Perinatal Exercise and Cardiovascular Disease Risk
Marnie K. McLean, Bradley J. Petek, Lidija McGrath, Emily McGill, Abbi D. Lane

TL;DR
This review explores how perinatal exercise can reduce cardiovascular disease risk by addressing traditional and nontraditional risk factors during pregnancy and beyond.
Contribution
The paper highlights gaps in evidence for subgroup-specific exercise recommendations and emerging associations with pregnancy-specific CVD risk factors.
Findings
Perinatal exercise is recommended to combat traditional CVD risk factors like gestational weight gain and high blood pressure.
Emerging data suggest perinatal exercise may improve nontraditional risk factors such as sleep and depression.
More research is needed on pregnancy-specific factors like placental characteristics and long-term cardiovascular outcomes.
Abstract
The purpose of this narrative review was to summarize perinatal exercise guidelines and associations of perinatal physical activity and/or exercise with cardiovascular disease (CVD) risk. Observational studies, randomized controlled trials, systematic reviews, and meta-analyses were included. Gaps in literature and suggestions for future studies were identified. Despite concordant international guidelines, data to support nuanced activity advice for some subgroups are limited. Perinatal physical activity and exercise are consistently recommended to combat traditional CVD risk factors during the perinatal period, like excessive gestational weight gain, high blood pressure, and high blood glucose. Physical activity and exercise appear to improve nontraditional risk factors such as poor sleep and depression. Data are emerging regarding associations with some pregnancy-specific factors,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
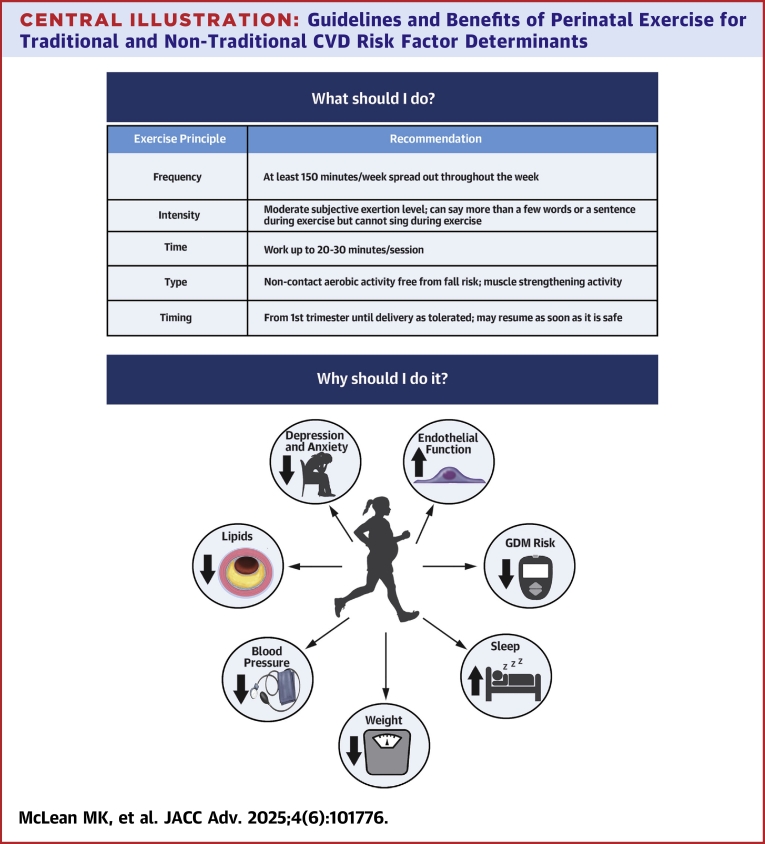 Figure 1
Figure 1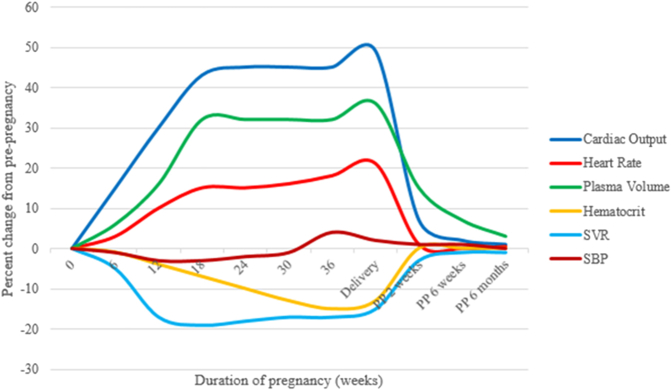 Figure 2
Figure 2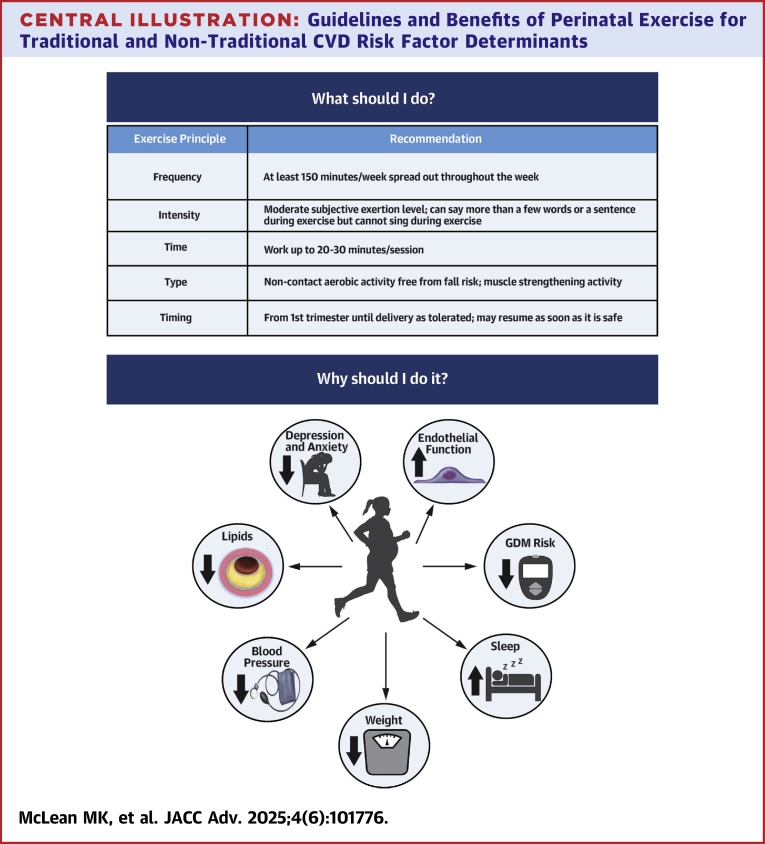 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBirth, Development, and Health · Obesity, Physical Activity, Diet · Gestational Diabetes Research and Management
Pregnancy is a cardiometabolic challenge.1 Even in uncomplicated pregnancies, individuals become more insulin resistant, and cholesterol levels increase.2 Hemodynamic adaptations occur: increased cardiac output, heart rate, plasma volume, and red blood cell mass, along with decreased systemic vascular resistance and hematocrit (Figure 1).1 Normotensive pregnancy is characterized by a small, transient fluctuations in systolic blood pressure (BP) (Figure 1).3 Impaired hemodynamic adaptations may represent unmasking of pre-existing subclinical cardiovascular dysfunction and/or an independent process that contributes to long-term complications.3 Compared to other developed nations, maternal morbidity and mortality rates in the United States are high and rising, reaching 23.8 deaths/100,000 live births in 2020.4 Cardiovascular conditions are the leading cause of maternal mortality, accounting for >25% of all pregnancy-related deaths.5 Reasons include more women entering pregnancy with risk factors, poor access to healthcare, and unfavorable social determinants of health.4^,^5Figure 1Hemodynamic Adaptations to PregnancyAdapted from Yucel et al.3
Evidence unequivocally demonstrates that regular exercise can prevent and/or treat adverse cardiometabolic conditions in many populations.6 Physical activity (PA) or exercise is associated with lower risk of novel and traditional cardiovascular disease (CVD) risk factors in the perinatal period,6 including adverse pregnancy outcomes (APOs) (hypertensive disorders of pregnancy [HDPs], gestational diabetes [GDMs], preterm birth, small-for-gestational-age deliveries).7^,^8 Offspring of individuals who exercise during pregnancy have better cardiovascular health, body composition, and nervous system development, with benefits extending into childhood.9
The goal of this narrative review is to synthesize literature related to perinatal PA/exercise, including national guidelines and effects of perinatal exercise on short- and long-term maternal CVD risk. This paper refers to PA as “any bodily movement resulting in energy expenditure,” while exercise is defined as “a subset of PA that is structured, repetitive, and aimed at maintaining or improving physical fitness.”10
Methods
Studies published in English were identified in PubMed and Google Scholar databases. Search terms included “pregnancy,” “pregnant,” “postpartum,” “perinatal,” “cardiovascular disease,” “risk factors,” “blood pressure,” “glucose,” “lipids,” “cholesterol,” “obesity,” “BMI,” “smoking,” “arterial stiffness,” “endothelial function,” “autonomic function,” “Flt-1,” “sleep,” “diet,” “inflammation,” “placenta/l,” “mood,” “anxiety,” “depression,” “exercise,” and “physical activity.” Observational studies, randomized controlled trials, systematic reviews, and meta-analyses were screened. When consensus statements, systematic reviews, and/or meta-analyses were found, conclusions were included. Results from individual studies were included if they specifically addressed the risk factor of interest and were conducted in a large or specific population or were one of the few existing studies related to a particular risk factor.
Perinatal exercise and PA recommendations worldwide
The benefits of exercise for reducing CVD risk are well described.11 Although benefits are clear, many individuals of reproductive age do not meet national PA guidelines including 150 min/wk or 500 MET·min/wk of moderate-vigorous aerobic activity and muscle-strengthening activities,6 and PA is frequently reduced during pregnancy and parenting.12
Current American College of Obstetrics and Gynecology guidelines
The American College of Obstetrics and Gynecology (ACOG) guidelines were updated in 2020 (Table 1).13 Previously, organizations recommended maintaining heart rates under specific levels (eg, 140 beats/min) due to wellbeing concerns.15 Guidelines now suggest using a subjective measure, the rating of perceived exertion (RPE), to monitor intensity as heart rate changes significantly during pregnancy.13 The RPE scale describes the individual's perception of physical work.16 Moderate-intensity exercise should elicit an RPE of 13 to 14 on the 6 to 20 scale, or “somewhat hard.”13^,^16 ACOG guidelines provide information about exercise frequency, type, intensity, and some information on duration.13 Musculoskeletal adaptations and injuries, as well as lower back, hip, leg, and foot pain are common17 and require consideration when prescribing perinatal exercise. Individualized or dynamic exercise prescriptions may be needed due to changes in body habitus and pre-existing or newly acquired comorbidities.13Table 1. Detailed Summary of PA and Exercise Guidelines During Pregnancy and PostpartumExercise PrincipleRecommendationRed FlagsFrequency150 min spread out throughout the week for aerobic exercise; no specific dosing in guideline statements for resistance exercise; nonconsecutive days are recommended for resistance training in nonpregnant populations
- •Vaginal bleeding
- •Abdominal pain
- •Regular painful contractions
- •Amniotic fluid leakage
- •Dyspnea before exertion
- •Dizziness/lightheadedness
- •Headache
- •Chest pain, pressure, or tightness
- •Muscle weakness or fatigue affecting balance
- •Calf or extremity pain or swelling IntensityModerate subjective exertion level of 12-14 on Borg Scale; <60%-80% of max effort; can say more than a few words or a sentence at a time during exercise but could not sing during exercise;Can continue vigorous activity if vigorous activity was performed prior to pregnancy;Moderate intensity resistance training characterized by >8 repetitions to volitional fatigue per setTimeWork up to 30-60 min/session; Can begin with shorter durations until >20-30 min is possibleTypeNon-contact aerobic training free from fall risk; resistance training including bands, bodyweight, or weights; pelvic floor exercisesEnvironment & safetyThermoneutral and preferably supervised setting; ensure hydration; avoid lying on back during pregnancy; avoid Valsalva maneuver during resistance training; avoid hypoglycemia; empty breasts before exercising if lactatingTimingFrom first trimester until delivery as tolerated; may resume as soon as it is safe; consult a healthcare provider after complicated birth or c-sectionAdapted from ACOG Committee Opinion, Number 804, National PA Guidelines, and the 2023 AHA Resistance Training Scientific Statement.6^,^13^,^14 Exercise physiology principles can be applied to the perinatal population for exercise prescription. Special considerations and red flags contraindicating exercise or necessitating exercise termination are included. Pregnant people should consult with a health care provider before beginning exercise. Hypoglycemia can be avoided by limiting the intensity or duration (<45 min) of exercise sessions and/or by consuming adequate calories before exercise.
Current ACOG guideline gaps
While resistance exercise is recommended, specific exercise prescription information is lacking in ACOG guidelines.13 For discussion of ACOG guidelines for patient subgroups and other guideline gaps, please see the Supplemental Appendix.
Global guidelines
Many countries developed their own perinatal exercise recommendations.18 While generally concordant, guidelines do not always have comprehensive exercise prescription recommendations (Table 2). A 2017 review reported prenatal walking, stationary cycling, aerobic exercises, dancing, resistance exercises, stretching exercises, hydrotherapy, and water aerobics have all been extensively studied and were safe and beneficial.19 Authors concluded that all pregnant individuals without a contraindication should engage in regular PA and exercise.19 Meta-analyses reported that women of normal weight (n = 2,059) who engage in aerobic exercise experience 49% lower incidence of GDM (2.9% vs 5.6%; relative risk: 0.51; 95% CI: 0.31-0.82) and 79% lower incidence of HDPs (1.0% vs 5.6%; relative risk: 0.21; 95% CI: 0.09-0.45).20Table 2. Summary of Perinatal PA and Exercise Guideline Components by CountryCountryFrequency Days/WeekIntensityDurationTypePrior Activity LevelSBWDAEREInactiveActiveAustralia✓✓✓✓✓✓✓✓Austria✓✓✓✓✓✓✓Belgium✓✓✓✓✓✓✓Brazil✓✓✓✓Brunei✓✓✓✓✓✓✓Canada✓✓✓✓✓✓✓Chile✓✓✓✓✓Cyprus✓✓✓✓✓Denmark✓✓✓✓✓✓Estonia✓✓✓✓✓Fiji✓✓✓✓Finland✓✓✓✓✓✓✓France✓✓✓✓✓✓Greece✓✓✓Iceland✓✓✓✓✓Kenya✓✓✓✓Latvia✓✓✓Malaysia✓✓✓✓✓NZ✓✓✓✓✓✓✓Norway✓✓✓✓Portugal✓✓✓Qatar✓✓✓✓✓✓✓Singapore✓✓✓✓✓✓✓Slovenia✓✓✓✓✓Spain✓✓✓✓✓✓✓Sri Lanka✓✓✓✓Switzerland✓✓✓✓✓✓UK✓✓✓✓USA✓✓✓✓✓✓Uruguay✓✓✓✓✓About half countries provide a weekly while half provide a daily exercise volume recommendation. Most countries provide frequency and intensity guidance. About half countries provide guidance on aerobic and resistance exercises. Most countries provide information regarding inactive people who become pregnant, with less information given for active women. Guidelines on sedentary behavior are provided in less than half the guidelines.Adapted from Hayman et al.18AE = aerobic exercise; D = daily; NZ = New Zealand; RE = resistance exercise; SB = sedentary behavior; UK = United Kingdom; USA = United States of America; W = weekly.
Pregnancy PA or exercise and CVD risk factor determinants during pregnancy and after delivery
Studies evaluated associations of perinatal exercise/PA and CVD risk factors. Summaries according to individual risk factors are found below with general effects shown in Table 3.Table 3. Perinatal Exercise and Traditional and Novel CVD Risk Factor DeterminantsRisk Factor DeterminantInfluence of Perinatal PA or ExerciseTraditional CVD risk factor determinants Blood pressure↓ SBP, ↓DBP21 Glucose↓ Fasting blood glucose, ↓ risk of GDM22 Obesity↓ Risk of excessive GWG, ↓ postpartum weight retention23 Body composition↑ Improved maternal and fetal body composition↓ Maternal fat mass,24 ↓ fetal fat mass25 Lipid profile↑ Improved maternal LDL and triglyceride levels26^,^27Novel CVD risk factor determinants APOs↓ Risk of APOs, PE, GDM, LBW, PTB19 Sleep↑ Improved sleep quality28^,^67 Depression and anxiety↓ Risk of PPD13 Cardiorespiratory fitness↑ Fitness13 and ↓HDP29 Inflammation↓ C-reactive protein30, 31, 32 Arterial stiffness↔/? Pulse wave velocity33 Endothelial function↑ Endothelial-dependent dilation34 Cardiac autonomic control↓ Heart rate, ↑ HRV35^,^36 Lactation↔ Breastmilk composition, volume, infant growth37APO = adverse pregnancy outcomes; CVD = cardiovascular disease; DBP = diastolic blood pressure; GDM = gestational diabetes mellitus; GWG = gestational weight gain; HDP = hypertensive disorders of pregnancy; HRV = heart rate variability; LBW = low birth weight; LDL = low-density lipoprotein cholesterol; PA = physical activity; PE = preeclampsia; PPD = postpartum depression; PTB = preterm birth; SBP = systolic blood pressure. ↑ = higher with exercise, ↔ = similar with PA/exercise, ↓ = decreased with PA or exercise.
Traditional CVD risk factor determinants
Blood pressure
According to a recent meta-analysis, exercise during pregnancy can lower systolic and diastolic BP by about 2-3 mm Hg (systolic: −3.19, 95% CI: −5.13 to −1.25 mm Hg; diastolic: −2.14, 95% CI: −4.26 to −0.03 mm Hg).21 Systolic BP was 7.5 mm Hg (95% CI: 1.5-12.6, P = 0.013) lower following a 12-week uphill walking exercise intervention in normotensive participants.38 This finding is important; even moderately elevated prenatal BP is associated with higher risk of hypertension years after delivery.39
Pregnant individuals at high risk of HDP had a smaller increase in systolic and diastolic BP from week 14 to 34 of pregnancy with a walking intervention; the mean systolic BP increase was 1.81 ± 2.40 mm Hg in walking group vs 9.87 ± 2.87 mm Hg in control group (P = 0.03).40 Regular PA during pregnancy appears to help prevent HDP and assist with management and severity in those diagnosed.7^,^40 Benefits are seen in individuals who do and do not exercise prior to becoming pregnant.13 PA prior to and during early pregnancy were associated with reductions in preeclampsia risk between 20% and 35%, with the greatest reductions seen in those engaged in PA prior to pregnancy (relative risk: 0.65; 95% CI: 0.47-0.89).41 Authors hypothesized that PA before and during early pregnancy could protect against hypertensive APOs due to improved placentation.41 The greatest benefits of PA were observed with 5 to 6 hours per week of exercise.41 This volume of PA is much greater than current guidelines for nonpregnant and pregnant adults.6
Less is known regarding the influence of prenatal PA or exercise on BP after delivery. An observational study reported that greater moderate-to-vigorous physical activity throughout pregnancy was linked to better BP in the first weeks after delivery.42 A sub-analysis of a trial that began in early pregnancy and focused on preventing excessive gestational weight gain (GWG) by counseling participants to eat healthfully and be more active found no effect of the intervention on BP patterns from early pregnancy to 12 months postpartum.43
Glucose
Performing high amounts of exercise (760 MET·min/wk) in early pregnancy–mid-second trimester was associated with a decrease of 3.9 mg/dL in glucose (95% CI: −7.4 to −0.5 mg/dL) compared with low exercise levels.22 According to a systematic review investigating associations between prenatal exercise and blood glucose, women with diabetes can improve fasting blood glucose following chronic exercise training (mean difference: −2.76 mg/dL, 95% CI: −3.18 to −2.34 mg/dL), an effect not observed in women free from diabetes (mean difference: −0.05 mg/dL, 95% CI: −0.16 to 0.05 mg/dL), although quality of evidence was “low.”44
GDM is a carbohydrate intolerance first observed during pregnancy and is associated with greater risk of hypertensive APOs, including gestational hypertension and preeclampsia.45 GDM is associated with higher lifetime risk of developing cardiometabolic diseases (CMDs).46 PA is linked to a lower risk of GDM, and National PA Guidelines recommend PA/exercise to help prevent GDM.6^,^10 Once GDM is diagnosed, lifestyle modification, including moderate exercise, is recommended for first-line management.45 Lifestyle modification, including increasing PA, was one of the few strategies identified for combating excess CMD risk after GDM in a recent review.47
Body mass index
Increases in body mass index do not always completely reverse after delivery, predisposing individuals to risk of obesity.48 The Institute of Medicine sets pregnancy weight gain goals based on pre-pregnancy body mass index to optimize pregnancy outcomes,49 yet only 30% to 40% of women gain the recommended amount of weight.50 Excessive GWG and postpartum weight retention are associated with excess CMD risk in individuals who did and did not have GDM.51^,^52 Historically, there was concern that prenatal exercise increases risk of inadequate GWG; these fears have been refuted.13
National PA Guidelines and others concluded that prenatal/perinatal exercise lowered odds of excessive GWG and promoted better postpartum weight, especially when combined with healthy diet.10^,^23 ACOG recommends obesity management prior to pregnancy, as even small weight reductions may improve pregnancy outcomes.53 A randomized controlled trial that began in early pregnancy among individuals who were overweight or obese prior to pregnancy counseled participants to eat healthfully and be more active demonstrated mildly favorable or null effects of the intervention on GWG depending on race and weight at study entry.54 However, the same study found postpartum weight outcomes were better in the intervention group: intervention participants retained 3.6 kg less weight (95% CI: −5.5 to −1.8 kg) at 6 months postpartum and 2.4 kg less weight (95% CI: −4.3 to −0.5 kg) at 12 months postpartum. At 6 months postpartum, overweight-intervention participants retained 4.1 kg less weight (95% CI: −6.7 to −1.5 kg), and obese intervention participants retained 3.3 kg less weight (95% CI: −5.8 to −0.7 kg) than control groups of the same weight status.55
Smoking
Pregnancy has been identified as an ideal time to intervene on smoking behaviors as pregnant women tend to have increased access to healthcare and may be motivated by fetal well-being.56 Health behaviors often cluster; PA interventions may have off-target effects on smoking. However, lifestyle interventions have not demonstrated consistent benefits on smoking cessation or relapse prevention in postpartum women.57 Studies that utilized a PA intervention as a smoking-cessation treatment have not been effective, although better PA quantification is needed.58
Diet
PA + nutrition interventions are recommended to combat obesity around the perinatal period.53 These combined interventions have had mixed effects on other pregnancy-specific CVD risk factors: GDM, excessive GWG, BP, APOs, and postpartum weight retention.43
Lipids
During pregnancy, cholesterol levels can increase by 50% to 70%.59 High maternal cholesterol levels during pregnancy may be associated with risk of CVD in offspring.60 Maternal dyslipidemia is associated with multiple APOs.61 Maternal lipid levels were improved with prenatal exercise (low-density lipoprotein levels mean change: −8 mg/dL, 95% CI: −3 to −29 mg/dL, P < 0.001) and triglycerides (mean change: −6 mg/dL, 95% CI: −1 to −11 mg/dL, P = 0.03)22^,^26^,^27 with nonsignificant improvements or no benefits seen with postpartum exercise in lactating women.62^,^63
Novel CVD risk factor determinants
Sleep
Poor sleep is an independent risk factor for CVD.64 Pregnancy has been associated with sleep disturbances and lower sleep quality.65 Greater sleep disturbances were directly associated with higher odds of preeclampsia (odds ratio [OR]: 2.80, 95% CI: 2.38-3.30), HDP (OR: 1.74, 95% CI: 1.54-1.97), GDM (OR: 1.59, 95% CI: 1.45-1.76), preterm birth (OR: 1.38, 95% CI: 1.26-1.51), and stillbirth (OR: 1.25, 95% CI: 1.08-1.45**)**.66 Exercise improves perinatal sleep, especially when initiated during early pregnancy,28 with improvements in sleep quality detected in a meta-analysis (OR: 6.21, 95% CI: 2.02-19.11, P = 0.001).67
Depression and anxiety
Depression and anxiety are strong CVD risk factors, especially for women.68 Depression and anxiety affect about 12% of pregnant and postpartum women.69^,^70 Exercise/PA can lower postpartum depression symptoms.6^,^71
Placental characteristics
Inadequate placental formation and vascularization is a seminal event in the pathogenesis of multiple APOs.72 Pan-vascular adaptations to exercise, including reduced inflammation and improved angiogenesis, may benefit placental development.73 Maternal exercise during pregnancy may influence placentation or placental characteristics.73 Pathological features, such as malperfusion lesions, have been associated with APOs and subclinical CVD after delivery.74^,^75
Better placental growth, volume, and function have been described in women who began or continued vigorous exercise (running) during pregnancy vs women who did not.76 A recent study found no association of moderate-to-vigorous physical activity with placental malperfusion lesions, but results were limited by the convenience sample that included only 50 individuals with medically indicated placental pathology examinations.42 Soluble FMS-like tyrosine-kinase-1 is a placenta-derived angiogenic inhibitor that is elevated in preeclampsia.77 Individuals in a national, diverse sample who were meeting PA guidelines had lower soluble FMS-like tyrosine-kinase-1 levels in the first trimester (846.3 pg/mL, 95% CI: 821.6-871.8) vs those who did not meet PA guidelines (893.0 pg/mL, 95% CI: 864.5-922.5, P < 0.017), potentially indicating a role for the placenta in the utility of PA for combating preeclampsia.78
Lactation
Lactation (dichotomous or dose-dependent) leads to both short- and long-term CMD risk-factor-determinant improvements, like insulin sensitivity, hypertension, lipid profiles, and glucose levels; is associated with 25% to 47% lower diabetes risk through late middle age; and is associated with lower lifetime CVD risk (HR: 0.89, 95% CI: 0.83-0.95).79^,^80 Individuals affected by APOs may be less likely to lactate due to multiple biological and logistical factors, such as delayed lactogenesis or infant neonatal intensive care unit admission.81^,^82 With appropriate caloric intake, breastmilk volume and composition and infant growth are not influenced by moderate exercise.37 A recent national cohort study found that Black and White parous individuals who both lactated for ≥3 months during reproductive years and performed above average amounts of PA throughout adulthood had lower CMD risk scores in late middle age, suggesting joint (and not overlapping) effects of lactation and PA in adulthood.83
Arterial stiffness
Arterial stiffness is independently associated with CVD in people with and without hypertension.84 High arterial stiffness may be associated with greater risk of preeclampsia.85 Increases in arterial stiffness during pregnancy tend to normalize 7 weeks postpartum in most cases but may continue following delivery in women with preeclampsia, enhancing CVD risk later in life.86 A recent study concluded that aerobic exercise initiated after the first trimester in low-risk pregnancies does not appear to influence pregnancy-induced vascular adaptations, including arterial stiffness.33
Endothelial function
Endothelial function is enhanced during pregnancy, perhaps due to greater shear stress in arteries and higher circulating blood volume.87 Fetal growth restriction and HDP are often characterized by endothelial dysfunction.87 Regular exercise training can improve endothelial function in healthy pregnant individuals.34
Autonomic balance
Lower baroreflex sensitivity may be associated with greater risk of HDP.88 Higher than expected increases in resting heart rate may be associated with greater risk of HDP.88 Lower heart rate variability may be an important risk marker for HDP, suggesting sympathovagal imbalance may play a role in the etiology of HDP.88
A prospective study of 139 women reported higher beat-to-beat BP variability in every trimester in individuals who developed preeclampsia (systolic: first: 4.8 ± 1.3 vs 3.7 ± 1.2 mm Hg, P = 0.001; second: 5.1 ± 1.8 vs 3.8 ± 1.1 mm Hg, P = 0.02; third: 5.2 ± 0.8 vs 4.0 ± 1.1 mm Hg, P = 0.002; diastolic: first: 3.1 ± 0.9 vs 2.5 ± 0.7 mm Hg, P = 0.02; second: 3.0 ± 0.8 vs 2.5 ± 0.5 mm Hg, P = 0.007; third: 3.5 ± 1.3 vs 2.5 ± 0.8 mm Hg, P = 0.04).35 Elevated first trimester systolic beat-to-beat BP variability was associated with preeclampsia after statistical adjustment, OR: 1.94, 95% CI: 1.27-2.99.35 Sympathetic activity during pregnancy was improved in a recent, small trial of pregnant individuals who began aerobic exercise.36
Inflammation
In individuals who go on to develop some APOs, higher inflammation may be detectable early in pregnancy yet do not appear to pre-date pregnancy.89^,^90 C-reactive protein was lower in active (n = 16) vs inactive (n = 16) women with obesity (inactive: 9.1 ± 4.0 mg/L vs active: 6.3 ± 2.5 mg/L, P = 0.02).30 Women at risk of GDM enrolled in an exercise intervention (n = 84) or control group (n = 87) who maintained their exercise had a decrease in CRP while those who reduced their exercise had an increase in CRP (decreased PA: +0.09 mg/dL, 95% CI: −0.14 to 0.33; maintained PA: −0.08 mg/dL, 95% CI: −0.23 to 0.08, P < 0.05).31 Light PA was negatively and significantly correlated with maternal C-reactive protein (light PA: r = −0.40, P = 0.01, moderate PA: r = −0.18, P = 0.21).32
Future directions to improve understanding of perinatal exercise and CVD risk
Areas in need of investigation are described in Table 4. Participation in perinatal exercise or PA is low. Effective, low-cost, perinatal exercise/PA promotion strategies are needed. Although entering pregnancy with an established exercise routine would be ideal, many US pregnancies are unplanned.92 Just-in-time interventions supporting the adoption and upkeep of exercise programs immediately before, during, and after pregnancy are critical. Given the role of social determinants of health in CVD risk and PA/exercise participation, perinatal exercise strategies must be tailored and adapted for individuals across a broad range of social and economic strata.Table 4. Areas in Need of ResearchGaps in Research Informing RecommendationsSignificance and Suggestions for Future StudiesTiming and dosing strategiesOptimal timing and dosing of the PA or exercise (pre-pregnancy, mid-pregnancy, or postpartum) are unknown. Some association studies concluded that prepregnancy or early pregnancy exercise/PA is especially helpful.41 Specific guidelines for return to exercise and fitness progression postpartum in athletes are lacking.Resistance training exercise programsData are sparse regarding the use of perinatal resistance training on CVD risk. Resistance training alone can improve multiple CVD risk factors in the general population14 and might be more feasible for pregnant individuals, especially in late pregnancy or early postpartum when aerobic exercise might be less comfortable.Gaps in research regarding relationships with perinatal exercise Placental featuresWhether perinatal exercise influences placental formation or function is not well defined. The use of more sensitive indicators of placental function and large, unbiased samples might better identify the optimal dose and timing of exercise/PA for placental health. LactationRecent evidence suggests joint rather than overlapping effects of PA/exercise and lactation on cardiometabolic disease (CMD) risk.83 Whether PA must be performed before, during, or after lactation to mitigate later life cardiometabolic risk is unknown. Arterial stiffnessArterial stiffness is independently associated with CVD.84 Data regarding associations of perinatal exercise with arterial stiffness during and after pregnancy are extremely limited. Sedentary behaviorSedentary behavior is a CVD risk factor. Preliminary data reveled that high sedentary behavior is a risk factor for APOs.91 Detailed recommendations regarding total amounts and consideration of sedentary behavior volume in relation to PA volume do not exist.
Conclusions
PA and exercise are recommended for pregnant and postpartum individuals without contraindications, have beneficial effects on CVD risk during and after pregnancy, and do not adversely influence infant growth or breastmilk (Central Illustration).10^,^93 Granular levels of information regarding optimal types, timing, doses, progression, and adoption and adherence strategies are sparser than those in the general nonpregnant population.6 More nuanced guidelines for prescribing and monitoring PA in individuals entering pregnancy or postpartum with CVD/CMD should be developed. Overlapping or interactive effects of exercise/PA with perinatal-specific factors linked to long-term CVD/CMD risk, such as placental development and lactation, need more investigation. Trials utilizing behavior change strategies and technologies should be tested in this population.Central IllustrationGuidelines and Benefits of Perinatal Exercise for Traditional and Non-Traditional CVD Risk Factor DeterminantsCreated with BioRender.
Funding support and author disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sanghavi M.Rutherford J.D.Cardiovascular physiology of pregnancy Circulation 13020141003100810.1161/CIRCULATIONAHA.114.00902925223771 · doi ↗ · pubmed ↗
- 2Berggren E.K.Presley L.Amini S.B.Hauguel-de Mouzon S.Catalano P.M.Are the metabolic changes of pregnancy reversible in the first year postpartum?Diabetologia 582015156115682595777710.1007/s 00125-015-3604-x PMC 4703315 · doi ↗ · pubmed ↗
- 3Yucel E.De Faria Y.D.Pregnancy in women with congenital heart disease Curr Treat Options Cardiovasc Med 192017732882874310.1007/s 11936-017-0572-0 · doi ↗ · pubmed ↗
- 4Wang S.Rexrode K.M.Florio A.A.Rich-Edwards J.W.Chavarro J.E.Maternal mortality in the United States: trends and opportunities for prevention Annu Rev Med 7420231992163670674610.1146/annurev-med-042921-123851 · doi ↗ · pubmed ↗
- 5American College of Obstetricians Gynecologists' Presidential Task Force on Pregnancy Heart Disease Committee on Practice Bulletins—Obstetrics ACOG Practice Bulletin No. 212: pregnancy and heart disease Obstet Gynecol 1332019 e 320e 35610.1097/AOG.000000000000324331022123 · doi ↗ · pubmed ↗
- 6Piercy K.L.Troiano R.P.Ballard R.M.The physical activity guidelines for Americans Jama 3202018202020283041847110.1001/jama.2018.14854 PMC 9582631 · doi ↗ · pubmed ↗
- 7Gavard J.A.Artal R.Effect of exercise on pregnancy outcome Clin Obstet Gynecol 5120084674801846347510.1097/GRF.0b 013e 31816 feb 1d · doi ↗ · pubmed ↗
- 8Magee L.A.Smith G.N.Bloch C.Guideline no. 426: hypertensive disorders of pregnancy: diagnosis, prediction, prevention, and management J Obstet Gynaecol Can 4420225475713557742610.1016/j.jogc.2022.03.002 · doi ↗ · pubmed ↗