Schematic Assessment of Non-invasive Ventilation in Acute Respiratory Failure by Exploration of Paradigm Shift in Emergency Medicine
Aimen Suleman, Mohammad Sohailuddin, Mars Christian Aragon Sta Ines, Bilal Fattani, Ghulam Mustafa Meladi, Zahid Ullah Khan, Sana Ullah, Aneesa Khalid, Komal Zara

TL;DR
This study reviews the effectiveness of non-invasive ventilation in treating acute respiratory failure and finds it beneficial in both ICU and general ward settings.
Contribution
The study provides a meta-analysis of NIV efficacy in ARF, identifying failure predictors and treatment site effects.
Findings
NIV improved outcomes with a pooled odds ratio of 2.01 in treating ARF.
Success rates ranged from 55.6% to 72.1% across studies.
Failure predictors included elevated respiratory rate, CO₂ levels, and clinical scores like ROX and HACOR.
Abstract
Non-invasive ventilation (NIV) has gained attention as an important intervention for the treatment of acute respiratory failure (ARF) in both resource-constrained and non-intensive care unit (ICU) settings. Clinical outcomes and the efficacy and failure indicators of NIV treatment are still inconsistent across a wide range of research studies. This systematic review and meta-analysis evaluated the efficacy of NIV in ARF by looking at treatment site effects, failure predictor variables, together with aggregated outcomes. Following Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines, this study looked for pertinent research studies from 2000 to 2025 by employing PubMed, Scopus, Embase, and Cochrane Library databases. Adult patients who met the inclusion criteria received NIV treatment for ARF. The random-effects method calculated odds ratio pools…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
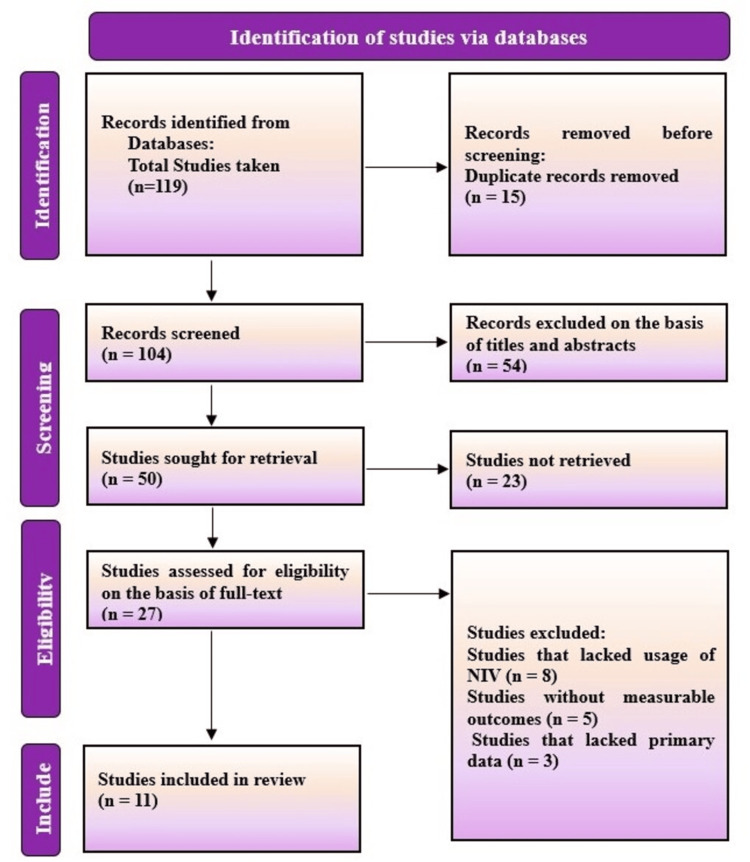 Figure 1
Figure 1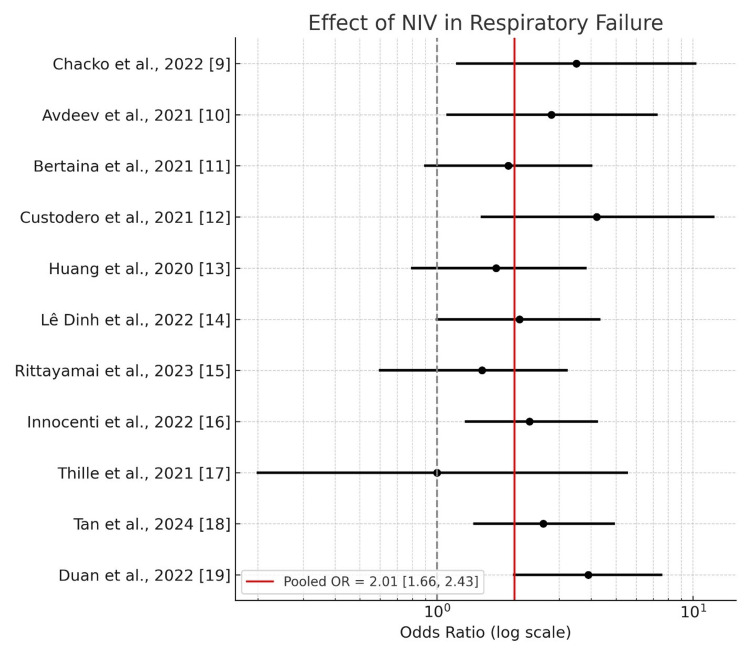 Figure 2
Figure 2| Author & Year | Study Design | Sample Size | Duration of NIV | Outcomes | Key Findings | Risk of Bias Assessment |
| Chacko et al., 2022 [ | Prospective cohort | 286 | Median 5 days (IQR 3–8); success: 6 days, failure: 4 days | NIV success: 63.6%; failure: 36.4%; overall mortality: 30.1% | NIV effective in resource-limited settings; failure associated with illness severity and systemic complications | Low–moderate; prospective design, possible selection bias, no randomization |
| Avdeev et al., 2021 [ | Retrospective cohort | 61 | Median 3.0 days (failure) vs 8.0 days (success), p=0.003 | NIV success: 72.1%; failure: 27.9%; mortality among intubated: 88% | NIV feasible outside ICU; failure predicted by age, high RR, D-dimer, CO₂ levels | Moderate; retrospective, small sample size, single region, detailed clinical data |
| Bertaina et al., 2021 [ | Multicenter registry-based subanalysis | 390 | Not explicitly stated; cross-sectional snapshot | NIV success: 55.6%; failure: 44.4% (mortality 37.7%, intubation 15.9%) | NIV beneficial in overburdened settings; early failure recognition critical | Moderate; registry-based, variable protocols, large diverse sample |
| Custodero et al., 2021 [ | Retrospective observational | 231 | Not explicitly stated | In-hospital mortality, NIV failure | MPI score predicted both mortality and NIV failure; cutoff ≥0.84 = 70.5% accuracy | Moderate; single-center, retrospective design |
| Huang et al., 2020 [ | Retrospective population-based (claims data) | 17,273 (NIV: 1,201; IMV: 16,072) | First episode only (2000–2012) | NIV vs IMV use characteristics and mortality trends | NIV use increased 733% (2000–2012); associated with age, comorbidities, cancer, COPD | Moderate; claims data limitations, potential unmeasured confounding |
| Lê Dinh et al., 2022 [ | Secondary analysis of prospective cohort | 389 | First 24 hours in ICU | NIV failure, sleep quality, ICU outcomes | Poor sleep and short duration linked to higher NIV failure; no impact on mortality or LOS | Low–moderate; large multicenter cohort, secondary analysis |
| Rittayamai et al., 2023 [ | Prospective cohort | 86 | ≥24 hours in general medical ward | NIV failure at 48 hours, hospital mortality | NIV safe/effective in general wards; SOFA score and male gender linked with failure; hospital mortality: 12.8% | Moderate; well-structured prospective study, small sample |
| Innocenti et al., 2022 [ | Retrospective cohort | 135 | Mean 9.1 ± 5.9 days | NIV failure, in-hospital mortality | HACOR and ROX scores predicted NIV failure/mortality; strongest accuracy from Day 0 onward | Moderate; retrospective, robust index-based analysis |
| Thille et al., 2021 [ | Post-hoc analysis of RCT | 146 (NIV: 84; HFNC: 62) | Median 12 h (IQR 4–27) | 28-day mortality, reintubation rate | NIV reduced mortality in hypercapnic patients (3% vs 31%); no difference in overall mortality | Low–moderate; post-hoc but based on RCT with strict criteria |
| Tan et al., 2024 [ | Randomized controlled non-inferiority trial | 225 (HFNC: 113; NIV: 112) | Minimum 2 h initially, then intermittent | Treatment failure, intubation, 28-day mortality | HFNC not non-inferior to NIV; higher failure (25.7%) and intubation rates (14.2%) | Low; RCT with clear endpoints and defined protocols |
| Duan et al., 2022 [ | Secondary analysis of prospective observational study | 1,286 | Not directly reported; data at 1–2, 12, 24 h | NIV failure prediction using ROX index | ROX index moderately effective in predicting NIV failure; early low scores highly predictive | Moderate; large multicenter cohort with multivariate modeling |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory Support and Mechanisms · Cardiac Arrest and Resuscitation · Sepsis Diagnosis and Treatment
Introduction and background
The medical condition known as acute respiratory failure (ARF) contributes significantly to worldwide morbidity and mortality; therefore, it requires prompt respiratory intervention [1]. Traditional treatment of severe ARF through invasive mechanical ventilation (IMV) exposes patients to three significant risks: ventilator-associated pneumonia, barotrauma, and an extended ICU hospitalization period [2]. Healthcare facilities face challenges with limited ICU beds and escalating respiratory infections, as shown during COVID-19 times, so healthcare professionals are exploring non-invasive ventilation (NIV) as a possible solution [3]. NIV gives respiratory support through a mask-like interface without requiring invasive endotracheal intubation. NIV treatments began with treating patients with COPD and cardiac-induced pulmonary edema and now serve patients experiencing hypoxemic respiratory failure alongside these original patient groups [4].
The literature contains multiple assessments of NIV effectiveness, but they demonstrate variability across different clinical situations. The results differ depending on whether patients receive treatment in the ICU or the general ward [5]. The patient properties and protocol standards of each facility also determine the outcome. Survival rates benefit from moving patients to IMV preemptively, using indicators including elevated respiratory rate, together with high CO₂ levels and the HACOR and ROX scores. Research validity remains unclear because the consistency of results between studies and their settings remains not fully revealed [6].
This study reviewed existing evidence about NIV treatment of ARF to present data about treatment effects while identifying warning signs for treatment failure and their practical implications. The research review included randomized trials as well as observational studies, which demonstrated both controlled experimental findings and real-world evidence.
Review
Methodology
This review followed the PRISMA 2020 protocol [7]. The literature research involved four databases, namely PubMed, Scopus, Embase, and the Cochrane Library, to retrieve studies from 2000 to 2024. The research strategy utilized multiple search terms, which included “non-invasive ventilation” and its abbreviations, in combination with “acute respiratory failure”, “intubation,” and “mortality.” A manual search of references from relevant reviews was conducted in order to find more studies. The research study included only original reports based on randomized controlled trials and observational studies that evaluated NIV as a main treatment method for people who suffered from ARF and provided measurements of NIV success, failure, intubation, or mortality rates. The research excluded pediatric studies and non-original data, such as reviews, together with results that did not measure outcomes regarding NIV effectiveness.
The data extraction process was conducted independently by two review authors. The research team collected data concerning the author/date, research design, study population, NIV length of treatment, success and mortality metrics, and key findings. Two reviewers reached an agreement on all conflicting points with the help of a third colleague who acted as an arbitrator. The assessment of study quality, along with its risk of bias, occurred through the utilization of the Cochrane Risk of Bias Tool (Version 2; www.cochrane.org) for RCTs and the Newcastle-Ottawa Scale (Version 2011) for observational studies. The authors classified each contributing study into three categories of bias levels: low, moderate, and high.
The authors conducted a meta-analysis using a random-effects model where the data were appropriate. The evaluation utilized odds ratios (ORs) with their accompanying 95% confidence intervals (CIs) for calculating treatment effects. Where the initial values were not odds ratios, researchers generated OR calculations based on risk ratios and area under the curve (AUCs) whenever possible. The I² statistic determined the study heterogeneity levels [8]. The methodology approach provided a clear synthesis of evidence with consistent ways of data confirmation and helped researchers evaluate NIV effectiveness across diverse patient situations.
Results
The research evaluation included 20,312 patients through eleven eligible studies. Research studies consisted of two randomized controlled trials, three prospective cohorts, four retrospective cohorts, one registry-based analysis as well as a secondary analysis of a prospective cohort. The selected patients had ARF due to COPD exacerbations as well as pneumonia combined with undifferentiated hypoxemic respiratory failure. Figure 1 depicts the flow diagram for study selection, which followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines 2020.
PRISMA flow diagram demonstrating study schemePRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses
Throughout the study period, NIV's successful utilization rates ranged from 55.6% to 72.1%, while its failure rates ranged from 27.9% to 44.4%. When comparing NIV treatment to standard care, the analysis revealed that the combined odds of positive NIV results are 2.01 (95% CI: 1.66-2.43).
The mortality rate increases significantly when patients require intubation after failing NIV. Several studies have found broad signs that NIV treatment would not work. Clinical indicators showed that patients with high respiratory rates, elevated D-dimer, CO₂ retention, and poor sleep quality had poor outcomes. The heart rate, acidosis, consciousness, oxygenation, and respiratory rate (HACOR) index demonstrated efficacy in identifying administration failure in the early NIV period and was created by combining heart rate, acidosis, oxygenation levels, and respiratory rate with consciousness scores. In order to identify early failure during NIV, the same result used data from the ROX index, which combines SpO₂/FiO₂ with respiratory rate. NIV treatment was effective in a variety of clinical settings.
Through research, the viability and safety of non-ICU NIV were established. RCT results demonstrated that NIV successfully surpassed the high-flow nasal cannula (HFNC) for reducing treatment failure and intubation requirements. Due to retrospective methods and study sample limitations, the majority of research was at moderate risk of bias; however, two randomized controlled trials showed low vulnerability to bias. The characteristics of selected studies along with risk of bias assessment is shown in Table 1.
Figure 2 forest plot shows odds ratios along with their 95% confidence intervals, which were taken from 11 research studies that investigated Non Invasive Ventilation-based outcomes for patients experiencing respiratory failure. The selected studies had added one relevant effect size measurement to the analysis. Estimates from risk ratios and area under the curve (AUC) values were used to derive odds ratios when original studies did not have OR.
Forest plot showing the effect of non-invasive ventilation (NIV) in respiratory failure across selected studies
Discussion
The systematic analysis supported the expanding utilization of NIV for ARF management, which showed both excellent outcomes and better applicability throughout healthcare institutions. The research data showed that NIV was a successful enhancer in patient outcomes when compared to both IMV and standard oxygen therapy delivery because its combined odds ratio reached 2.01. This study offered significant insights into the use of NIV in the management of acute respiratory failure (ARF). One is that NIV continues to be a useful treatment outside of the intensive care unit. Research conducted in emergency rooms, general medical wards, as well as in environments with limited resources, yielded results comparable to those of NIV applications in intensive care units. The findings were particularly important for low- and middle-income nations and for medical emergencies that drain intensive care unit resources [20].
This review's findings showed that medical practitioners need to identify NIV failure as soon as treatment begins. Before starting NIV, the clinical examination should incorporate assessments that include predictive factors like elevated respiration rates and hypercapnia with inflammatory markers. For predicting NIV failure, the ROX and the HACOR clinical scoring systems were found to be reliable instruments [21]. One study demonstrated that the HACOR scoring parameter improved its ability to predict treatment failure with the passage of time. In one study, the researchers found that a higher MPI score accurately predicted both patient mortality outcomes and NIV failure [22]. The use of randomized trials in this evaluation improved the body of evidence. Another trial's results showed that NIV and HFNC had different failure rates, but these results made NIV the first-choice approach for certain ARF conditions. According to clinical trials, patients with hypercapnia who received NIV had a lower 28-day mortality rate than those who received HFNC, according to a similar study [23].
Although the results showed promise, doctors should proceed with caution. Inconsistent study methodologies and retrospective research applied performance constraints that limited the possibility of a wide interpretation [24]. Information about particular patient variables, such as adherence rates, interface types, and real-time monitoring practices, was not provided by research that relied primarily on administrative data. Predictive solutions and warning systems that initiate the switch from NIV to IMV at crucial moments should be incorporated into medical practice. Improved non-invasive ventilation deployment across various settings is achieved through the combination of standardized protocols and training for multiple healthcare providers [25].
These findings had solid practice-based support thanks to the inclusion of real clinical data and trial evidence. In order to validate findings across a range of societal groups and management systems, future research endeavors must create improved risk assessment tools, then investigate comprehensive long-term NIV impacts while conducting RCTs in multiple healthcare facilities.
Conclusions
Non-invasive ventilation (NIV) is an effective treatment for acute respiratory failure that results in lower rates of intubation and related mortality. While scoring systems like ROX and HACOR aid in identifying impending failure, the therapy yields positive results in a variety of treatment settings outside of intensive care units. The implementation of NIV in larger patient populations is supported by numerous consistent research findings. Clinical scoring systems with early patient escalation protocols must be used when NIV implementation is expanded. Future research must improve our capacity to select appropriate patients for NIV therapy and create performance-based NIV treatment strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and epidemiology of acute respiratory failure Crit Care Clin Chen L Rackley CR 2212334020243843269310.1016/j.ccc.2023.12.001 · doi ↗ · pubmed ↗
- 2Incidence, risk factors and outcome of barotrauma in mechanically ventilated patients Intensive Care Med Anzueto A Frutos-Vivar F Esteban A 6126193020041499109010.1007/s 00134-004-2187-7 · doi ↗ · pubmed ↗
- 3Mechanical ventilation for COVID-19 patients Semin Respir Crit Care Med Brioni M Meli A Grasselli G 4054164320223543983110.1055/s-0042-1744305 · doi ↗ · pubmed ↗
- 4Non-invasive positive pressure ventilation for acute cardiogenic pulmonary edema and chronic obstructive pulmonary disease in prehospital and emergency settings Cureus Abubacker AP Ndakotsu A Chawla HV 013202110.7759/cureus.15624 PMC 827709234277241 · doi ↗ · pubmed ↗
- 5Non-invasive ventilation versus invasive weaning in critically ill adults: a systematic review and meta-analysis Thorax Burns KE Stevenson J Laird M 7527617720223471628210.1136/thoraxjnl-2021-216993 · doi ↗ · pubmed ↗
- 6Longitudinal assessment of ROX and HACOR scores to predict non-invasive ventilation failure in patients with SARS-Co V-2 pneumonia J Crit Care Med (Targu Mures) Anand A Kodamanchili ST Joshi A 1471571020243910927110.2478/jccm-2024-0013 PMC 11193952 · doi ↗ · pubmed ↗
- 7The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 0372202110.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗
- 8Meta-analysis in clinical trials revisited Contemp Clin Trials Der Simonian R Laird N 1391454520152634374510.1016/j.cct.2015.09.002PMC 4639420 · doi ↗ · pubmed ↗