Beyond Spasticity: The Dual Impact of Selective Dorsal Rhizotomy in Spastic Quadriplegic Patients With Generalized Dystonia and the Need for Intrathecal Baclofen
Sevgi Sarikaya-Seiwert, Ralf Clauberg, Ina Hainmann, Hartmut Vatter, Hannes Haberl, Ehab Shabo

TL;DR
This study explores how combining selective dorsal rhizotomy with retained intrathecal baclofen therapy can help manage spasticity and dystonia in cerebral palsy patients.
Contribution
A novel surgical strategy is introduced for managing mixed movement disorders in CP patients by retaining the ITB system during SDR.
Findings
SDR reduced spasticity but worsened dystonia in most patients.
Reintroducing ITB after SDR significantly improved dystonia and motor function.
ITB dosage requirements decreased after SDR.
Abstract
Background Selective dorsal rhizotomy (SDR) is primarily indicated for spastic diplegia, effectively reducing lower limb spasticity. However, its role in generalized dystonia remains controversial, as some reports suggest potential symptom exacerbation. In such cases, intrathecal baclofen (ITB) represents the preferred approach. This study evaluates the effects of SDR as a secondary intervention following insufficient ITB therapy on motor function in patients with spastic quadriplegic cerebral palsy (CP) and generalized dystonia while also introducing a novel surgical strategy to approach mixed movement disorders. Material and methods This retrospective study included patients with spastic quadriplegic cerebral palsy and generalized dystonia treated at our institution between 2018 and 2023. All patients (n = 16) initially received intrathecal baclofen (ITB) therapy. In three…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
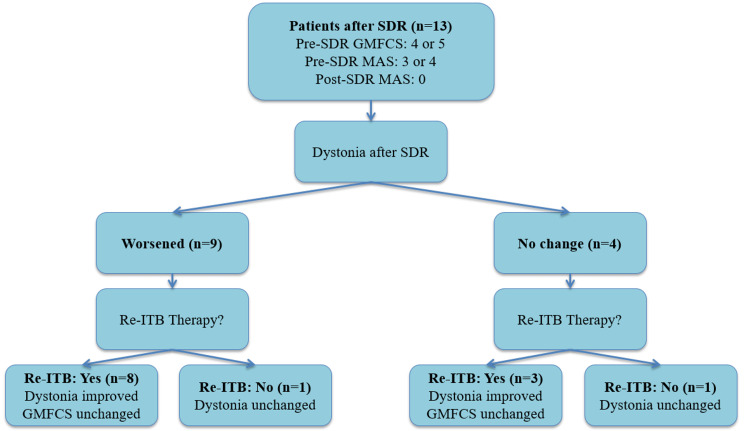 Figure 1
Figure 1| No. of Patients | 13 | |
| Age at Diagnosis (months) | 20.2 (range: 12-31) | |
| Male/Female | 9/4 | |
| GMFCS | Level IV | 1 |
| Level V | 12 | |
| MAS score | 3 | 2 |
| 4 | 11 | |
| Time of ITB (years) | 4.8 years (range: 3-8 years) | |
| Age at SDR | 12.3 years (range: 9-16 years) | |
| Follow-up time after SDR | 11.2 months (range: 6-16 months) | |
| SDR alone | ITB after SDR | p-values | ||
| Patients No. (%) | 13 | 11 | ||
| Spasticity | improved | 13 (100%) | remained improved after SDR | p = 1.0 |
| no change | 0 | |||
| worsened | 0 | |||
| Dystonia | improved | 0 | 11 (100%) | p < 0.001 |
| no change | 4 (30.8%) | 0 | ||
| worsened | 9 (69.2%) | 0 | ||
| Standing | improved | 5 (38.5%) | 11 (100%) | p < 0.001 |
| no change | 8 (61.5%) | 0 | ||
| worsened | 0 | 0 | ||
| Sitting | improved | 0 | 11 (100%) | p < 0.001 |
| no change | 4 (30.8%) | 0 | ||
| worsened | 9 (69.2%) | 0 | ||
| Transition movements | improved | 0 | 11 (100%) | p < 0.001 |
| no change | 13 (100%) | 0 | ||
| worsened | 0 | 0 | ||
| Required dosage of intrathecal Baclofen (Median ± SD) in µg/d | 485±61.5 | 175±27.4 | p < 0.001 | |
| Patient Number | Age at Diagnosis (months) | Years with ITB | ITB Dosage pre-SDR (µg/d) | Age at SDR (years) | ITB Removal | Follow-up (months) | Pre-SDR GMFCS | Post-SDR GMFCS | Pre-SDR MAS | Post-SDR MAS | Dystonia after SDR | Post-SDR Standing | Post-SDR Sitting | Post-SDR Transition Movement | Re-ITB Therapy | Dystonia (SDR+ITB) | Standing (SDR + ITB) | Sitting (SDR + ITB) | Transition Movement (SDR + ITB) | ITB Dosage post-SDR (µg/d) |
| 1 | 18 | 4 | 535 | 9 | Yes | 16 | 5 | 5 | 4 | 0 | worsened | no change | worsened | no change | yes | improved | improved | improved | improved | 170 |
| 2 | 15 | 6 | 512 | 12 | No | 14 | 5 | 5 | 4 | 0 | worsened | no change | worsened | no change | yes | improved | improved | improved | improved | 175 |
| 3 | 20 | 4 | 487 | 13 | No | 14 | 5 | 5 | 4 | 0 | worsened | no change | worsened | no change | yes | improved | improved | improved | improved | 235 |
| 4 | 24 | 3 | 420 | 14 | No | 13 | 5 | 5 | 3 | 0 | no change | improved | no change | no change | yes | improved | improved | improved | improved | 205 |
| 5 | 17 | 5 | 387 | 14 | No | 11 | 4 | 5 | 3 | 0 | no change | improved | no change | no change | yes | improved | improved | improved | improved | 175 |
| 6 | 12 | 4 | 400 | 13 | No | 11 | 5 | 5 | 4 | 0 | worsened | no change | worsened | no change | yes | improved | improved | improved | improved | 150 |
| 7 | 25 | 5 | 575 | 15 | Yes | 10 | 5 | 5 | 4 | 0 | no change | no change | no change | no change | no | n. d. | n. d. | n. d. | n. d. | 0 |
| 8 | 30 | 7 | 455 | 15 | No | 10 | 5 | 5 | 4 | 0 | worsened | improved | worsened | no change | yes | improved | improved | improved | improved | 210 |
| 9 | 27 | 8 | 415 | 16 | No | 8 | 5 | 5 | 4 | 0 | worsened | no change | worsened | no change | yes | improved | improved | improved | improved | 150 |
| 10 | 31 | 4 | 485 | 12 | No | 8 | 5 | 5 | 4 | 0 | worsened | improved | no change | no change | yes | improved | improved | improved | improved | 155 |
| 11 | 22 | 4 | 550 | 11 | Yes | 7 | 5 | 5 | 4 | 0 | worsened | improved | worsened | no change | no | n. d. | n. d. | n. d. | n. d. | 0 |
| 12 | 19 | 3 | 420 | 11 | No | 6 | 5 | 5 | 4 | 0 | no change | no change | worsened | no change | yes | improved | improved | improved | improved | 175 |
| 13 | 18 | 4 | 510 | 10 | No | 6 | 5 | 5 | 4 | 0 | worsened | no change | worsened | no change | yes | improved | improved | improved | improved | 200 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebral Palsy and Movement Disorders · Botulinum Toxin and Related Neurological Disorders · Neurogenetic and Muscular Disorders Research
Introduction
Cerebral palsy (CP) is a group of permanent movement disorders that emerge in early childhood, primarily affecting movement and posture. CP is classified into four major motor types: spastic, dyskinetic, ataxic, and mixed [1,2], with spastic CP being the most prevalent, affecting approximately 80%-95% of diagnosed individuals [1,3].
Spasticity, characterized by increased muscle tone leading to stiffness and restricted movement, significantly impacts mobility, daily activities, and overall quality of life [1-3]. Many patients diagnosed with spastic CP also exhibit various degrees of dystonia, a movement disorder marked by involuntary muscle contractions that cause repetitive movements or abnormal postures [1,2].
Given the complexity of these motor impairments, accurate assessment tools, such as the modified Ashworth scale (MAS) for muscle tone evaluation and the Gross Motor Function Classification System (GMFCS) for functional classification, are crucial in clinical decision-making [4,5].
Among non-ambulatory children with severe spasticity or mixed CP, surgical interventions such as selective dorsal rhizotomy (SDR) and intrathecal baclofen (ITB) therapy are commonly utilized to manage symptoms [6-9].
ITB is typically preferred for patients with generalized spasticity or mixed movement disorders, as it effectively reduces spasticity in both the upper and lower extremities while also alleviating dystonia-related pain [2,6,7,10-12]. SDR, on the other hand, is primarily indicated for ambulatory children with spastic diplegia, where the goal is to improve gait and overall mobility [2,11,13-15].
Numerous studies have demonstrated SDR’s efficacy in reducing lower limb spasticity [3,16,17]. Its role in managing accompanied generalized dystonia remains controversial. Some reports suggest that SDR may exacerbate dystonic symptoms in certain patients, highlighting the importance of careful patient selection and individualized treatment planning [18].
Despite extensive research on ITB and SDR separately, there is a notable lack of studies analyzing functional neurological outcomes in complex cases involving both spasticity and generalized dystonia. Moreover, there is limited guidance on optimal surgical strategies when ITB therapy fails. In such cases, one potential approach involves the removal of the ITB pump system followed by SDR [2,19,20].
This study aims to evaluate the efficacy of SDR as a secondary intervention in conjunction with the reinitiation of ITB therapy in patients with complex movement disorders, specifically those diagnosed with spastic quadriplegic CP and concurrent generalized dystonia. Additionally, we propose a novel surgical strategy for managing patients exhibiting mixed movement disorders characterized by the coexistence of spasticity and generalized dystonia. This strategy seeks to optimize functional outcomes, minimize potential surgical complications, and enhance overall quality of life.
Materials and methods
Patients’ selection and inclusion criteria
Between 2018 and 2023, all patients (n = 16) with spastic quadriplegic cerebral palsy and generalized dystonia initially received intrathecal baclofen (ITB) therapy at our institution. ITB monotherapy was effective in only three patients; in the remaining 13, spasticity control was insufficient, necessitating subsequent selective dorsal rhizotomy (SDR) without removal of the existing ITB system. Accordingly, this retrospective study includes all patients (n = 13) who underwent SDR following inadequate response to ITB monotherapy.
Surgical approach
Initially, all patients underwent intrathecal baclofen (ITB) therapy due to concurrent generalized dystonia. However, over time, these patients exhibited suboptimal spasticity control with ITB monotherapy. As a result, selective dorsal rhizotomy (SDR) was conducted.
Once the patients were approved for SDR, ITB therapy was gradually weaned in preparation for the procedure. They did not receive intrathecal baclofen for at least one month before SDR to prevent baclofen withdrawal symptoms such as increased spasticity (rebound effect), agitation, hallucinations, seizures, and, in severe cases, delirium or multi-organ failure.
SDR is performed under general anesthesia with the patient in the prone position, using standard microsurgical techniques. The procedure involves a single-level laminotomy, most commonly at the L1-L2 level, as determined preoperatively by spinal MRI to accurately localize the conus medullaris. Intraoperative electrophysiological stimulation is then employed to identify hyperactive dorsal (sensory) rootlets, which are selectively sectioned. Based on stimulation response, approximately 60-80% of the abnormal rootlets are bilaterally divided to achieve optimal spasticity reduction while preserving motor function.
Given the challenges associated with the prone positioning required for SDR and the additional risks of prolonged operative time and complications related to intraoperative repositioning to side position for explantation of the ITB system, the ITB system was not explanted after completing SDR.
Multidimensional assessment of movement disorders was conducted before and after the SDR procedure using the following scales: Gross Motor Function Classification System (GMFCS), a widely used, standardized, and five-level classification system that classifies motor function in children with cerebral palsy based on self-initiated movement, with level I indicating minimal motor function impairment, whereas level V represents severe limitations in voluntary movement, requiring extensive use of assistive technology [5]. For spasticity, we used the Modified Ashworth Scale (MAS), a clinical tool that assesses the resistance during passive muscle stretching and ranges from 0 (no increase in muscle tone) to 4 (affected part(s) rigid in flexion or extension), providing a semi-quantitative measure of hypertonia [21]. Dystonia was assessed mainly based on clinical observation of involuntary muscle contractions that result in repetitive movements and abnormal postures; however, the Fahn-Marsden Dystonia Rating Scale (FMDRS) [22], composed of two clinician-rated subscales (a movement subscale ranging from 0 to 120 points, based on patient examination, and a disability subscale ranging from 0 to 30 points, based on the patient’s report of disability in activities of daily living), was used as a supportive tool and not as a primary tool due to its limitations, such as the absence of detailed assessment of individual body areas, such as separate ratings for proximal and distal limbs [22].
Specific functional abilities were evaluated using a two-step approach. First, a visual gait assessment scale was applied [23], followed by a clinical evaluation of three key motor function skills: standing, sitting, and transition movements. Functional outcomes were categorized as “improved,” “unchanged,” or “worsened” based this dual approach.
If the dystonia and the motor functions (standing, sitting and transition movement) did not improve after SDR during the initial postoperative evaluation within four weeks, reinitiation of ITB therapy was indicated. Due to the remaining ITB system, no further surgery was needed to reinitiate ITB therapy.
Following the combined approach (SDR and ITB) as well as during follow-ups, dystonia and motor functions (standing, sitting and transition movement) were thoroughly assessed using the same standardized approach of presurgical evaluation using GMFCS, AMS and visual gait assessment scale.
The clinical evaluation of movement disorders in all patients was conducted, at the time of first diagnosis as well as during follow-ups, in an interdisciplinary setting involving neurosurgeons, orthopedic surgeons, neuro-pediatricians, and physiotherapists.
The required dosage of intrathecal baclofen to effectively reduce the dystonia without causing any side effects before and after SDR in µg/day was also analyzed.
Statistical analysis
All data analysis was performed using IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp. In the case of categorical variables, data are given as numbers and percentages. After normality testing via the Shapiro-Wilk test, continuous normally distributed data were compared using t-tests, while the Mann-Whitney U test was used for non-parametric data. Nominal data were tested between groups using Fisher’s exact test and in the case of multinomial data with a chi-squared test.
A p-value of <0.05 was considered statistically significant.
Results
Patient cohort and general characteristics
A total of 13 patients (nine males, four females) with generalized dystonia and severe spastic quadriplegic cerebral palsy (CP) were included in this study. The average age at CP diagnosis was 20.2 months (range: 12-31 months).
Due to the absence of improvement in spasticity and motor impairments, all patients underwent a secondary SDR. Patients had an average of 4.8 years (range: 3-8 years) of intrathecal ITB therapy before undergoing SDR. The average age at SDR was 12.3 years (range: 9-16 years). The mean follow-up time after SDR was 11.2 months (range: 6-16 months). Patients’ characteristics are summarized in Table 1.
Development of spasticity, motor function, and dystonia after SDR
GMFCS level, MAS score, and specific functional abilities developed after SDR as follows:
GMFCS level: Before and after SDR, all patients remained at the highest level of impairment (GMFCS level V) with one patient even worsening from GMFCS level IV pre-SDR to GMFCS level V post-SDR. This indicates that SDR did not significantly improve overall mobility.
MAS scores: Before SDR, 11 had a MAS score of 4 and two patients had an MAS score of 3. After SDR, this score dropped to 0 in all patients, indicating a successful reduction of spasticity.
Standing: Eight patients (61.5%) showed no change, while five patients (38.5%) improved.
Sitting: Four patients (30.8%) showed no change, while nine patients (69.2%) worsened.
Transition movements: All patients (100%) exhibited no changes in transition movements.
Dystonia: 9 out of 13 patients (69.2%) experienced worsening of dystonia after SDR. The rest four patients (30.8%) had stable dystonia.
Development of motor function and dystonia after ITB reinitiation
Since most of the patients experienced worsening dystonia and none of the patients had an improvement of overall motor function after the SDR surgery, oral baclofen therapy was started in patient number 1 three weeks after SDR. The symptoms got slightly better with a baclofen dose of 30 mg/day. Due to this notable improvement, intrathecal ITB therapy was reintroduced to control dystonia in all patients. Two families (patients 7 and 11) opted against renewed ITB therapy. In one case (patient 1), a new central ITB catheter was implanted due to a previously removed central catheter during the SDR surgery.
Overall, 11 of 13 patients (84.6%) underwent a reinitiation of ITB therapy. Remarkably, all 11 patients (100%) who underwent reinitiation of ITB therapy exhibited a significant improvement in dystonia and all functional abilities (standing, sitting, and transition movements) with a p-value of <0.001.
Furthermore, the required dosage of intrathecal baclofen to control dystonia after SDR (175±27.4µg/d) was significantly lower than the required dosage before SDR (485±61.5µg/d) with a p-value of <0.001 in both t-test and Mann-Whitney U test.
A detailed comparison of motor function and dystonia progression following SDR alone and after the combined approach (SDR and ITB) as well as the required ITB dosage is presented in Table 2.
Details about patients’ characteristics and motor function development are presented in Table 3.
To facilitate better comprehension of the detailed tables presented above, the results are summarized in an easily interpretable visual format in Figure 1.
Illustrates motor function outcomes (GMFCS level, MAS score and dystonia status) following the reinitiation of intrathecal baclofen (ITB) therapy after selective dorsal rhizotomy (SDR).
Discussion
Selective dorsal rhizotomy (SDR) is well-established for managing spasticity, but its effectiveness in cases with concurrent generalized dystonia remains uncertain, with some studies suggesting it may worsen dystonic symptoms [18]. This underscores the importance of careful patient selection, with ITB therapy typically being the preferred approach for generalized dystonia. However, there is a lack of research on the functional outcomes of treating complex and mixed cases with both spasticity and generalized dystonia and no reports on the combined or simultaneous use of the two approaches (SDR and traumatic brain injury [TBI]) [24].
Our retrospective study examines the impact of SDR as a secondary intervention following insufficient initial ITB therapy, then combined with ITB reinitiation in patients with spastic quadriplegic CP and coexisting generalized dystonia, proposing a novel surgical approach for these mixed movement disorders.
Limited studies in the literature have investigated the effectiveness of secondary SDR following unsuccessful ITB therapy for spasticity management [2,19,20]. These studies describe a procedure in which, after completing SDR, patients are repositioned for baclofen system removal with separate incisions made on the back and abdomen to extract the baclofen pump and catheters [2,20,24].
This additional surgical step logically and inevitably extends the overall operative duration, potentially increasing the risk of surgical complications. However, information about extended surgery duration and postoperative complications was not reported in the existing literature. In our institute, we followed this in our first case routine by removing the intrathecal part of the catheter of the baclofen pump. We disconnected the system from the connection of the intrathecal catheter with the pump. To avoid potential risks associated with intraoperative repositioning of the patient and prolonged surgery, we decided, to retain the baclofen pump after completing the SDR. The surgery for removal of the pump was scheduled three months after the SDR surgery.
Consistent with previous findings in the literature, we observed that SDR effectively reduced spasticity, as demonstrated by a decrease in MAS scores from 4 to 0 in all patients. However, it did not lead to improvements in gross motor function, with GMFCS levels remaining at level V. Moreover, SDR alone was insufficient in managing dystonia, as 69.2% of cases experienced a worsening of symptoms, requiring the reintroduction of ITB therapy. Notably, patients who received ITB reinitiation following SDR showed functional improvements in 100% of cases, including enhanced abilities to sit, stand, and perform transition movements. These results suggest that the reintroduction of ITB therapy after SDR significantly improves functional outcomes in patients with mixed severe quadriplegic spastic CP and generalized dystonia.
These findings underscore the limitations of SDR in cases where dystonia coexists with spasticity. While SDR effectively reduces spasticity, its potential to exacerbate dystonic symptoms highlights the need for individualized treatment strategies.
The success of ITB reinitiation after SDR suggests that a combined approach may be beneficial for selected patients, reinforcing the importance of thorough preoperative assessment and personalized treatment planning.
Furthermore, our study suggests that in patients with mixed motor function impairments who have experienced an inadequate response to ITB therapy, performing SDR without explanting the existing ITB system during the SDR procedure may represent a safe and effective management strategy.
This strategy could minimize potential surgical complications as previously mentioned as well as eliminate the need for an additional surgical procedure in case ITB therapy should be reinstated, thereby reducing surgical burden and associated risks for the patient.
Overall, this study represents the first report in the literature addressing this highly complex subgroup of CP patients, characterized by quadriplegic involvement and generalized dystonia. Additionally, it introduces a novel surgical approach that has not been previously described. This technique is designed to minimize potential surgical complications by reducing operative time while also improving the clinical outcomes of these patients.
The present study is, however, limited by its retrospective design, small patient cohort, and single-center setting, which may restrict the statistical power and affect the external validity and generalizability of the results.
Larger, multicenter prospective studies are needed to validate the findings of this study and, if proven beneficial, standardize the dual surgical approach in highly complex CP cases.
Conclusions
Selective dorsal rhizotomy remains a valuable surgical option for reducing spasticity but does not enhance motor function in quadriplegic patients with concurrent generalized dystonia. Moreover, it may contribute to worsening dystonia in the majority of cases, underscoring the need for ITB reinitiation after SDR. These findings highlight the importance of a carefully tailored, multimodal approach to complex and mixed cerebral palsy cases with spasticity and dystonia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Identification and measurement of dystonia in cerebral palsy Dev Med Child Neurol Rice J Skuza P Baker F 124912555920172878647610.1111/dmcn.13502 · doi ↗ · pubmed ↗
- 2Comparison of intrathecal baclofen pump insertion and selective dorsal rhizotomy for nonambulatory children with predominantly spastic cerebral palsy J Neurosurg Pediatr Mansur A Morgan B Lavigne A 2172233020223590177210.3171/2022.4.PEDS 21576 · doi ↗ · pubmed ↗
- 3Surgical techniques of selective dorsal rhizotomy for spastic cerebral palsy. Technical note Neurosurg Focus Park TS Johnston JM 0212006 https://pubmed.ncbi.nlm.nih.gov/16918228/16918228 · pubmed ↗
- 4Inter- and intra-rater reliability of the Modified Ashworth Scale: a systematic review and meta-analysis Eur J Phys Rehabil Med Meseguer-Henarejos AB Sánchez-Meca J López-Pina JA Carles-Hernández R 5765905420182890111910.23736/S 1973-9087.17.04796-7 · doi ↗ · pubmed ↗
- 5Development and reliability of a system to classify gross motor function in children with cerebral palsy Dev Med Child Neurol Palisano R Rosenbaum P Walter S 214223391997918325810.1111/j.1469-8749.1997.tb 07414.x · doi ↗ · pubmed ↗
- 6Intrathecal baclofen versus selective dorsal rhizotomy for children with cerebral palsy who are nonambulant: a systematic review J Neurosurg Pediatr Davidson B Schoen N Sedighim S 69772520203162828610.3171/2019.8.PEDS 19282 · doi ↗ · pubmed ↗
- 7Effect of continuous intrathecal baclofen therapy in children: a systematic review Dev Med Child Neurol Buizer AI Martens BH van Ravenhorst CG 1281346120193018792110.1111/dmcn.14005 PMC 7379262 · doi ↗ · pubmed ↗
- 8Selective dorsal rhizotomy: an illustrated review of operative techniques J Neurosurg Pediatr Warsi NM Tailor J Coulter IC 5405472520203203294910.3171/2019.12.PEDS 19629 · doi ↗ · pubmed ↗