Unemployed/ retired − 0.0800.253Skin severity index–0.1590.023Low severity/ medium severity − 0.0250.722Low severity/ high severity0.1880.007Social supportNo/ yes0.2080.003Sources of supportNo / social networks0.0970.168No / institutions0.0660.345No / others0.1700.015*No / family0.1900.006No / friends0.1550.026No / partner − 0.0220.760EQ-5D– − 0.238 < 0.001EQ-VAS– − 0.1010.150S-BIS modified–0.2180.002Neurofibromas (Ad Hoc)–0.0770.270ρ, Spearman’s coefficient; Pr ( >|ρ|), Significance level: < 0.05 (), < 0.01 (), < 0.001 ()
The correlations with social support and sources of support show that social support is directly associated with psychological assistance and with family, friends and partner support (< 0.01). The EQ-5D score was negatively correlated with social support (− 0.210, < 0.01). Sources of support from others, from family and from friends correlated positively with psychological assistance (< 0.05). The EQ-5D score was inversely associated with family support (− 0.169, < 0.05). The medium severity of skin severity was negatively associated with social support and family and friends support (< 0.05). Social support and sources of support were not correlated with S-BIS-modified or Neurofibromas Question Ad Hoc scores (Table 5 and Supplementary material 5).Table 5. Correlations with social supportSocial supportVariableCategoriesρPr ( >|p|)GenderMale/fdemale0.0620.374Age–− 0.1790.010Age GroupsAdolescent/ young adult0.1440.039Adolescent/ adult− 0.0310.663Adolescent/ middle Aged− 0.1390.047Adolescent/ aged-0.0890.204Marital StatusSingle/ married− 0.1150.101Single/ divorced-0.0100.888Single/ widowed0.0380.587EducationNo-studies/ primary school0.0750.284No-studies/ middle school− 0.0680.330No-studies/ high school0.0210.764No-studies/ University0.0080.913EmploymentUnemployed/ employed− 0.1500.032Unemployed/ paid leave0.1360.052Unemployed/ retired− 0.1270.070Skin Severity Index-− 0.0940.180Low severity/ medium severity− 0.1550.026Low severity/ high severity0.0150.836Psychological AssistanceNo/ yes0.2080.003Sources of SupportNo / social Networks0.0660.344No / institutions0.1170.095No / others0.1170.095No / family0.848 < 0.001No / friends0.432 < 0.001No / partner0.264 < 0.001EQ-5D–− 0.2100.002EQ-VAS–− 0.0860.223S-BIS modified–0.1190.089Neurofibromas (Ad Hoc)–0.0040.953ρ, Spearman’s coefficient; Pr ( >|ρ|), Significance level: < 0.05 (*), < 0.01 (), < 0.001 (***)
Discussion
This research explored BI, the negative perception of the appearance of neurofibromas and clinical skin severity in NF1 patients; assessed its association with quality of life; and demonstrated the relevance of social support and psychological assistance among NF1 patients with BI concerns.
The vast majority of our NF1 cohort presented minor skin severity, only 18% of the individuals have high severity. Therefore, few of them reported negative perception of the appearance of neurofibromas, and they presented positive BI and QoL. For those who rated high skin severity, we noticed that they also had BI impairments and negative perception of the aspect of neurofibromas. When the skin is altered in NF1 patients, body image is disturbed [8]. Moreover, as we hypothesized, our results show that negative perception of the appearance of neurofibromas is an important factor in the increase in BI impairment in NF1 patients, especially considering that over 50% of our patients reported dissatisfaction with the appearance of their neurofibromas.
NF1 individuals from our CSUR had significantly lower QoL only if they had severe BI impairment, not if they reported negative perception of the appearance of neurofibromas. Previous studies have suggested that when cutaneous neurofibromas are numerous and extensively cover the body surface, individuals are more likely to experience a diminished QoL [13]. However, it is essential to note that the visibility of the disease itself does not reliably predict overall QoL [18]. We must consider the role of body image as a moderator in the relationship between disease visibility and QoL impairments [18].
Negative perception of the appearance of neurofibromas does not affect QoL in the same way as BI problems do. Accordingly, even though discontent with the appearance of neurofibromas plays an important role in BI, BI impairments do not merely derive from the negative perception the patient have about the appearance of their neurofibromas.
Therefore, instead of relying solely on the severity of skin manifestations to assess QoL, it is accurate to consider evaluating the overall concept of BI as a more meaningful indicator of overall QoL. Indeed, BI impairments affect each QoL domain evaluated by the EQ-5D and the EQ-VAS [19]. Modified S-BIS used in this study presented good validity and reliability requirements and correlated with the QoL test and the question referring to the neurofibromas appearance. Hence, it proves to be a reliable tool for assessing body image in NF1 patients.
Patients with NF1 and severe skin involvement, in our sample, correlated with increased body image concerns and negative perception of the appearance of neurofibromas. Various studies have reported that optimum psychological interventions could improve BI in these patients [12, 20, 21]. Consequently, it is reasonable that our patients reported having undergone or currently undergoing psychological assistance to address these issues.
Similarly, NF1 patients with poor QoL tend to report attending psychological assistance, and they also tend to inform that they have social support, especially from their family [11, 23]. The distinction between psychological assistance and social support becomes evident when considering that body image impairments do not seem to affect how NF1 patients perceive their social support. However, patients who report having received psychological assistance are more likely to report having social support networks, possibly because they learn coping strategies to acquire or maintain their social support. Therefore, psychological assistance appears to be an effective strategy for coping with body image impairments in NF1 patients.
Limitations of the study
A comprehensive understanding of the aspects involved in therapy, such as alliance, expectations, therapist effects, cultural adaptation of evidence-based treatments, treatment differences, accessibility and adherence and competence, is needed to better identify whether individuals who are receiving psychological assistance can address body image impairments and diminish their effects on NF1 patients’ QoL [34]. In this regard, it is crucial to implement longitudinal measurements that consider the progression of psychological assistance over time.
Additionally, the assessment of social support extends beyond the mere identification of sources of support. To enhance the understanding of its implications, measurements should also evaluate how patients derive tangible benefits from these supportive networks [11].
Conclusion
The findings of this study are particularly relevant to the minority population diagnosed with NF1, shedding light on the unique challenges they face and advancing research in the field of genetic disorders.
This study emphasizes the role of body image impairments as predictors of reduced quality of life (QoL) in NF1 patients. The Modified S-BIS questionnaire provides an effective tool to identify individuals at risk of QoL decline, enabling timely psychological intervention. Compared to skin severity, body image is a stronger indicator of QoL impairments. The Modified S-BIS directly measures body image issues without relying on clinical cut-off points, making it a valuable tool for ongoing patient monitoring. It also captures feelings of bodily insecurity—such as reduced attractiveness and self-confidence—which have been previously linked to negative body image in NF1 patients.
An increase in a patient’s body image impairment score over time could signal emerging QoL issues. Healthcare professionals should consider this metric in their clinical practice to shape effective interventions and improve the overall patient experience. Additionally, our findings support previous studies that highlight body image as a key factor in how NF1 patients perceive their bodies and how this perception influences their psychological well-being and QoL.
NF1 patients benefit from both positive social support and psychological assistance, particularly when facing QoL impairments. Notably, when patients seek psychological counseling, they often report having social support. However, a key difference arises when body image impairments increase. In these cases, patients may report receiving psychological support but not social support. Therefore, when healthcare professionals detect body image impairments in NF1 patients, it is crucial to guide them toward psychological therapies that also focus on enhancing social skills and providing psychoeducation for families and close social networks. This approach can help improve social support, ensuring that patients benefit from both professional and personal environments. Future research should explore the effects of psychological assistance and social support on NF1 patients with body image impairments.
Supplementary Information
Supplementary material 1: The modified S-BIS.Supplementary material 2: EFA analysis: S-BIS modified – Validity and Reliability Requirements; The Exploratory Factorial Analysis of the S-BIS modified scale.Supplementary material 3: Correlations between independent and dependent variables; Correlations between independent and dependent variablesSupplementary material 4: Simple regressions with the independent variables and the EQ-5D subscales.; Simple regressions performed with the EQ-5D subscalesSupplementary material 5: Correlations with Sources of Support; Correlations with the sources of support measures in the study
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hopwood P, Fletcher I, Lee A, Al Ghazal S. A body image scale for use with cancer patients. [cited 2023 Jan 12]. Available from: www.ejconline.com 10.1016/s 0959-8049(00)00353-111166145 · doi ↗ · pubmed ↗
- 2World health organization (WHO) [Internet]. 2023 [cited 2023 May 2]. Available from: https://www.who.int/