Reconstruction of a thumb metacarpophalangeal bone defect using the Masquelet technique: A case report
Gauthier Lagarde, Omar Alawadhi, Olivier Camuzard, Thierry Balaguer, Brieuc Monin, Elise Lupon

TL;DR
This case report shows how the Masquelet technique can successfully reconstruct severe thumb bone defects, avoiding amputation.
Contribution
The paper presents a novel application of the Masquelet technique in hand surgery for thumb reconstruction.
Findings
The Masquelet technique preserved thumb function in a severe osteoarticular injury.
Two-stage procedures may prevent amputation in post-infectious bone loss.
Conservative salvage is a viable alternative to amputation or toe transfer.
Abstract
Bone defects of the thumb secondary to trauma or infection pose a significant challenge for surgeons. The limited therapeutic options in such cases may, in the most severe scenarios, necessitate amputation, which has devastating functional consequences. The induced membrane technique, described by Masquelet, has proven effective in reconstructing bone loss in the lower limbs, particularly in septic contexts. However, its application in hand surgery remains underreported. In this case, we describe a bone and joint defect of the thumb's metacarpophalangeal joint, complicated by osteoarthritis following a dog bite injury. After failure of initial osteosynthesis, resulting in bone and joint destruction, we performed a two-stage metacarpophalangeal arthrodesis using an iliac bone graft and Masquelet's technique. The permanent use of a cement spacer is often employed in clinical practice,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
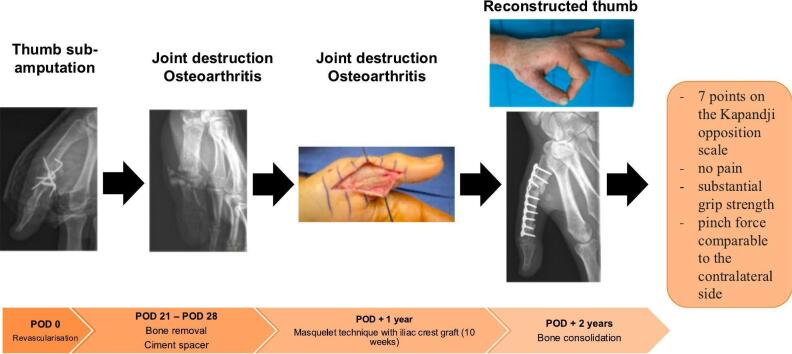 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Bone fractures and treatments · Reconstructive Surgery and Microvascular Techniques
Introduction
1
The thumb contributes to approximately 40 % of hand function through its roles in opposition and circumduction, requiring a balance of mobility and stability [1]. Because of its essential function, the thumb is often the primary focus of reconstructive procedures following trauma [2]. In France, among the 1.4 million hand injuries reported annually, the thumb is involved in more than 25 % of cases [3].
Animal bites are a common source of osteo-articular infections, which can lead to bone destruction. These infections require appropriate antibiotic treatment, skeletal stabilization, and bone tissue supplementation. The hand is the second most common site of osteoarticular infection after the knee [4]. The amputation rate secondary to osteomyelitis of the tubular bones approaches 39% [5]. In cases of composite digital trauma involving multitissue lesions, bone stabilization is the first stage of treatment, preceding vascular and nervous repair. Restoring skeletal length is a major challenge in the presence of a significant bone defect. Alternatives to amputation are limited and include bone distraction, structural allografts, arthrodesis, or vascularized bone grafts [6]. In manual laborers who require strong grip function, skeletal robustness becomes a critical factor and must be carefully considered when planning the reconstruction.
The induced membrane technique, described by Masquelet, enhances reconstruction of lower limb bone defects in septic conditions by restoring both bone integrity and strength. More recently, its application to the hand has attracted growing interest as a promising option for managing osteitis with a high risk of amputation [7]. This technique can effectively preserve segmental length while maintaining satisfactory function. The Masquelet-induced membrane technique is a two-stage procedure. The first stage consists of the surgical debridement of necrotic tissue and the implantation of a cement spacer matching the dimensions of the bone loss. The second stage involves autologous bone grafting after the removal of the cement while preserving the induced membrane [8]. The pseudosynovial membrane secretes osteomodulating and angiogenic growth factors, such as VEGF, TGF-β, and BMP2, as studied by Pelissier et al [9]
In this report, we describe a case of metacarpophalangeal bone and joint loss of the thumb, complicated by osteomyelitis following a dog bite injury in a manual laborer. The condition was managed using an iliac crest autograft and a two-stage metacarpophalangeal arthrodesis based on the Masquelet induced membrane technique.
Case report
2
A 31-year-old right-hand dominant man, working as a dog handler, with no significant medical history but an active smoking habit, presented to the emergency department with a dog bite injury to the left thumb. On initial examination, a major wound was observed in the palmar T2 zone, with dorsal attachment and signs of devascularization (sub-amputation). Radiographs revealed substantial bone and joint severe injury at the first phalanx, first metacarpal, and metacarpophalangeal (MCP) joint. The initial sensory examination showed normal sensation on the dorsal aspect of the thumb but no sensation on the volar aspect. The patient underwent urgent revascularization, debridement, open reduction, and temporary MCP arthrodesis using five small Kirschner wires. The arteries and nerves were anastomosed using non-absorbable 9.0 sutures, and intraoperative assessment confirmed patency of the anastomosis (Fig. 1). Immediately postoperatively, the finger showed signs of revascularization, and the initial postoperative course was satisfactory. Management included single-agent antiplatelet therapy for 45 days and a 10-day course of antibiotics. The patient was discharged after five days of inpatient monitoring and was followed up weekly.Fig. 1. Lateral radiograph at the first operative stage during replantation.Fig. 1
At three weeks postoperatively, the patient presented with purulent wound discharge and radiographic signs of osteitis, although the thumb remained viable. At four weeks, despite the absence of bone consolidation, the decision was made to remove the devitalized bone and fixation material and to place a 3-centimeter antibiotic-impregnated polymethylmethacrylate (PMMA) spacer spanning the first phalanx. The patient was subsequently lost to follow-up.
One year later, he returned with a palmar draining fistula with purulent discharge and exposed cement. He reported significant pain and total functional impairment. Radiographs confirmed complete joint destruction with chronic osteoarthritis (Fig. 2). A two-stage surgical treatment was planned using the Masquelet technique with antibiotic coverage. The first stage, performed one year after the initial trauma, involved bone resection with fistulectomy and placement of an antibiotic-loaded PMMA spacer for ten weeks. No osteosynthesis hardware was used to secure the spacer between surgical stages; immobilization was maintained with an orthosis. The fixation strength of the PMMA spacer was deemed sufficient to allow stabilization with orthotic support alone. Dual antibiotic therapy, including rifampicin and fluoroquinolone, was administered for ten weeks based on microbiological findings.Fig. 2. Frontal radiograph at 3 weeks showing osteoarthritis, necessitating the removal of the osteosynthesis material.Fig. 2
During the second surgical stage, the antibiotic spacer was carefully removed while preserving the induced membrane, which was approximately 2 mm thick and continuous (Fig. 3). A tricortical iliac crest autograft was harvested and designed to fill the defect, supplemented with allograft composite bone within the membrane. A long locking plate (2 mm) contoured to 15° of flexion was fixed with screws to achieve the definitive arthrodesis position. The induced membrane was sutured around the graft to optimize its integration.Fig. 3. Photograph of the thumb showing the lateral opening of the Masquelet-induced membrane at one month, allowing for the replacement of the cement with iliac crest bone.Fig. 3
Following surgery, the thumb remained viable, and intraoperative radiographs confirmed stable fixation. The patient was immobilized with a gauntlet splint for three months postoperatively, both due to non-compliance with postoperative recommendations (continued tobacco use, failure to maintain strict immobilization) and to maximize the chances of success in the context of multiple surgical revisions.
The patient underwent monthly radiographic follow-ups. At the first postoperative visit, ten days after surgery, radiographs showed stable fixation with no displacement, and the surgical wound was well-healed. Passive physiotherapy was initiated immediately after surgery, followed by active physiotherapy at three weeks. Weight-bearing activities were permitted at three months.
At one year postoperatively, radiographs confirmed bone consolidation (Fig. 4). The thumb demonstrated good mobility, with a Kapandji opposition score of 7 (Fig. 5). Other thumb joints preserved normal range of motion, as mobility was maintained through the trapeziometacarpal and interphalangeal joints. Functionally, the patient reported no pain, with grip and pinch strength comparable to the contralateral side and to his pre-injury status. He returned to manual work and expressed full satisfaction with the functional outcome of the thumb. The scars were considered fully acceptable by the patient. Given the absence of complaints, it was decided not to remove the osteosynthesis hardware.Fig. 4. Frontal radiograph at 12 months postoperatively, demonstrating bone consolidation with ossification.Fig. 4. Fig. 5Kapandji opposition scale.a. Kapandji score for assessing the opposition of the thumb.b. Photograph of the patient thumb at 12 months postoperatively, demonstrating good mobility, achieving a score of 7 points on the Kapandji opposition scale.Fig. 5
Discussion
3
The management of hand trauma—particularly thumb injuries complicated by chronic osteoarticular infection—remains a significant surgical challenge, often associated with a high risk of amputation. While permanent cement spacers are commonly used in clinical practice, their use is frequently associated with complications such as spacer fracture, pain, and dislocation. This report presents a non-compliant patient, which justified the use of a simple and efficient surgical approach—avoiding microsurgery, prolonged hospitalization, and allowing for straightforward physiotherapy. Report presents an original application of a well-established and reliable technique that facilitated the preservation and functional recovery of the patient's thumb.
In cases of post-traumatic or septic bone loss, the induced membrane technique offers a superior conservative approach [10,11]. This method is simple, reproducible, and applicable in both emergency and elective settings. It enables effective control of chronic infection through thorough debridement while initiating reconstruction and preserving skeletal length. Several studies, including those by Lum et al., support a conservative approach prior to considering amputation or more complex reconstructions such as toe-to-thumb transfers [12]. There is limited literature regarding the application of this technique to the hand and even fewer reports specific to the thumb [[12], [13], [14], [15]]. Our review of the literature on metacarpophalangeal trauma with bone defects treated using the Masquelet technique highlights a consensus among authors regarding the importance of prioritizing conservative management at the thumb level. A detailed summary of relevant studies is presented in Table 1. Most involve post-traumatic or infectious etiologies, with an interval between the two surgical stages ranging from 17 days to 7 months [[13], [14], [15]]. The need for additional procedures, such as skin flaps, remains rare and typically arises when soft tissue loss is present [14]. Reported bone consolidation was achieved in all cases, generally within 2 to 12 months [[12], [13], [14]]. These results, although based on small series or case reports, suggest that the Masquelet technique may be a reliable option for managing bone defects in the hand, even in complex scenarios. Although current outcomes are promising, further case series are required to validate these results and establish stronger evidence.Table 1. Table summarizing the literature on metacarpophalangeal trauma with bone defects treated using the Masquelet technique.Table 1. ReferenceNumber of patientsEtiology of bone defectAssociated lesionsDelay between T1-T2 Masquelet's procedureAdditional surgeryTime to consolidationFollow- upFlammans [13]113 sepsis, 8 traumaNo17 days- 7 monthsNo1,5–12 months5 yearsLum [12]1TraumaNo4 weeksNo2 months2 yearsLim [15]1TumorNo3 weeksNo_9 monthsLuttenberger [14]1TraumaSkin defect6 weeksSkin flap8 weeks8 months
In our case, the Masquelet technique successfully preserved thumb-to-finger function, offering a more functional and aesthetically acceptable result than amputation. Amputation at the thumb level is associated with significant disability and poor functional prognosis [16]. When a vascularized thumb with extensive bone loss is salvageable, it should be prioritized as the first-line treatment. Alternative reconstructive procedures—such as index finger pollicization or toe-to-hand transfer—may compensate for post-amputation deficits but should be reserved as last-resort options. The sacrifice of a potentially functional structure is only justified when all conservative options have been exhausted or deemed unfeasible. While toe transfers can restore function, patient acceptance is often limited due to the heterotopic appearance of the reconstruction and the morbidity associated with the donor site [17].
Several limitations should be acknowledged in this case. This report, following the SCARE guidelines [18], describes a single case of thumb reconstruction using this technique by a trained hand surgeon, and further case series are necessary to draw broader conclusions. Additionally, the postoperative follow-up period remains relatively short, highlighting the need for longer-term evaluation to confirm these promising preliminary results. A systematic assessment of the technique's indications, associated risks, and long-term outcomes is essential to better define its role in complex reconstructive procedures.
Conclusion
4
The application of the Masquelet technique to the hand represents a promising option for managing large bone defects in osteitis cases with a high risk of amputation. This technique allowed for the preservation of sufficient bone length to maintain pollici-digital function, enabling satisfactory gripping. Further studies are required to validate these initial findings over the long term.
SCARE guideline
The work has been reported in line with the SCARE criteria 2023.
Author contribution
GL: Gauthier Lagarde.
BM: Brieuc Monin.
O.M: Omar Alawadi.
T.B: Thierry Balaguer.
O·C: Olivier Camuzard.
E.L: Elise Lupon.
G.L: conceptualization, investigation, project administration, writing – original draft. B.M: conceptualization, investigation, methodology, writing – original draft. O.M: investigation, software, writing – original draft**. T.B and O·C**: supervision, writing – review and editing. E.L: project administration, supervision, writing – review and editing.
Declaration of patient consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. This study was approved by our institution's Research Ethics Committee.
Guarantor
All authors in the article accept full responsibility for the work, have access to the patient's information, and decide to publish.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Declaration of competing interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Emerson E.T.Krizek T.J.Greenwald D.P.Anatomy, physiology, and functional restoration of the thumb Ann. Plast. Surg.3621996 Feb 180191891938410.1097/00000637-199602000-00014 · doi ↗ · pubmed ↗
- 2Muzaffar A.R.Chao J.J.Friedrich J.B.Posttraumatic thumb reconstruction Plast. Reconstr. Surg.11652005 Oct 103e–22e 10.1097/01.prs.0000182650.17230.2a 16217456 · doi ↗ · pubmed ↗
- 3Mouton J.Houdre H.Beccari R.Tarissi N.Autran M.Auquit-Auckbur I.Plaies de main aux urgences : étude préliminaire de 80 dossiers d’un assureur des établissements de santéRevue de Chirurgie Orthopédique et Traumatologique.10282016 Dec 1723726
- 4Lipatov K.V.Asatryan A.Melkonyan G.Kazantcev A.D.Solov’eva E.I.Cherkasov U.E.Septic arthritis of the hand: current issues of etiology, pathogenesis, diagnosis, treatment World J. Orthop.1372022 Jul 186226303605137510.5312/wjo.v 13.i 7.622PMC 9302027 · doi ↗ · pubmed ↗
- 5Reilly K.E.Linz J.C.Stern P.J.Giza E.Wyrick J.D.Osteomyelitis of the tubular bones of the hand J. Hand. Surg. [Am.]2241997 Jul 64464910.1016/S 0363-5023(97)80122-09260620 · doi ↗ · pubmed ↗
- 6Gan A.W.T.Puhaindran M.E.Pho R.W.H.The reconstruction of large bone defects in the upper limb Injury 4432013 Mar 3133172334023710.1016/j.injury.2013.01.014 · doi ↗ · pubmed ↗
- 7Ono R.Komura S.Hirakawa A.Hirose H.Tsugita M.Masuda T.Staged arthrodesis using the Masquelet technique for osteomyelitis of the finger with articular destruction: a report of two cases Arch. Orthop. Trauma Surg.13972019 Jul 1102510313109375410.1007/s 00402-019-03197-5 · doi ↗ · pubmed ↗
- 8Masquelet A.C.Fitoussi F.Begue T.Muller G.P.Reconstruction of the long bones by the induced membrane and spongy autograft Ann. Chir. Plast. Esthet.4532000 Jun 34635310929461 · pubmed ↗